“Previously … CDC developed tests for emerging pathogens and then shared those tests with others, and then after that, commercial labs would develop their own tests,” Shah told CNN. “That process took time. Now with these new arrangements, commercial labs will be developing new tests for public health responses alongside CDC, not after CDC.”
In a news release announcing the contract, ARUP Laboratories also characterized the move as a shift for the agency.
“The new contract formalizes ARUP’s relationship with the CDC,” said Benjamin Bradley, MD, PhD, medical director of the ARUP Institute for Research and Innovation in Infectious Disease Genomic Technologies, High Consequence Pathogen Response, Virology, and Molecular Infectious Diseases. “We continue to expand our capabilities to address public health crises and are prepared to scale up testing for H5N1, or develop other tests quickly, should the need arise.”
“To be clear, we have no evidence so far that this [bird flu] virus can easily infect human beings or that it can spread between human beings easily in a sustained fashion,” Jennifer Nuzzo, DrPH (above), Director of the Pandemic Center and Professor of Epidemiology at Brown University School of Public Health, told CNN. “If it did have those abilities, we would be in a pandemic.” Clinical laboratory leaders will recall the challenges at the CDC as it developed its SARS-CoV-2 test early in the COVID-19 pandemic. (Photo copyright: Brown University.)
Missouri Case Raises Concerns
The first human infection of HPAI was reported in late March following a farmer’s “exposure to dairy cows presumably infected with bird flu,” the CDC stated in its June 3, 2024, bird flu Situation Summary. That followed confirmation by the USDA’s Animal and Plant Health Inspection Service (APHIS) of an HPAI outbreak in commercial poultry flocks in February 2022, and the CDC’s confirmation of the first known infections in dairy herds reported on March 25, 2024.
Concerns about the outbreak were heightened in September following news that a person in Missouri had been infected with the virus despite having no known contact with infected animals. CNN reported that it was the 14th human case in the US this year, but all previous cases were in farm workers known to be exposed to infected dairy cattle or poultry.
In a news release, the Missouri Department of Health and Senior Services (DHSS) revealed that the patient, who was not identified, was hospitalized on Aug. 22. This person had “underlying medical conditions,” DHSS reported, and has since recovered and was sent home. Both DHSS and the CDC conducted tests to determine that the virus was the H5 subtype, the news release states.
At present, the CDC states that the public health risk from the virus is low. However, public health experts are concerned that risks could rise as the weather gets cooler, creating opportunities for the virus to mutate “since both cows and other flu viruses will be on the move,” CNN reported.
Concerns over CDC Testing and FDA Oversight
In the months immediately following the first human case of the bird flu virus, Nuzzo was among several public health experts sounding an alarm about the country’s ability to ramp up testing in the face of new pathogens.
“We’re flying blind,” she told KFF Health News in June, due to an inability to track infections in farmworkers. At that time, tests had been distributed to approximately 100 public health labs, but Nuzzo and other experts noted that doctors typically order tests from commercial laboratories and universities.
KFF reported that one diagnostics company, Neelyx Labs, ran into obstacles as it tried to license the CDC’s bird flu test. Founder, CEO, and lead scientist Shyam Saladi, PhD, told KFF that the federal agency had promised to cooperate by facilitating a license and a “right to reference” CDC data when applying for FDA authorization but was slow to come through.
While acknowledging the need for testing accuracy, Greninger contended that the CDC was prioritizing caution over speed, as it did in the early days of the COVID-19 pandemic. “The CDC should be trying to open this up to labs with national reach and a good reputation,” he told KFF.
Another problem, KFF reported, related to the FDA’s new oversight of laboratory developed tests (LDTs), which is causing labs to move cautiously in developing their own tests.
Jennifer Nuzzo, DrPH (above), Director of the Pandemic Center and Professor of Epidemiology at the Brown University School of Public Health co-authored a June 2024 analysis in Health Affairs that called on the CDC to develop “a better testing playbook for biological emergencies.” The authors’ analysis cited earlier problems with the responses to the COVID-19 and mpox (formerly known as monkeypox) outbreaks.
If global surveillance networks have detected a novel pathogen, the authors advise, the US should gather information and “begin examining the existing testing landscape” within the first 48 hours.
Once the pathogen is detected in the US, they continued, FDA-authorized tests should be distributed to public health laboratories and the CDC’s Laboratory Response Network (LRN) laboratories within 48 hours.
Advocates of this approach suggest that within the first week diagnostics manufacturers should begin developing their own tests and the federal government should begin working with commercial labs. Then, within the first month, commercial laboratories should be using FDA-authorized tests to provide “high throughput capacity.”
This may be good advice. Experts in the clinical laboratory and healthcare professions believe there needs to be improvement in how novel tests are developed and made available as novel infectious agents are identified.
Patients outside the US wait even longer to see healthcare specialists with some appointments scheduled a year out in the Canadian province of Nova Scotia
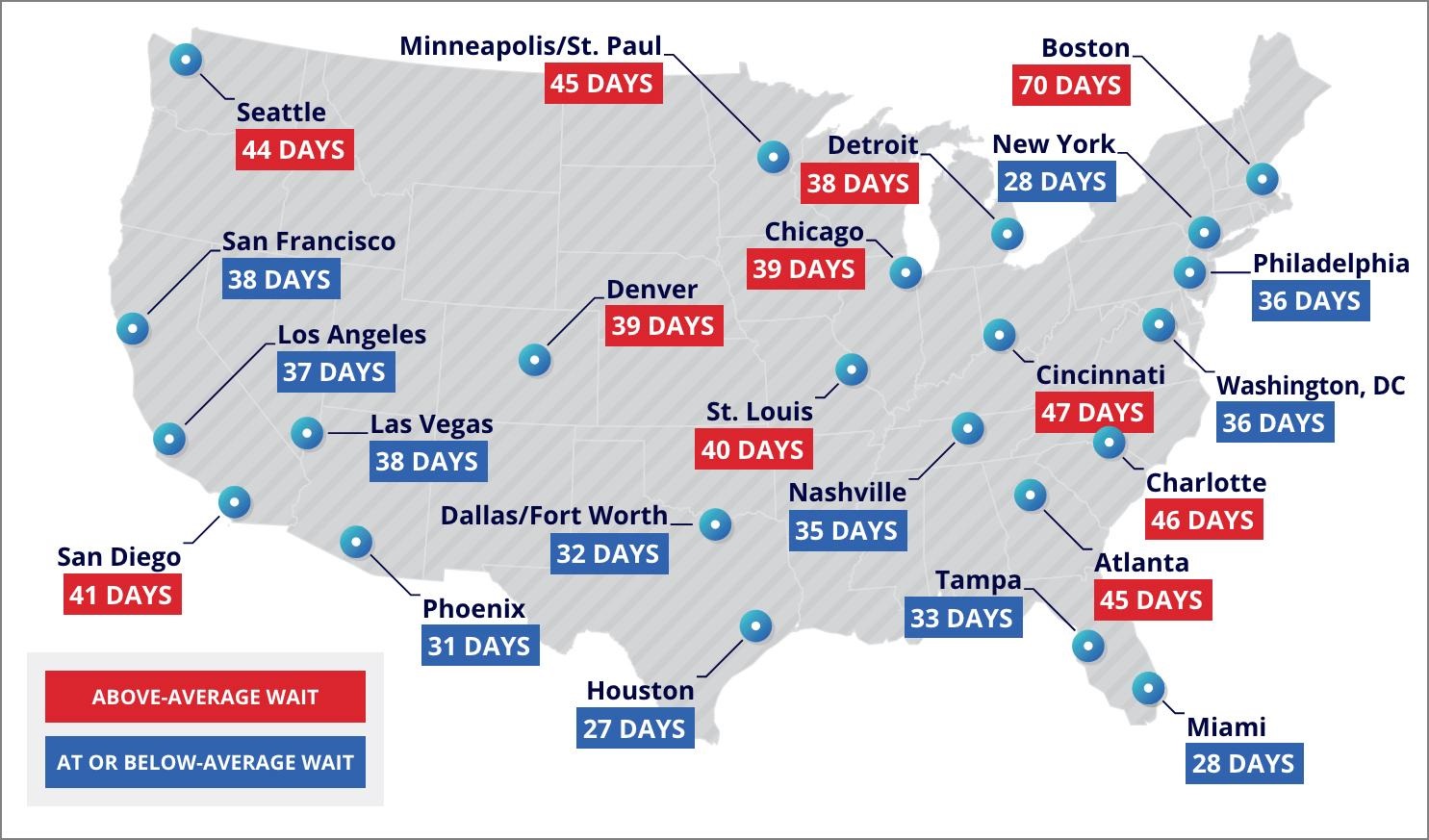
Data recently released by healthcare consulting firm ECG Management Consultants (ECG) reveals that patients in the United States wait an average of 38 days for healthcare appointments. That figure is a significant stretch from the desired industry standard of 14-day or less wait times, according to Becker’s Hospital Review.
Clinical laboratories serve the needs of physicians who see patients and refer testing needed by patients to labs. Thus, average wait times should be of interest to lab professionals who strive to meet reporting turnaround times for lab test results, particularly given the unique way that ECG conducted its survey of patient wait times.
In “The Waiting Game: New-Patient Appointment Access for US Physicians,” ECG wrote, “Adopting a ‘secret shopper’ approach, we put ourselves in the shoes of the average patient trying to book an appointment. We contacted nearly 4,000 physician practices in 23 major cities across the US, posing as a new, commercially insured patient seeking care for general, nonemergent conditions that typically don’t require a physician referral.”
ECG’s study provides “a realistic view of where and in what specialties patients face the most significant challenges to accessing routine care,” the authors wrote in their published report. The report also includes patients’ appointment-keeping behavior based on length of wait times.
“Consumer expectations have evolved significantly in all industries. From buying a plane ticket to making a restaurant reservation, the consumer experience has been highly optimized and customers in turn have become accustomed to information and services being available at their fingertips. They bring the same expectations about speed and convenience to healthcare,” the researchers explained.
ECG pointed out that when patients are required to wait 14 days or more to see their physicians, no shows and cancellations increase dramatically.
“Numerous studies have shown that patients are significantly less likely to show up for appointments that are scheduled further out,” the study authors noted.
“One of the takeaways was how difficult the patient experience is. Not only did our secret shoppers have to go out and find physicians, they had to sit on the phone sometimes on very long holds and go through multiple barriers and jump through hoops,” Jennifer Moody (above), partner with ECG Management Consultants and one of the authors of the study, told Becker’s Hospital Review. “Even in that case, they weren’t successful in scheduling appointments with all the practices they called. I think of the average consumer who might be having a similar experience,” she added. Lengthy wait times are not believed to be an issue when patients need clinical laboratory tests. (Photo copyright: ECG Management Consultants.)
Getting Authentic Results
To gather the study data, ECG distributed its secret shoppers throughout 23 major US cities, reaching almost 4,000 physician practices (between 145-168 per city) to schedule appointments for non-emergency conditions not needing a physical referral.
The researchers gathered wait times for TNAAs (third next available appointments), a common metric. They chose TNAAs because first and second appointments often produce unclear results due to extenuating circumstances or late cancellations, Becker’s Hospital Review reported.
The researchers recorded TNAAs for the following specialties:
Cardiology (39 days),
Dermatology (40 days),
Family medicine (29 days),
Gastroenterology (48 days),
General surgery (22 days),
Neurology (63 days),
Obstetrics/gynecology (37 days),
Ophthalmology (37 days),
Orthopedic surgery (20 days),
Pediatrics (24 days), and,
Rheumatology (68 days).
They found the average wait time to be 38 days. And “of the 253 metropolitan market and specialty combinations included in this research, only 6% had an average wait time of 14 days or less,” Becker’s reported.
The researchers omitted the physician practices that were unable to either take or return calls, take messages, or provide a hold time under five minutes to give the secret shopper an answer, Becker’s added.
Jennifer Moody, Partner, ECG Management Consultants, one of the authors of the study, “was particularly surprised by the portion of callers who never even made it to the stage of learning about wait times. Out of 3,712 physician practices, callers were able to secure responses from only 3,079, meaning nearly one in five physician practices could not provide appointment availability information,” Becker’s reported.
The lowest average wait time in all specialties was 27 days in Houston, and the longest was 70 days in Boston. “A key takeaway from the report is that physician concentration does not guarantee timely access, as a major healthcare hub like Boston helps illustrate,” Becker’s noted, adding that physicians in such areas may “devote time to teaching or research over appointments.”
The graphic above, taken from ECG’s published report, shows the average TNAA times recorded by their secret shoppers at medical specialty practices in major cities across the US. (Graphic copyright: ECG Management Consultants.)
Other Country’s Wait Times
Healthcare systems outside the US struggle with patient wait times as well. Forbes reported that patients of Canada’s public health system “faced a median wait of 27.7 weeks for medically necessary treatment from a specialist after being referred by a general practitioner. That’s over six months—the longest ever recorded.”
Patients in Nova Scotia wait even longer. There they “face a median wait of 56.7 weeks—more than a year—for specialist treatment following referral by a general practitioner. Those on Prince Edward Island are also in the year-long waiting club—a median of just over 55 weeks,” Forbes noted.
And in the UK, a recent survey found that “more than 150,000 patients had to wait a day in A&E [accident and emergency] before getting a hospital bed last year, according to new data,” with the majority of those patients over the age of 65, according to The Guardian.
ECG suggestions that may reduce wait times include:
Adopt automation and self-service tools in an “easily navigable platform” that enables patients to schedule appointments 24/7.
Ensure healthcare providers are “utilized appropriately and at the top of their license.”
Address inequities in access to healthcare regardless of patients’ location or socioeconomic status.
There is more in the ECG report that hospitals—as well as clinical laboratories—can use to reduce patient wait times to see care providers. As the authors wrote, “For patients, the first step of the care journey shouldn’t be the hardest.”
New technique could allow emergency responders to determine severity of LVO stroke while patient is still in the ambulance
Researchers at Brigham and Women’s Hospital in Massachusetts say they have developed a clinical laboratory test that can quickly determine whether a patient is experiencing one of the deadliest types of strokes, known as an ischemiclarge vessel occlusion (LVO) stroke. The development team believes this new assay could be deployed as a point-of-care test to enable faster diagnosis of stroke events.
The test combines measurement of two blood plasma biomarkers with an established clinical score used by clinicians and EMS personnel to assess stroke severity. Compared with current approaches, their technique more accurately differentiates LVO strokes from other types of strokes, making it more likely that patients receive appropriate treatment in a timely manner, the researchers said in a Brigham news release.
Dark Daily has long predicted that advances in technology and computing power would make it possible for pathologists and clinical laboratory scientists to combine multiple established biomarkers (individually not associated with the disease state targeted) with other clinical and patient data to create the ability to make an accurate and earlier diagnosis.
Ultimately, Brigham’s research could “aid in the development of a point‐of‐care diagnostic test capable of guiding prehospital LVO stroke triage,” wrote Joshua Bernstock, MD, PhD, Clinical Fellow in Neurosurgery at Brigham and Women’s Hospital, lead author of the study, and colleagues.
“We have developed a game-changing, accessible tool that could help ensure that more people suffering from stroke are in the right place at the right time to receive critical, life-restoring care,” said Joshua Bernstock, MD, PhD (above), Clinical Fellow in Neurosurgery at Brigham and Women’s Hospital and lead author of the Brigham study that developed the clinical laboratory test that the researchers say can enable emergency caregivers to determine quickly and accurately if a patient is having an ischemic large vessel occlusion (LVO) stroke. (Photo copyright: Brigham and Women’s Hospital.)
Early Identification of LVO Stroke
As explained in the news release, an LVO stroke is a type of ischemic stroke caused by obstruction in a major brain artery. The researchers noted that LVO strokes account for “62% of poststroke disabilities and 96% of poststroke death.”
These strokes are readily treatable using endovascular thrombectomy (EVT), in which the blockages are surgically removed, the news release note. However, the researchers observed that EVT “requires specialized teams and equipment, limiting its availability to comprehensive stroke centers and other EVT‐capable centers.”
This can lead to delays as patients are transferred to those facilities, worsening outcomes and increasing the risk of death, the researchers wrote in Stroke: Vascular and Interventional Neurology. So, early identification of LVO stroke is key to ensuring patients receive timely treatment.
Identifying False Negatives/Positives
One challenge, the news release notes, is that brain bleeds (hemorrhagic stroke) can present similar symptoms, yet require “vastly different” treatment.
“A growing body of work has, therefore, evaluated prehospital stroke assessment scales in an effort to identify LVO strokes in the field,” the researchers wrote. “However, such severity scales lack the sensitivity and specificity required for triaging LVO patients with confidence, resulting in false negatives in patients with LVO as well as false positives in patients with stroke mimics or hemorrhagic stroke.”
As explained by EMS Aware, these assessment scales, such as FAST-ED (field assessment stroke triage for emergency destination) and RACE (rapid arterial occlusion evaluation), attempt to determine the severity of a stroke by assigning scores based on symptoms such as facial palsy, arm weakness, and speech difficulties.
To develop their test, Bernstock and colleagues proposed combining the scales with measurement of two blood proteins:
In their study, they attempted to validate cutoff values for the biomarkers and scales.
To do so, the researchers analyzed data from 323 patients admitted to a Florida hospital with suspected stroke between May 2021 and August 2022. Each was assigned to one of four diagnostic categories based on clinical data from their medical records, which included results of computed tomography (CT scan) or magnetic resonance angiography (MRA). The diagnostic categories included:
The patients were assessed using five stroke severity scales. The researchers used frozen blood samples from the patients to measure the biomarkers. They then used this data to determine the likelihood of LVO stroke and compared the results with the diagnoses as determined by the clinical data.
“Combinations of the blood biomarkers with the scales FAST‐ED or RACE showed the best performance for LVO detection, with a specificity of 94% (for either scale combination) and a sensitivity of 71% for both scales,” the researchers wrote.
Sensitivity was higher in patients who presented within the first six hours from onset of symptoms.
“Critically, application of the biomarker and stroke scale algorithms ruled out all patients with hemorrhage,” the researchers wrote. However, they also suggested that their algorithm could be adjusted to enable early identification of hemorrhagic stroke.
The researchers noted that they chose biomarker cutoffs to maximize specificity, so “a certain number of LVOs are missed. However, as such patients default into ‘standard‐of‐care’ triaging pathways, such a decision is unlikely to represent much clinical risk.”
Testing in the Field
The Brigham researchers used established biological biomarkers combined with modern computing—in combination with the scores from a field assessment test—to develop their new clinical laboratory test that identifies the type of stroke.
Their next step is to carry out “another prospective trial to measure the test’s performance when used in an ambulance,” the news release states. “They have also designed an interventional trial that leverages the technology to expedite the triage of stroke patients by having them bypass standard imaging and move directly to intervention.”
“In stroke care, time is brain,” Bernstock said. “The sooner a patient is put on the right care pathway, the better they are going to do. Whether that means ruling out bleeds or ruling in something that needs an intervention, being able to do this in a prehospital setting with the technology that we built is going to be truly transformative.”
More research and clinical studies are needed. However, the fact that the Brigham team wants to deploy this approach in ambulances is an indication that there is high clinical value from this approach.
Clinical pathologists and medical laboratory managers will want to watch the ongoing development and deployment of this new assay, whether it is run in near-patient settings or core clinical laboratories in support of patients presenting in emergency departments.
Study found highest incidences of occupational carcinogenesis among clinical laboratory and histology technicians, followed by pathologists
It has been known for years that formalin (a form of formaldehyde used as a disinfectant and preservative in the handling of tissues samples in anatomy, pathology, and microbiology labs), as well as xylene and toluene, are dangerous to clinical laboratory workers. Nations around the world have taken steps to minimize exposure to these dangerous chemicals. However, a recent study in Iran found that those measures may not have gone far enough to protect histology and clinical laboratory technicians, pathologists, and medical laboratory scientists.
The study conducted by researchers in the Department of Occupational Health Engineering, School of Public Health, at Tehran University of Medical Sciences, showed that levels of exposure to these chemicals is still significantly higher than recommended, resulting in a higher risk for cancer among lab workers in Iran’s hospitals.
“Employing risk assessment techniques as a complementary tool in monitoring programs for respiratory exposure in the different work setting should be considered to protect the staffs against both non-cancerous and cancer-related hazards,” the study authors wrote.
Lessons learned from the Iranian hospital lab study could benefit clinical laboratory workers in US hospitals and help those who work with formaldehyde, toluene, and xylene worldwide to reduce their chances of developing a vascular condition known as Raynaud’s phenomenon (shown above) which can lead to necrosis and gangrene, as well as other dangerous health conditions affecting the lungs, brain, and other systems and organs in the body. (Photo copyright: Wikipedia.)
Study Details
The Iranian study considered the carcinogenic and non-carcinogenic impact of occupational exposure to formaldehyde in the pathology laboratories of four Tehran hospitals. The researchers “used a quantitative risk assessment method proposed by the United States Environmental Protection Agency (EPA), along with its provided database known as the Integrated Risk Information System (IRIS). Respiratory symptoms were assessed using the American Thoracic Society (ATS) questionnaire,” the study authors wrote in NatureScientific Reports.
The scientists found that “91.23% of exposure levels in occupational groups exceed the NIOSH [National Institute for Occupational Safety and Health] standard of 0.016 ppm.” They determined that “41.03% of all the studied subjects were in the definite carcinogenic risk range (LCR > 10−4), 23.08% were in the possible carcinogenic risk range (10−5 < LCR < 10−4), and 35.90% were in the negligible risk range (LCR < 10−6),” they wrote.
“The highest index of occupational carcinogenesis was observed in the group of lab technicians with a risk number of 3.7 × 10-4, followed by pathologists with a risk number of 1.7 × 10-4,” the scientists wrote. “Furthermore, 23.08% of the studied subjects were within the permitted health risk range (HQ < 1.0), while 76.92% were within the unhealthy risk range (HQ > 1.0),” they added.
“Formaldehyde exhibits high solubility in water and is rapidly absorbed by the nasal cavity, sinuses, throat, and mucous membrane of the upper respiratory tract upon exposure,” the study authors wrote. “Consequently, due to the elevated potential for both carcinogenic and non-carcinogenic formaldehyde exposure among pathology staff—particularly laboratory technicians—the implementation of management measures … becomes imperative to lower the exposure levels of all employees below permissible limits.”
Those management measures include:
“Strict guideline adherence and safe work protocols,
“Increasing staff numbers to decrease exposure duration,
“Adoption of engineering solutions such as localized ventilation systems, and
“Use of respiratory protective equipment during sample handling and tissue processing.”
Previous Reports on Exposure Risk to Clinical Lab Workers
The knowledge of the danger behind these chemicals isn’t new.
In 2017, a pathology lab in Auckland, New Zealand, lost its accreditation because formaldehyde levels were so high the lab had to be evacuated nearly every day, The New Zealand Herald reported.
“In epidemiological studies on industrial workers, pathologists and anatomists, the relationship between exposure to formaldehyde and an increased risk of various types of cancer including nasal cavity, nasopharynx, lung, brain, pancreas, prostate, colon and atopic lymphoma system has been determined,” the Iranian scientists wrote in Nature Scientific Reports.
Call for Stronger Regulations
“The Food and Drug Administration (FDA), the Consumer Product Safety Commission (CPSC), and the Environmental Protection Agency have expressed serious concern about the carcinogenicity of formaldehyde,” the Iranian scientists noted, adding that “the potential carcinogenic risk to humans has been studied in a number of cohort and case-control studies.”
There is room for more studies looking at the health effects of exposure to these chemicals among lab workers, as well as continued evaluation of the risks and preventative measures that could be taken. Perhaps tightened regulations will make its way to US labs, echoing more stringent ones of the European Union.
“It is imperative to implement control measures across various hospital departments to mitigate occupational formaldehyde exposure levels proactively. These findings can be valuable for policymakers in the health sector, aiding in the elimination or reduction of airborne formaldehyde exposure in work environments,” the Iranian scientists wrote.
Managers of histology and clinical laboratories may find useful advice in hospital laboratory studies like that coming out of Iran. Protecting the health of lab workers worldwide starts with reducing their exposure to deadly chemicals.
Trend will likely lead to physicians ordering more clinical laboratory screening tests for cancer among all age groups, including young patients
Upticks in colorectal cancer cases among younger populations, as reported in recent news stores, is an issue that has implications for clinical laboratories. According to a study conducted at the University of Missouri-Kansas City (UMKC), the number of colorectal cancer cases in the US has increased greatly since 1999 with the “most dramatic jumps” seen in children, teens, and young adults, a Digestive Disease Week (DDW) news release reported.
“Colorectal cancer is no longer considered just a disease of the elderly population,” said lead researcher Islam Mohamed, MD, an internal medicine resident physician at UMKC. “It’s important that the public is aware of signs and symptoms of colorectal cancer.”
The researchers noted in the DDW news release that “colorectal cancer cases, over about two decades, increased by 500% among children, ages 10 to 14; 333% in teens, ages 15 to 19; and 185% among young adults, ages 20 to 24.”
“[The results of the UMKC study] means that there is a trend. We don’t know what to make of it yet. It could be lifestyle factors or genetics, but there is a trend,” lead researcher Islam Mohamed, MD (above), Internal Medicine Resident, University of Missouri-Kansas City, told NBC News. If proved, this trend could lead to increased demand for clinical laboratory screening tests for colorectal and other cancers among young people. (Photo copyright: Digestive Disease Week.)
0.6/100,000 children ages 10 to 14 (a 500% increase).
1.3/100,000 teens ages 15 to 19 (a 333% increase).
Two/100,000 young adults ages 20 to 24 (a 185% increase).
Albeit small numbers, the cases are growing at a rate that is troublesome, according to experts. As NBC put it, “any increase can take on a larger significance” when rates begin at low points.
The study also found incidence of colorectal cancer up in people in their 30s and 40s, reaching by 2020:
6.5/100,000 people ages 30 to 34 (a 71% increase).
11.7/100,000 people ages 35 to 39 (a 58% increase).
20/100,000 people ages 40 to 44 (a 37% increase).
Screening Guidelines May Need to Change
Further research based on UMKC’s study findings could lead to changes in cancer screening guidelines.
“We were screening people from the age of 60 for colon cancer. This has now been lowered to 55, and that is due to be lowered again to 50 over the next few months,” Jude Tidbury, RN, nurse endoscopist and clinical nurse specialist, gastroenterology and endoscopy, at the UK’s East Sussex Healthcare NHS Trust, told Healthline.
In the US, the American Cancer Society advises people of average risk for cancer to start screening for colorectal cancer at age 45. The test options ACS recommends annually include:
What is behind early-onset colorectal cancer among certain age groups? An international study led by Fred Hutchinson Cancer Center (Fred Hutch), Seattle, found “strong correlations” with consuming alcohol and being obese with early-onset colorectal cancer in adults under age 50, according to a news release.
The researchers set out to explore the common genetic variants and causal modifiable risk factors that are behind early-onset colorectal cancer, according to a paper they published in the journal Annals of Oncology.
To do so they used big databases, pulling out 6,176 early-onset colorectal cancer cases and 65,829 controls from sources including:
They focused on “lifestyle factors increasing risk” by comparing the genetic variations in those with colorectal cancer to healthy people, the Fred Hutch news release explained.
“It’s important to see that alcohol and obesity are linked to early-onset colorectal cancer. Also, insulin signaling and infection-related biological pathways. These are all really important to understand—it’s helping us to develop interventions,” said Ulrike Peters, PhD, Professor and Associate Director, Public Health Services Division, Fred Hutch, who co-led the research, in the news release.
Peters noted future research may aim to address data gaps relating to racial and ethnic groups.
More Colorectal Cancer Tests
As studies continue to explore the notion that cancer may not be a disease of aging,
clinical laboratories could see more primary care physicians and healthcare consumers using colorectal cancer screening tests, which require analysis and reporting by labs.
Medical laboratory leaders may want to proactively encourage lab sales and service representatives to educate physician office staff about using the lab’s available resources for screening young adults for colorectal cancer.
Clinical laboratories with mobile phlebotomy programs are positioned to benefit as demand for at-home blood draws increases
Hospital-at-Home (HaH) models of remote healthcare continue to pick up speed. The latest example comes from the 793-bed Mass General Brigham (MGB) health system which partnered with Best Buy Health to build the largest HaH program in the nation, according to Becker’s Hospital Review. This means clinical laboratories will have new opportunities to provide mobile phlebotomy home-draw services for MGB’s HaH patients.
“The health system now has a capacity for acute hospital care at home of 70 patients and is currently treating about 50 to 60 a day. The goal is to move to 10% of Mass General Brigham’s overall capacity, or about 200 to 300 patients,” Becker’s reported.
Best Buy Health provides MGB’s Home Hospital patients with computer tablets and Internet access, Becker’s noted.
“Healthcare is fragmented, the technology doesn’t always connect. Technology is our expertise,” said Chemu Lang’at, COO, Best Buy Health, during the WMIF presentation.
The hospital is the most expensive site of care in the US healthcare industry. Thus, preventing patients from needing to be hospitalized—or treating them in their homes—could reduce the cost of care considerably for both patients and multihospital systems.
“It’s been estimated that 30% of inpatient care will move to the home in the next five years, representing $82 billion in revenue. This is a tremendous opportunity,” said Heather O’Sullivan, MS, RN, A-GNP, Mass General Brigham’s President of Healthcare at Home, during MGB’s presentation at the World Medical Innovation Forum in September, according to Becker’s Hospital Review. MGB’s HaH program offers clinical laboratories with new opportunities to provide mobile phlebotomy services to the health system’s Hospital-at-Home patients. (Photo copyright: Mass General Brigham.)
Hospital-at-Home
Proponents of HaH call it a “sustainable, innovative, and next-generation healthcare model. [It is] person-centered medical care that keeps patients out of the hospital, away from possible complications, and on to better outcomes,” RamaOnHealthcare reported.
Some of the biggest payoffs of HaH include:
• Cost Savings: Anne Klibanski, MD, President and CEO, MGB, described the HaH program as “a way the health system could stay afloat and thrive amid financial challenges affecting the industry, with lower costs and better outcomes for patients at home,” Becker’s Hospital Review reported.
• Increased Capacity: Having an HaH program can help alleviate bed shortages by treating many conditions in patient’s homes rather than in the ER. “The program … typically treats patients with conditions like COPD flare-ups, heart failure exacerbations, acute infections and complex cellulitis,” Becker’s reported.
“It’s not typically comfortable to be cared for in the emergency room,” said O’Neil Britton, MD, MGB’s Chief Integration Officer, at WMIF.
• Decreased Staff Exhaustion: “Clinicians have described getting an extra level of joy from treating patients at home,” said Jatin Dave, MD, CMO, MassHealth, at WMIF. He added that this could provide one solution to healthcare burnout, Becker’s noted.
• Lab Connection: Clinical laboratories have the opportunity to meet the need for mobile phlebotomists to draw blood specimens from HaH patients in their homes.
• Patient Satisfaction: “The data suggests that for populations studied in multiple areas, [HaH] is a safe service with high-quality care, low readmission rates, low escalation rates, low infection rates and—bottom line—patients love it.” Adam Groff, MD, co-founder of Maribel Health, told RamaOnHealthcare.
HaH Program Going Forward
Britton told the WMIF audience that MGB hopes to “expand the program for surgery, oncology, and pain management patients, recently admitting its first colorectal surgery patient,” Becker’s reported.
However, the future of MGB’s HaH program is not assured. “The Centers for Medicare and Medicaid Services (CMS) waiver to provide acute hospital care at home expires at the end of 2024. A bill to extend the program recently passed a House committee,” Becker’s reported.
Dave said at WMIF that he “hopes the home will one day provide a ‘single infrastructure’ for all levels of care: from primary to inpatient care to skilled nursing,” Becker’s Hospital Review noted, adding, “The home is where, in the long run, we can have this full continuum.”
Overall, this can be a snapshot of where the HaH movement in the US is currently at, with the Mass General Brigham example showing that this mode of healthcare is delivering results and helping patients. Clinical laboratories across the nation should track efforts by hospitals and health systems in their areas to establish and expand hospital-at-home programs.