Survey respondents specifically mentioned clinical laboratory charges as part of the balance billing they were receiving
Unexpected medical bills—which often include clinical laboratory test and pathology charges—are still arriving in patients’ mailboxes, even though the federal No Surprises Act (H.R.3630) was passed as part of the Consolidated Appropriations Act, 2021 specifically to prevent that from happening.
According to a survey conducted by Morning Consult, a global research firm with offices in New York, Washington, D.C., and San Francisco, 20% of patients said they or a family member received an unexpected medical bill in 2022.
Notably, survey respondents specifically mentioned charges for clinical laboratory testing as part of the unanticipated balance billing they received.
“Adults who received unexpected bills this year were most likely to get them for in-network lab work that was sent to an out-of-network lab for assessment, which is covered under the law, or for testing or procedures not covered by insurance, which isn’t,” a Morning Consult news release noted.
Morning Consult polled more than 2,000 adults between June 22 and June 24, 2022, according to the published results.
“The No Surprises Act ended the practice of surprise medical billing in most circumstances, providing relief for millions of patients who faced surprise medical bills they did not expect,” said Matt Eyles (above), President/CEO, America’s Health Insurance Plans, in an AHIP news release. “But more work needs to be done,” he added. Clinical laboratory managers should be aware of the federal law before balance billing their patients. (Photo copyright: Business Wire.)
When the Law Works, and When It Does Not
In “Judge Vacates Provision in No Surprises Act,” Dark Daily’s sister publication, The Dark Report, explained that the No Surprises Act aims to protect insured individuals from receiving unexpected medical bills for unanticipated emergency care or services—including clinical lab tests—that they unknowingly received from out-of-network providers.
However, certain provisions of the law can counteract its intention.
“[The No Surprises Act] doesn’t apply if a patient goes to his or her own primary care physician, or another doctor in the community, and that doctor sends that patient to an out-of-network laboratory,” healthcare attorney Charles Dunham IV, a shareholder at law firm Greenberg Traurig LLP in Houston, told The Dark Report. “In general, it applies to emergency services or a non-emergency service where the patient is in an inpatient or outpatient setting in a hospital that’s in network, and they utilize a lab that’s out of network.”
Bills for Lab Tests, Other Services Surprise Patients
Healthcare services cited by the most respondents to the Morning Consult survey that resulted in unexpected medical bills include:
Testing or procedures not covered by insurance, 34%.
Lab work at an in-network hospital or healthcare facility that was sent to an out-of-network lab for assessment, 32%.
Treatment by an out-of-network physician or specialist at an in-network hospital or healthcare facility, 21%.
Treatment at an out-of-network hospital or healthcare facility, 19%.
Transportation to an emergency department by an out-of-network ambulance, 18%.
Clinical laboratory testing was at the top of the unexpected charges, which were typically more than $1,000, according to 22% of those who received balance billing.
Could Billing Disputes Escalate?
Anatomic pathology practices, medical laboratories, and other providers who fail to comply with the No Surprises Act may be at risk. And, unfortunately, a Health Care Cost Institute study in 2020 found pathologists second only to emergency medicine physicians as specialists who most often bill for out-of-network hospital charges, according to a Dark Daily e-briefing.
“It’s possible providers continuing to send patients bills that violate the No Surprises Act may be targeted by the U.S. Department of Justice at some future time, even several years from now. So, there is risk,” said Robert Michel, Editor-in-Chief of Dark Daily and The Dark Report.
“Also, patients who realize that bills they received from healthcare providers were in violation of the No Surprises Act could potentially file class action lawsuits against those providers,” Michel added.
In fact, 63% of those surveyed by Morning Consult expressed confidence in their ability to address a surprise bill they deemed illegal. Thus, healthcare providers, clinical laboratory leaders, and pathology group managers are advised to brush up their understanding of the federal ban on certain types of balance billing.
“As the administration continues to work on implementing the law, it must continue to keep patients out of the middle of billing disputes and raise awareness about the law among both patients and providers,” said a spokesperson for Sen. Maggie Hassan (D-N.H), a cosponsor of the No Surprises Act (NSA), in the Morning Consult news release.
Only 16% of adults surveyed said they were aware of the No Surprises Act, down from 19% at the law’s launch in January, the study found.
Another Study Finds NSA Making Progress
America’s Health Insurance Plans (AHIP) and the Blue Cross and Blue Shield Association (BCBS) conducted a survey of commercial health plans. According to their findings, in its first two months, the No Surprises Act may have prevented two million surprise bills from reaching commercially insured patients, and it is possible 12 million surprise bills may be averted in 2022.
Though a much smaller survey, the 31 respondents to the AHIP-BCBS study represented 115 million commercial enrollees or 54% of the total commercial insurance market. The data they shared included:
Number of commercial claims incurred and paid during January and February.
Number of those claims that were No Surprises Act-eligible.
From those data, the study found 600,000 No Surprises Act-eligible claims in the market in January and February. Following calculations using 2020 Census data of commercial enrollees (213 million), the study authors estimated the No Surprises Act may stop 12 million unexpected healthcare bills in 2022.
Clinical laboratory tests will likely be a focal point in more studies about the No Surprises Act’s effectiveness. Medical lab and anatomic pathology group leaders may want to check-in with reference laboratory and billing company partners to ensure compliance with the most recent federal laws concerning balance billing.
Answers and effective solutions to the lab profession’s most urgent challenges will be front and center at the innovative ‘Lab Management Essentials Workshop’
Three powerful forces are slamming clinical laboratories today. One is the urgent need to cut costs. Second is the struggle to achieve and maintain full lab staffing. Third is the pressure to increase revenue and expand market share.
All of this is happening even as hospitals and health systems must deal with almost identical issues. Cost-cutting, recruiting more staff, and finding ways to increase revenue dominate the thoughts and actions of senior health administrators.
Most Hospitals and Health Systems Report Substantial Financial Losses
News reports about the financial losses at hospitals and health systems tell the story. For example, one report in Becker’s Healthcare described the financial damage at three major, multi-state health systems:
AdventHealth, a 48-hospital health system, reported a $417.7 million net loss in the first quarter of 2022. It reported that, because of inflation, costs had increased by 15% over prior year.
Kaiser Permanente, with 12.6 million members in seven regions of the United States, reported a net loss of $961 million in the first quarter of 2022. One major factor in these losses was the increase in expenses, which was 9.5%. For second quarter 2022, Kaiser Permanente showed a loss of $1.3 billion, most of that from a decline in the value of its investment portfolio.
Ascension Health, with 143 hospitals in 19 states, reported a net loss of $884.7 million in first quarter of 2022. It said its costs increased by 10.6% over the same period last year.
Most hospital-based clinical laboratory managers and pathologist are aware of these staggering financial losses. They also are watching how the shortage of nurses and other skilled personnel has hospitals scrambling to close that gap by paying more overtime, using temporary nurses who are paid at much higher rates, and increasing nurse salaries to prevent existing staff nurses from taking more lucrative offers from other hospitals in the community.
Clinical Laboratories Under Pressure to Cut Costs and Maintain Adequate Staff Levels
Hospital-based laboratories are on the frontline of these hurricane forces. Facing operating losses, hospitals ask their laboratories and other clinical service lines to cut costs below authorized budgets. Meanwhile, the labs themselves must deal with their own shortage of medical technologists (MTs) and clinical laboratory scientists (CLSs)—along with other skilled positions—that are required to provide the full menu of lab testing services.
This “perfect storm” of pressures to cut costs, keep staffing at authorized levels, and generate more revenue (that can offset rising costs of lab supplies and the higher salaries being paid to MTs and CLSs) is without precedent in the past four decades. To provide lab managers with the knowledge to resolve these challenges swiftly and confidently in their own laboratories, the team behind the Executive War College assembled experts to conduct a one-and-a-half-day interactive workshop.
Using Lab Case Studies to Teach Proven Solutions for Reducing Expenses
Each of the three important topics will be addressed in half-day learning modules. Following case study presentations on best practices, attendees at Lab Management Essentials will break out into smaller roundtable groups facilitated by lab industry experts. The groups will brainstorm how to apply these proven methods to cut costs, retain employees, and create revenue. They will then describe their findings to all participants.
Lab Management Essentials Workshop facilitators (clockwise from top left): Tafney Gunderson, Carlton Burgess, Dorothy Martin, Rick VanNess, Jane Hermansen, and Kim Zunker.
On the morning of day one, leaders of the lab cost-cutting module will be:
Carlton Burgess, Vice President of Laboratory Services at Prime Healthcare in Ontario, Calif.
Tafney Gunderson, Quality Systems Supervisor at Avera McKennan Laboratory in Sioux Falls, S.D.
On the afternoon of day one, leaders of the lab staff recruiting, hiring, and retention module will be:
Dorothy Martin, Regional Laboratory Manager at Dartmouth-Hitchcock Health in Lebanon, N.H.
Kim Zunker, MBA, MLS(ASCP), CAPM, Consulting Manager at Accumen in Scottsdale, Ariz.
On the morning of day two, leaders of the lab staff recruiting, hiring, and retention module will be:
Jane Hermansen, MBA, MT(ASCP), Manager of Outreach and Network Development at Mayo Clinic in Rochester, Minn.
Rick VanNess, Director of Product Management at Rhodes Group and TriCore Reference Laboratories in Albuquerque, N.M.
Delivering Essential Knowledge to Up-and-Coming Laboratory Managers
This Lab Management Essentials workshop is a first for the clinical laboratory profession. It brings together experienced, effective lab leaders to teach, guide, and coach your lab’s smartest up-and-coming lab managers. It accomplishes this in just one-and-a-half days, to minimize the time they are away from your lab.
To gain maximum benefits from this well-designed program, it is recommended that you send three or four of your front-line lab managers. Together, they will hear and learn at the same time, while working during the intimate sessions to identify the techniques and methods that will work best for your lab. This is important because, upon their return, they will have both enthusiasm and the knowledge to light the right fires under your lab staff and energize them into quickly deploying ways to slash expenses, attract top candidates to fill open positions, and even to tap new sources of revenue—all of which they learned during Lab Management Essentials.
Because the number of attendees to each workshop is limited, you are encouraged to click here to register yourself and your designated lab managers today.
Federal judge must rule on her bid for a new trial, after former Theranos lab director Adam Rosendorff’s statement that he regrets his testimony during her criminal fraud trial
It is a rare event for a board-certified clinical pathologist to be named in national news headlines, but that is what is happening now to Adam Rosendorff, MD, who served as the CLIA laboratory director at Theranos for several years.
Rosendorff is once more the subject of news headlines because of his recent statements expressing “regret” about his testimony for the prosecution during the trial of Elizabeth Holmes, founder and ex-CEO of now defunct Theranos. This development caused attorneys for Holmes to file a motion for a new trial.
In August, Rosendorff showed up at the residence of Elizabeth Holmes and made statements to her attorneys that are the basis for the motion to conduct a new trial.
In a recent court filing requesting the new trial, Holmes’ attorneys described Rosendorff as a “star witness” for the prosecution and pointed out, “The government mentioned him more than any other government witness in both opening and closing statements, and Dr. Rosendorff testified longer than any other government witness.”
During four days of testimony last October, Rosendorff emerged as a central prosecution witness. On the stand, he supported prosecutors’ contention that Holmes knew about the accuracy issues with Theranos’ Edison blood-testing device and intentionally mislead investors and patients.
In court testimony, Adam Rosendorff, MD (above) said, “I had frequent conversations with Elizabeth about concerns that I had in the laboratory,” and [that] she was often copied on emails discussing issues, the Wall Street Journal reported at the time. As clinical laboratory leaders who closely followed his testimony know, Rosendorff was Theranos’ laboratory director from April 2013 to November 2014. (Photo copyright: LinkedIn.)
Rosendorff Attempts to Meet with Holmes
The “Dr. Rosendorff’s Encounter at Ms. Holmes’ Home” section of the 17-page filing states Rosendorff appeared at the home of Holmes and her partner William Evans on August 8 after leaving a voicemail earlier in the evening asking for a meeting with Holmes. Rosendorff allegedly had two short conversations with Evans, who told him Holmes could not speak to anyone and asked Rosendorff to leave. Rosendorff was described by Evans as speaking in a “trembling” voice and appearing to be “in distress.”
The filing goes on to state Rosendorff told Evans “that he wanted to speak to Ms. Holmes because it would be ‘healing for both himself and Elizabeth to talk.’ He stated that ‘when he was called as a witness, he tried to answer the questions honestly but that the prosecutors tried to make everyone look bad’ and that ‘the government made things sound worse than they were when he was up on the stand during his testimony.’”
The filing continues: “Dr. Rosendorff stated that ‘Theranos was early in his and [Ms. Holmes’] career,’ that ‘everyone was just doing the best they could,’ and ‘everyone was working so hard to do something good and meaningful.’”
The section concludes, “He stated that ‘he fe[lt] guilty’ and that he ‘felt like he had done something wrong,’ apparently in connection with his testimony in Ms. Holmes’ case. He stated that these issues were ‘weighing on him’ and that “he was having trouble sleeping.’”
Rosendorff’s Regrets Unlikely to Trigger New Trial
In the filing, Holmes’ attorneys wrote, “under any interpretation of his statements, the statements warrant a new trial under Rule 33. But, at a minimum … the Court should order an evidentiary hearing and permit Ms. Holmes to subpoena Dr. Rosendorff to testify about his concerns.”
Bloomberg, however, quoted criminal defense attorney Michael Weinstein, JD, Chair of Cole Schotz P.C.’s White-Collar Litigations and Government Investigations Practice, as saying Rosendorff’s misgivings about his testimony are unlikely to warrant a new trial.
“A witness having second thoughts and how they were generally perceived is not new in criminal trials but often don’t lead to new trials or much of anything,” Weinstein told Bloomberg. “The burden for that is simply too high.” Weinstein was not involved in the Holmes case.
CBS News reached out to Rosendorff via LinkedIn, who responded he had no comment, adding, “Do not contact me.”
Nevertheless, Holmes’ lawyers have proposed an October 3 hearing to discuss why they believe a new trial is merited. Their request for a new trial came less than a week after U.S. District Judge Edward Davila rejected the defense team’s bid to have Holmes’ January convictions thrown out, the Mercury News reported.
“The evidence does support the jury’s findings,” Davila said at a September 1 hearing in San Jose, California, in which he issued a preliminary ruling denying her bid to have the verdict thrown out.
Theranos Saga Continues
At the hearing, Holmes’ lawyer Amy Mason Saharia, JD, told Davila the defense team would make another attempt to overturn the jury’s findings based on “new evidence,” the Mercury News stated. That new evidence appears to be Rosendorff’s admission that he has regrets about his testimony in the case.
Holmes, 38, is currently free on bail, but faces up to 20 years in prison and a fine of $250,000, plus restitution on each of four counts. She will be sentenced on October 17. The court originally set her sentencing date for September 26, but agreed to delay her sentencing without giving a reason for the delay, CBS News reported.
Will former Theranos laboratory director Adam Rosendorff, MD’s, regrets alter the court’s previous decisions? Who knows? Many clinical laboratory directors and medical laboratory scientists followed Elizabeth Holmes’ nearly four-month long fraud trial with rapt interest. They will now have to wait a few more weeks to find out if the disgraced Theranos executive will get a new trial or a prison sentence.
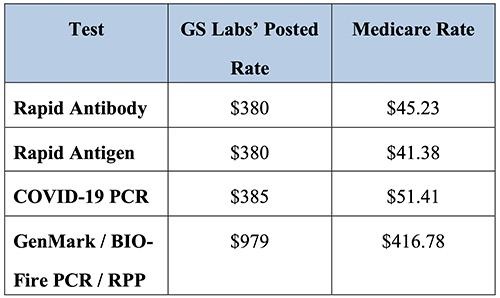
Insurers from three states claim pandemic start-up medical lab company charged as much as $979 for SARS-CoV-2 PCR test
In an unprecedented move, Blue Cross insurers in three states are suing a clinical laboratory company in Nebraska for test price gouging during the COVID-19 pandemic. The lawsuit claims that the lab company charged as much as 10 times more than other labs for similar tests.
The interesting twist to the pricing aspect of this story is that the Coronavirus Aid, Relief, and Economic Security Act (CARES Act) requires insurers to pay the full publicly-posted cost of COVID-19 testing. This means that, in many cases, the insurers may have no choice but to pay.
Is GS Labs, which was formed by an investment firm in the early months of the COVID-19 pandemic, yet another example of unscrupulous clinical laboratory operators taking advantage of the demand for COVID-19 testing during the early years of the coronavirus pandemic? GS Labs says no. The courts will decide.
Taken from the Premera Blue Cross court documents, the chart above shows GS Labs’ test prices compared with Medicare reimbursement rates. “As demonstrated by the following chart, the prices GS Labs charges insurers for COVID-19 testing well exceed the reimbursement rates set by Medicare Administrative Contractors, and in some cases are nearly ten times Medicare rates,” Premera states in the documents. Nevertheless, the federal CARES Act requires insurers to pay any COVID-19 test price a clinical laboratory posts publicly on its website. (Graphic copyright: Premera Blue Cross.)
Responding to Nationwide Demand for COVID-19 Testing
In October 2020, GS Labs began offering COVID-19 tests to provide Omaha residents with “convenient and quick testing options with same-day appointments and same-day results,” according to the company’s website. In response to nationwide demand, GS Labs quickly opened more than 20 testing COVID-19 testing sites across multiple states in its first three months of operations.
Today, GS Labs operates 14 rapid COVID testing locations in Iowa (1), Minnesota (6), Nebraska (1), Oregon (1) and Washington (5), but is under fire in several states for alleged price gouging.
Blue Cross Blue Shield of Kansas City was the first insurer to file suit in July 2021, alleging unreasonable reimbursement rates. The Kansas City Business Journal reported that GS Labs responded with a counter suit a month later accusing Blue KC of a “reckless disregard for the law” and attempting to bully its way out of paying for $9.7 million in COVID-19 testing fees.
The CARES Act states that, in the absence of a contractual payment agreement, insurers are required to pay the “cash prices” testing providers post on their public websites.
Christopher Erickson, a GS Labs Partner, told The New York Times (NYT), the law is on GS Labs’ side. “Insurers are obligated to pay cash price, unless we come to a negotiated rate,” he said.
In the fall of 2021, Premera Blue Cross also filed suit in Washington state alleging the lab routinely uses deceptive practices to run multiple unnecessary COVID tests on patients at an inflated cost. “In the words of one former employee, it ‘manipulates people into thinking they need all three COVID [sic] test’ that GS Labs offers, such that ‘[p]atients are being lied to just so th[e] company can make a profit,’” court documents state.
Premera also alleges in its lawsuit that GS Labs failed to report test results in a timely manner and returned hundreds of tests that were “by its own admission, tainted by “deviat[ions] from applicable laboratory standards for testing facilities.”
“This is fraud, and it’s fraud against Premera, it’s fraud against the industry, and more importantly, it’s fraud against the customers,” Courtney Wallace, DNP, Premera’s Director of Strategic Communications, told Washington State Wire.
And earlier this year, Blue Cross Blue Shield of Minnesota sued GS Labs to recover more than $10 million in over payments made since the start of the pandemic. A BCBS of Minnesota new release states that GS Labs “consistently charged more than five times the median market rate for its most commonly administered COVID-19 diagnostic test.”
CMS Inspection Finds GS Labs Site Posed “Immediate Jeopardy”
APM Reports spent nearly a year investigating the startup lab. Its team of journalists interviewed more than 65 GS Labs customers, former employees, and public health professionals, and reviewed thousands of pages of public documents. It concluded the lab “at times delivered inaccurate results, faced backlogs, charged high prices, and pushed customers into unnecessary tests.”
The APM Reports investigators found:
The company was slow to inform public health officials in several states about positive cases and in a few instances reported negative results to patients who had COVID-19. Other patients never received test results or received someone else’s results.
Overwhelmed by the number of tests it was processing, GS Labs at one point had a month-long backlog of untested samples.
Health officials in three states found GS Labs’ work was slower and less reliable than other labs.
According to APM Reports, in an email to colleagues about flaws in GS Labs’ operation in Washington state, Melissa Pond, [then] Program Manager for Clark County Washington’s COVID-19 Response Team, wrote, “[It] makes me so angry that they brought their greed to our community. They just popped up to make money knowing they would fly under the radar as long as possible and close their doors when someone caught them!”
Providing COVID-19 Testing During a Time of Need
APM Reports noted GS Labs’ founders formed the company in the early days of the pandemic after their friends and family could not find tests following a COVID exposure.
GS Labs is a subsidiary of City+Ventures, an Omaha investment and development company. Its portfolio includes an aviation investment company, car wash chain, car dealerships, restaurants, and other businesses.
City+Ventures’ co-founders, Erickson and Danny White had no healthcare investments prior to 2020, APM Reports noted. But early that year, the two men had joined with Gabe Sullivan and Darin Jackson, MD, who currently owns Prestige Medical Laser Solutions in Omaha, to create a men’s health and anti-aging company called 88MED. During the pandemic, that company transitioned to COVID-19 testing and was renamed GS Labs.
It is worth noting that GS Labs responded at length and in detail to the questions raised by the APM Reports investigation. It is useful reading for clinical laboratory leaders who wish to be fully informed on both sides of the controversy.
In its rebuttal, the company pointed out it had processed more than 2.1 million tests nationwide with less than 1.5% of its results being called into question. It maintained “GS Labs’ policy has never been to ‘push’ tests on anyone” and stated its cash prices “were higher than some testing providers,” but “lower than others” and reflected the company’s significant start-up costs.
GS Labs wrote, “At a time when our communities desperately needed increased COVID testing capacity, GS Labs took action to deliver that testing, investing more than $150 million in a business whose prospective success and lifespan were extremely uncertain. By filling a critical gap in COVID testing, GS Labs literally saved lives, and we are extremely proud of the service that we have provided to the communities we serve.”
GS Labs also has countersued BCBS of Minnesota, denying all prior allegations made by the insurer and alleging 21 counter claims.
Sabrina Corlette, JD, Research Professor and Project Director at Georgetown University Center on Health Insurance Reforms, has studied coronavirus testing prices. She told the NYT, “This is not like neurosurgery where you might want to pay a premium for someone to have years of experience.” She pointed out the CARES Act may provide GS Labs with the legal grounds to charge above market prices.
“Whatever price the lab puts on their public-facing website, that is what has to be paid,” she said.
GS Labs may have found a legal loophole to justify its sky-high COVID-19 testing prices, but consumers may view this behavior by a clinical laboratory company as unethical and yet another reason to be disillusioned with America’s healthcare system.
There are reports of phlebotomists refusing to draw monkeypox blood samples and social stigma surrounding the disease can affect who gets a medical laboratory test
Cases of monkeypox are increasing in the US—14,115 as of Aug. 19, up 1,400 from the prior week—and clinical laboratories around the country are bracing for a potential increase in monkeypox testing orders.
Several factors, however, are affecting the testing. Chief among them:
Lab workers refusing to take blood draws from potential monkeypox patients, and
Community clinics in some cities having to delay other care to deal with an onslaught of monkeypox test orders.
Here are five trends clinical laboratory leaders should be aware of that are influencing the state of monkeypox testing in the country.
Trend 1: Some Phlebotomists Refuse to Draw Possible Monkeypox Specimens
CNN reported that phlebotomists at two of the largest commercial laboratories—Labcorp and Quest Diagnostics—were either refusing or being told not to draw blood samples from suspected monkeypox patients.
“Labcorp and Quest don’t dispute that, in many cases, their phlebotomists are not taking blood from possible monkeypox patients,” according to CNN. “What remains unclear, after company statements and follow-ups from CNN, is whether the phlebotomists are refusing on their own to take blood or if it is the company policy that prevents them. The two testing giants say they’re reviewing their safety policies and procedures for their employees.”
In “Medical Laboratories Respond to Monkeypox Outbreak Using CDC-Developed Diagnostic Test,” Dark Daily noted that skin lesion swabbing, such as that necessary to perform the OrthopoxvirusPCR test, is the preferred method to check for monkeypox because of higher viral counts in the lesions. However, physicians may order follow-up blood tests for confirmed monkeypox patients, and suspected patients may need bloodwork as part of other routine care.
In an update posted on its website, Quest noted it has been testing swab specimens of skin lesions for monkeypox, but those swabs are performed by providers and not Quest. However, the company was also preparing to take blood draws of possible monkeypox patients in its patient service centers.
“Given that monkeypox has been declared a national public health emergency and the most recent CDC guidance, we are now implementing procedures to safely enable patients with suspected or confirmed monkeypox infection into our patient service sites for phlebotomy blood draws and other non-swab specimen collections,” Quest stated. “This approach will enable patients with suspected or confirmed monkeypox infections to receive additional testing they may need.”
Trend 2: Guidance Is Available to Help Lab Workers Avoid Monkeypox Infection
The CDC has posted guidance to maintain infection control around suspected monkeypox specimens. Among the steps noted by the agency:
Lesion specimens from patients suspected of having monkeypox will carry the highest quantity of the virus. When possible, lab workers that have a smallpox vaccination from within the last three years should handle these specimens. Smallpox vaccination also protects from monkeypox in many cases. Unvaccinated workers who test suspected monkeypox specimens need to take extra precautions, such as wearing a buttoned lab coat, gloves, and face protection, and avoiding splashes, the CDC stated.
Blood specimens draw from suspected monkeypox patients will have a low quantity of the virus. Lab workers testing these specimens do not need to be vaccinated for monkeypox, but standard precautions should be followed.
Before using automated testing platforms with suspected monkeypox specimens, labs should conduct a risk assessment to identify potential hazards.
Trend 3: Monkeypox Testing Gains an Early Social Stigma
Some people who need to be tested for monkeypox may be hesitant to seek out a medical laboratory or patient service center because of a stigma being attached to the disease.
Although it does not match the early hysteria associated with HIV infections in the 1980s—in a 1987 poll, 60% of respondents said AIDS patients should carry a card identifying them as such, Gallup noted—there have been clear instances where people and agencies have associated monkeypox infection with men having sex with other men.
“The focus for all countries must be engaging and empowering communities of men who have sex with men to reduce the risk of infection and onward transmission, to provide care for those infected, and to safeguard human rights and dignity,” Tedros Adhanom Ghebreyesus, PhD, the Director-General at the World Health Organization, said in a July 27 media briefing.
Ghebreyesus added that while 98% of monkeypox infections have been among men who have sex with men, anyone can get the disease, including children.
“Stigma and discrimination can be as dangerous as any virus, and can fuel the outbreak,” said Tedros Adhanom Ghebreyesus, PhD (above), Director-General at the World Health Organization (WHO), in a media briefing. Clinical laboratories would be wise to prepare for a marked increase in demand for monkeypox testing. (Photo Copyright: WHO/Christopher Black.)
“Men who have sex with men have been hit the hardest by monkeypox to date, but LGBTQ+ health advocates say improper messaging risks branding monkeypox as a ‘gay disease,’ eroding effective preventive measures and allowing the virus to spread,” Bloomberg Law reported.
For example, 66% of respondents either were not sure or did not believe there is a vaccine for monkeypox.
Trend 4: Workers Who Refuse to Test Patients for Monkeypox Face Possible Backlash
Some medical professionals have raised concerns about healthcare workers being unwilling to test monkeypox patients.
“This is absolutely inexcusable. It’s a grave dereliction of duty,” David Harvey, Executive Director of the National Coalition of STD Directors, told CNN. The group represents sexually transmitted disease (STD) directors at public health departments in the US.
“For every single patient that walks [through] your door, you use universal precautions because every disease doesn’t have a phenotype or outward appearance, so you have to treat everyone exactly the same,” Garfield Clunie, MD, president of the National Medical Association and Assistant Professor of Obstetrics, Gynecology, and Reproductive Science at the Icahn School of Medicine at Mount Sinai, told Bloomberg Law. “You can’t treat someone differently because of their sexual orientation, or race, or gender, or for any other reason.”
Trend 5: Public Clinics Show Early Signs of Monkeypox Testing Pressure
A survey of 80 public health departments conducted by the National Coalition of STD Directors indicated that some sites may already be getting overwhelmed by demand for monkeypox testing.
According to the survey results, 79% of public health clinics saw an increased demand for monkeypox testing over the past four weeks. In a troubling aspect, 28% of clinics said they could not meet testing demand if it increases.
Further, 22% of clinics have reduced screenings for other STDs to prioritize monkeypox testing. Such moves likely delay patients from receiving other care they need.
Clinical laboratories may want to take note of the survey findings. The pressure public health clinics currently face could be a precursor to similar problems at labs if demand for monkeypox testing grows.
By partnering with drug manufacturers to connect customers with clinical trials, the retail pharmacy chain believes this new venture will be the company’s “next growth engine.”
Walgreens is launching a business to connect customers with clinical drug trials, a venture that adds another offering to the retail pharmacy giants’ growing menu of healthcare services. This new venture might also mean additional test orders for clinical laboratories and pathology groups in areas that serve Walgreens customers.
Now, Walgreens is attempting to further redefine the patient experience by partnering with pharmaceutical companies to find participants for clinical trials, a business that could result in more Americans from underrepresented racial and ethnic populations enrolling in drug-development trials. With 9,021 retail pharmacies in all 50 states, it is well-positioned to know which of its customers would be candidates for different clinical trials.
“Walgreens’ trusted community presence across the nation, combined with our enterprise-wide data and health capabilities, enables us to pioneer a comprehensive solution that makes health options, including clinical trials, more accessible, convenient and equitable,” said Ramita Tandon, Walgreens’ Chief Clinical Trials Officer, in a press release.
Ramita Tandon, Walgreens’ Chief Clinical Trials Officer, believes Walgreens can play a role in solving the issues of diversity and declining enrollment in clinical trials. “Through the launch of our clinical trials services, we can provide another offering for patients with complex or chronic conditions in their care journey, while helping sponsors advance treatment options for the diverse communities we serve,” she said in a press release. (Photo copyright: Walgreens.)
Serving the Socially Vulnerable
In an interview with Fierce Healthcare, Tandon described the clinical trials business as Walgreens’ “next growth engine” of consumer-centric healthcare solutions.
According to the company press release, “Walgreens is addressing access barriers through a compliant, validated and secure decentralized clinical trial platform built on a rigorous compliance and regulatory framework to ensure patient privacy and security. This approach leverages owned and partner digital and physical assets, including select Health Corner and Village Medical at Walgreens locations, to directly engage patients at home, virtually or in-person.”
Walgreens notes that more than half of its roughly 9,000 U.S.-based stores are in “socially vulnerable areas.”
According to the Washington Examiner, a US Food and Drug Administration (FDA) study revealed that 75% of patients who participate in clinical trials are white, while just 11% are Hispanic and fewer than 10% are Asian or black. In addition, participation in clinical trials has been declining, with 80% of trials failing to attract enough participants on time.
Tandon maintains that making the process of participating in clinical trials easier is another key to increasing diversity and participation in clinical trials.
“During the clinical trial journey, we know it’s a burden for patients to visit sites. We also know that 78% of patient-consumers in the US live within five miles of a Walgreens,” she told PharmaVoice. “If a patient can complete much of the up-front clinical trial requirements at a local Walgreens, or conduct some of the visits digitally, it would make the whole clinical trial experience that much more positive and, maybe, encourage the patient to participate in new clinical trials going forward.”
Walgreens also plans to use its treasure-trove of customer data to find potential patients for its trials business.
“Understanding this detail of customer preference and segmentation can be quite useful particularly in clinical trials, for example, to create better protocols,” Tandon told PharmaVoice. “We are sitting on so much information, but we can, and need to, do a better job of using these insights in a real-world setting, which can be translated to pharma R/D or brand management organizations. We’re all about patient-centric drug development.”
FDA Seeks Diversity in Clinical Trails
Walgreens is in discussions with several drug manufacturers as it looks to launch this new venture.
“We are working very closely with them to understand their business needs and create the solution that’s going to be sort of bespoke to their specific trial needs,” Tandon told Fierce Healthcare. “Our goal is to move that needle and start to see a larger number of US patients participating and highly diverse participants that are coming into clinical trials.”
In April, an FDA press release announced new draft guidance aimed at “developing plans to enroll more participants from underrepresented racial and ethnic populations in the US into clinical trials.”
“Despite having a disproportionate burden for certain diseases, racial and ethnic minorities are frequently underrepresented in biomedical research,” the FDA stated. “Clinical trials provide a crucial base of evidence for evaluating whether a medical product is safe and effective; therefore, enrollment in clinical trials should reflect the diversity of the population that is ultimately going to use the treatment.”
Disintermediation of Retail Pharmacies
“Walgreens has a significant opportunity to create an interconnected healthcare ecosystem where we can use the physical assets of Walgreens and connect with patients and consumers at a local level to better support healthcare and healthcare equality,” Tandon said in PharmaVoice.
This is the latest example of a billion-dollar retail pharmacy chain diversifying away from simply filling prescriptions. Two types of competitors are driving the disintermediation of retail pharmacies because they end up directing patients away from the pharmacy:
Amazon.com acquired PillPack and now sends, via mail, prescriptions to patients’ homes.
Pharmacy benefit management (PBM) companies with a business model that encourage patients to get 90 days of prescriptions at once, mailed to their home.
In both cases, retail pharmacies lose access to patients. This is what is motivating several national pharmacy chains to offer primary care within their retail pharmacies (where following an office visit with a general practitioner, the patient simply crosses the store to the pharmacy to fill his/her prescription), as well as the clinical trial matching business.
As retail pharmacy chains become an increasingly disruptive force in healthcare, clinical laboratory managers and pathologists should be preparing new strategies to meet the testing needs of a changing primary care delivery model, which likely will include lab testing being offered in nontraditional medical locations.