COVID lab testing company reportedly was paid up to $124 million for COVID-19 testing
What do an axe-throwing lounge, a donut shop, and a COVID-19 testing company have in common? All three were under the ownership of the same husband and wife. Apparently, though, COVID-19 medical laboratory testing was more lucrative. It’s been reported this married couple’s testing company received as much as $124 million just from federal health programs.
The co-owners are now being sued by multiple state’s attorney generals for allegedly failing to deliver SARS-CoV-2 test results and/or for delivering COVID-19 test results that “were falsified or inaccurate,” according to NBC News.
Chicago-based Center for COVID Control (CCC)—an operator of 300 pop-up COVID testing sites nationwide—faces investigations from state and federal authorities amid allegations of improper procedures and business practices. The company voluntarily suspended operations in January, when the allegations first surfaced, according to a company press release.
The founders, who had no prior clinical laboratory experience, now say they have turned their attention from running the sites to handling the investigations, USA Today reported. The newspaper was the first to publicly report problems with the company and its associated lab, Doctors Clinical Laboratory (DCL), both of which have the same address in suburban Chicago.
According to USA Today, “The Center for COVID Control was incorporated in December 2020, according to Illinois state filings. The business, which describes itself as a ‘test collection marketing and management firm,’ worked closely with Doctors Clinical Lab. Regulators didn’t visit the lab for an on-site inspection until the end of September of the following year, according to the Centers for Medicare and Medicaid Services. Regulators found the lab was not reporting coronavirus test results to public health officials.”
Questionable Collection Procedures for COVID-19 Testing
An earlier USA Today story by reporter Grace Hauck described an outdoor COVID-19 collection site in Chicago run by a man operating from a small shack powered by a generator.
“As he opens the door, piles of plastic bags, apparently grouped by test type, can be seen in crates on the ground,” Hauck reported. “He encourages test-takers to scan a QR code with their phones, fill out an online form with identifying information, and write a digitally-generated string of numbers on a paper sheet inside the plastic test kit bag.”
Hauck’s story noted complaints from readers about shoddy specimen collection procedures, conflicting or errant clinical laboratory test results, and failure to receive COVID-19 results in a timely manner.
Block Club Chicago, a non-profit news site, reported on Jan. 13 that inspectors from the Centers for Medicare and Medicaid Services (CMS) had uncovered numerous instances of “non-compliance” and “deficiencies” at DCL.
CMS lab inspectors found that DCL “could not process or store PCR test samples appropriately—while it was being inundated with tests,” the news site reported. “Over an 11-day period in November, the lab received 84,436 PCR test samples; over that period, it processed and reported 43,240 test results, according to the [CMS] report.”
Specific problems included:
Inadequate staffing, training, and quality controls at the clinical laboratory.
A lack of freezers needed to store test samples.
Failure to maintain confidentiality of patient information.
Failure to label samples with identifying information.
Failure to log complaints from test recipients.
USA Today reported that the FBI executed a search warrant at the companies’ suburban Chicago offices on Jan. 22.
State Actions against Doctors Clinical Laboratory and CCC
In addition to the federal actions, state attorneys general in Minnesota and Washington State both filed lawsuits against Center for COVID Control (CCC) and Doctors Clinical Laboratory (DCL).
“When Minnesotans and people from around the country tested with these companies to keep themselves and their families safe, they trusted they would get correct [COVID-19 test] results on time,” said Minnesota Attorney General Keith Ellison in a statement announcing a lawsuit against the two companies. “I’m holding these companies accountable that sent back false or inaccurate [COVID-19 test] results, when they sent them back at all, for deceiving Minnesotans and undermining the public’s trust in testing.” (Photo copyright: Office of Minnesota Attorney General.)
Washington Attorney General Bob Ferguson filed suit in King County Superior Court on Jan. 31. “Center for COVID Control contributed to the spread of COVID-19 when it provided false negative results,” he stated in a news release. “These sham testing centers threatened the health and safety of our communities.”
On Feb. 17, Ferguson announced that the court had granted a preliminary injunction that prohibited CCC from providing testing services in the state.
NBC News reported that authorities in other states have also taken actions against the company. Oregon and Illinois launched civil investigations, while “Massachusetts and Rhode Island have issued cease and desist letters to the company, and local regulators in Washington and California shut down several of its sites for operating without a license,” the newspaper reported.
Big Money in COVID-19 Testing
USA Today reported that CCC was launched in December 2020 by Akbar Syed, 35, and Aleya Siyaj, 29, a married couple. Siyaj is listed as being CEO of CCC since June 2021, according to her LinkedIn profile.
“Doctors Clinical Lab is registered under another person’s name in state records, but federal documents and multiple former employees and business partners claimed Siyaj and Syed run the lab and Center for COVID Control,” Block Club Chicago reported.
USA Today reported that DCL received more than $124 million in federal reimbursement for COVID-19 clinical laboratory testing and treatment. The paper also described a lavish lifestyle for Syed and Siyaj, including recent purchases of a $1.36 million mansion and multiple luxury cars. Asked on social media site TikTok about the source of his wealth, Syed stated, “COVID money,” according to USA Today.
Siyaj and Syed have denied wrongdoing, stating that they are now focused on “responding and cooperating with legal probes, and to clearing our good names,” according to a statement provided to USA Today.
Regulatory Loopholes
One question about CCC and DCL is how they were able to escape regulatory scrutiny. “Some experts said unscrupulous lab operators can take advantage of a regulatory opening that allows labs to register, test, and bill before inspectors finish a CLIA certificate survey,” USA Today reported. “In other cases, investors might purchase or establish management agreements with labs and begin testing before inspectors get in to verify the lab’s reliability.”
Pathologists and clinical laboratory managers will want to continue to watch the news, as other examples of fraud and incompetence by new companies that rushed into the COVID-19 lab testing marketplace are uncovered and investigated by both state and federal regulators.
Further, some of these companies may have generated more than $1 billion in payments from public and private sources after launching testing operations in the months after the arrival of the pandemic.
Medical laboratories and anatomic pathologists may need to squeeze into narrow networks to be paid under value-based schemes, especially where Medicare Advantage is concerned
Pathologists have likely heard the arguments in favor of value-based payment versus fee-for-service (FFS) reimbursement models: FFS encourages providers to order medically unnecessary procedures and lab tests. FFS removes incentives for providers to order patient services more carefully. Fraudsters can generate huge volumes of FFS claims that take payers months/years to recognize and stop.
Studies that favor value-based payment schemes support these claims. But do hospitals and other healthcare providers also accept them? And how is value-based reimbursement really doing?
To find out, Chicago-based thought leadership and advisory company 4Sight Health culled data from various organizations’ reports that suggest value-based reimbursement shows signs of growth as well as signs of stagnation.
Value-Based Payment Has Its Ups and Downs
Healthcare journalist David Burda is News Editor and Columnist at 4Sight Health. In his article, “Is Value-Based Reimbursement Mostly Dead or Slightly Alive?” Burda commented on data from various industry reports that indicated value-based reimbursement shows “signs of life.” For example:
More doctors are accepting pay-for-performance payments: 44.5% in 2020, up from 42.3% in 2018, according to an American Medical Association (AMA) biennial report on physician participation in value-based reimbursement, titled, “Policy Research Perspectives: Payment and Delivery in 2020.”
On the other hand, Burda reported that value-based reimbursement also has these declining indicators:
39.3% of provider payments “flowed” through FFS plans in 2020 with no link to cost or quality. This was unchanged since 2019. (HCPLAN report)
19.8% of FFS payments to providers in 2020 were linked to cost or quality, down from 22.5% in 2019. (HCPLAN report)
88% of doctors reported accepting FFS payments in 2019, an increase from 87% in 2018. (AMA report)
Does Today’s Healthcare Industry Support Value-based Care?
A survey of 680 physicians conducted by the Deloitte Center for Health Solutions suggests the answer could be “not yet.” In “Equipping Physicians for Value-Based Care,” Deloitte reported:
“Physician compensation continues to emphasize volume more than value.
“Availability and use of data-driven tools to support physicians in practicing value-based care continue to lag.
“Existing care models do not support value-based care.”
Deloitte analysts wrote, “Physicians increasingly recognize their role in improving the affordability of care. We repeated a question we asked six years ago and saw a large increase in the proportion of physicians who say they have a prominent role in limiting the use of unnecessary treatments and tests: 76% in 2020 vs. 57% in 2014.
“Physicians also recognize that today’s care models are not geared toward value,” Deloitte continued. “They see many untapped opportunities for improving quality and efficiency. They estimate that even today, sizable portions of their work can be performed by nonphysicians (30%) in nontraditional settings (30%) and/or can be automated (18%), creating opportunities for multidisciplinary care teams and clinicians to work at the top of their license.”
Hospital CFOs Also See Opportunities for Value-based Care
This could be problematic for clinical laboratories, according to Robert Michel, Editor-in-Chief of Dark Daily and our sister publication The Dark Report. According to Guidehouse, “Nearly 60% of health systems plan to advance into risk-based Medicare Advantage models in 2022.”
Medicare Advantage (MA) enrollments have escalated over 10 years: 26.4 million people of the 62.7 million eligible for Medicare chose MA in 2021, noted a Kaiser Family Foundation brief that also noted MA enrollment in 2021 was up by 2.4 million beneficiaries or 10% over 2020.
The graph above is taken from the Kaiser Family Foundation report, “Medicare Advantage in 2021: Enrollment Update and Key Trends.” According to the KFF, “In 2021, more than four in 10 (42%) Medicare beneficiaries—26.4 million people out of 62.7 million Medicare beneficiaries overall—are enrolled in Medicare Advantage plans; this share has steadily increased over time since the early 2000s.” Since MA employs narrow networks for its healthcare providers, it’s likely this trend will continue to affect clinical laboratories that may find it difficult to access these providers. (Graphic copyright: Kaiser Family Foundation.)
“The shift from Medicare Part B—where any lab can bill Medicare on behalf of patients for doctor visits and outpatient care, including lab tests—to Medicare Advantage is a serious financial threat for smaller and regional labs that do a lot of Medicare Part B testing. The Medicare Advantage plans often have networks that exclude all but a handful of clinical laboratories as contracted providers,” Michel cautioned. “Moving into the future, it’s incumbent on regional and smaller clinical laboratories to develop value-added services that solve health plans’ pain points and encourage insurers to include local labs in their networks.”
Medical laboratories and anatomic pathology groups need to be aware of this trend. Michel says value-based care programs call on clinical laboratories to collaborate with healthcare partners toward goals of closing care gaps.
“Physicians and hospitals in a value-based environment need a different level of service and professional consultation from the lab and pathology group because they are being incented to detect disease earlier and be active in managing patients with chronic conditions to keep them healthy and out of the hospital,” he added.
Value-based reimbursement may eventually replace fee-for-service contracts. The change, however, is slow and clinical laboratories should monitor for opportunities and potential pitfalls the new payment arrangements might bring.
Labs need to rethink recruitment tactics to successfully hire younger workers
We’ve heard a lot anecdotally about the “Great Resignation”—a labor phenomenon rooted in the pandemic that has led to an abnormally large amount of workers, including lab professionals, quitting their jobs.
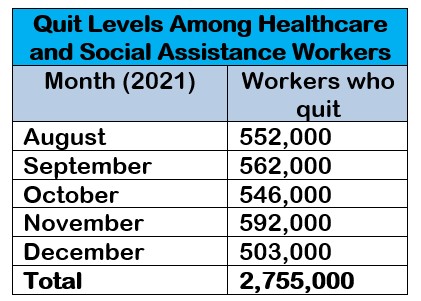
The trend has hit healthcare hard, as evidenced by the latest numbers from the U.S. Bureau of Labor Statistics. From August 2021 through December 2021, the healthcare and social assistance workforce saw nearly 2.8 million workers quit—an average of 551,000 people each of those months. By comparison, in December 2020, 419,000 healthcare workers left their jobs.
Nearly 2.8 million healthcare and social workers quit their jobs from August through December 2021. Source: Bureau of Labor Statistics.
Anxiety from the pandemic is likely a contributing factor to some job departures. However, in clinical labs, other causes also are behind the abundance of open positions, such as early retirements, graduating individuals experiencing more specialized training programs, and a shift in the way the current working generation views employment, said Tara Luellen, Vice President of Laboratory Director Services at consulting and recruiting firm Lighthouse Lab Services.
“The lab industry has been hurt at the greatest extreme from this Great Resignation just in terms of the dire need for lab roles and the small pool of correctly qualified individuals in many instances,” particularly with COVID-19 testing demand, she noted.
Specialized Laboratory Roles Cramp Further Development for New Hires
Luellen explained that the labor shortage problem is exacerbated because fewer new lab technologists and pathologists are entering the field at the same time that many lab professionals are quitting.
Additionally, younger workers that do go into the clinical lab and pathology industry tend to be trained in specialty areas more so now than the broader training programs of the past.
“We don’t have as many individuals who are more broadly trained; instead, they’re very specialized,” she added. “So, it takes them years working at labs that do a variety of things to gain real-life, hands-on experience with other kinds of testing than that included in their specialty program, in many cases.”
“We don’t have as many individuals who are more broadly trained,” said Tara Luelllen.
‘They Want to Experience a Community at Work’
For clinical labs and pathology groups looking to fill open roles, it may be time to take action beyond just beefing up salaries.
Instead, look at what motivates lab professionals to come to an organization, Luellen suggested. She’ll explore the topic of how to successfully recruit new clinical lab leaders in further detail at her session during the 2022 Executive War College on April 27-28 in New Orleans.
One piece of advice she offered is for lab recruiters to carefully articulate to job candidates how an open lab director position or similar role may contribute to either the local or medical community. It’s also important to explain what type of culture an organization offers new employees.
“What we’re seeing is a big shift in what people are looking for,” Luellen said. “The compensation still has to be there, but it’s also a whole community that these people are looking for.
“They’re looking for more than just a 9 to 5, punch the clock, and go home gig,” she continued. “They want the job to enrich their lives. They want to experience a community at work. It’s a different paradigm in how they look at what work means for them.”
Due to the national health system’s aggressive cost-cutting measures over the past 20 years, some regions of the island country now have only limited local medical laboratory services
It was in the early 2000s when different district health boards throughout New Zealand decided on a strategy of issuing sole source, multi-year medical laboratory testing contracts in their regions to cut lab test testing costs. Consequently, pathology laboratories that lost their bidding were forced to cease operations or merge with the winning bidders. At the time, New Zealand pathologists and laboratory scientists feared the government health system was undermining the financial stability of pathology laboratories and leaving portions of the country with limited testing capacity.
Now, arrival of the SARS-CoV-2 Omicron variant on the remote island nation may be creating a day of reckoning for that decision. In particular, “holiday hotspots” in New Zealand may be filling up with seasonal travelers at the exact moment a surge in COVID-19 testing is needed.
Holiday Destinations Lack Pathology Lab Capacity
Medical laboratory scientist Terry Taylor, president of the New Zealand Institute of Medical Laboratory Science (NZIMLS), fears some small-town tourist destinations do not have the local-based medical laboratory testing capacity to process a surge in PCR tests and will need to ship samples elsewhere, delaying the speed at which COVID-19 test results can be delivered in communities that attract thousands of vacationers during New Zealand’s summer from December to February.
“In these areas, those swabs that are taken will end up being sent to the mothership so to speak, so one of the larger laboratories that’s nearby those regions,” he told Checkpoint. “So, there will be delays when this starts to kick on.”
Taylor also pointed out that shifting lab work to larger medical centers creates capacity concerns within those facilities as well.
“I will reiterate, all of the big hospitals will obviously still be operating 24-hour services doing the acute work that’s coming through,” he said. “But be aware, we do everything. We don’t just do COVID testing, so sometimes things are just going to have to wait in those periods.”
“We’ve certainly got to get together now and come up with a plan that works so that we do not inundate our laboratories and therefore the other health services,” medical laboratory scientist Terry Taylor (above), president of the New Zealand Institute of Medical Laboratory Science, told Newshub. “It is really not an option to test everyone. We need to be looking at who we test, how we test and when we test,” he added. (Photo copyright: Newshub.)
In a statement to Checkpoint, the New Zealand Ministry of Health maintained COVID-19 testing remained a priority for the government over the Christmas and New Year period.
“The ministry works closely with DHBs (District Health Boards) and laboratories to manage demands for testing, and to reiterate the importance of processing and returning tests as quickly as possible,” the statement said. “It should be noted that samples of close contacts of cases and high-risk individual are prioritized by laboratories.”
Dark Daily Correctly Predicted Pathology Lab Losses
In 2009, Dark Daily reported on New Zealand’s use of contract bidding for pathology lab testing services in Wellington and Auckland in an effort to drive down costs. The winning labs agreed to roughly a 20% decrease in reimbursement rates.
At that time, Editor Robert L. Michel predicted the loss of established pathology providers and insufficient reimbursement rates could lead to scaled down testing menus, loss of skilled staff and a negative impact on patient care. He noted then, “New Zealand may become the first developed country in the world to learn what happens to the entire healthcare system when deep budget cuts finally leave medical laboratories with insufficient reimbursement.
“Such a situation,” Michel continued, “would likely mean that laboratory test providers in New Zealand would lack the funding and resources to offer physicians and patients a full menu of state-of-the-art diagnostics tests. It could also mean that medical laboratories would lack adequate resources and skilled staff to sustain the quality of test results at a world-class level of quality, accuracy, reliability, and reproducibility. In either case, the quality of patient care would be negatively affected.”
Fast forward to 2022, as the COVID-19 pandemic continues some New Zealand leaders fear the opening of Auckland’s border to summer travelers will lead to community spread of the coronavirus at a time when budget cuts have left these same regions with local pathology testing capacity that is insufficient to meet the needs of the surrounding community.
In fact, New Zealand’s first case of community exposure to the Omicron variant was reported in Auckland on December 29, 2021, a Ministry of Health news release noted.
“You’re going to see the virus seeded everywhere,” epidemiologist Michael Baker, Professor of Public Health, University of Otago in Dunedin, New Zealand, told The Guardian in mid-November.
Critical Supply Shortages as Pathology Testing ‘Crunch Point’ Reached
In the early months of the COVID-19 pandemic, New Zealand’s clinical laboratory system nearly reached a breaking point as a shortage of COVID-19 tests left the system teetering on the edge of collapse.
According to Joshua Freeman, MD, Clinical Director of Microbiology and Virology at the Canterbury DHB, the “crunch point” arrived around March 20, 2020, when New Zealanders were being urged to get tested so the country could determine if there was community transmission of the virus, online news site Stuff reported.
Meanwhile, testing supplies such as reagents, plastic tubes, and pipette tips were in short supply globally and 13 regional labs were yet to be set up across the country. Even once the new laboratories, district health board testing centers, and mobile clinics were up and running, procuring needed supplies remained challenging, according to COVID-19 testing data from the Ministry of Health.
America also Struggled with COVID-19 Supply Shortages
While New Zealand’s mostly publicly funded universal healthcare system has been stressed by the COVID-19 pandemic, America’s private system has not fared much better. In the early months of the pandemic, personal protective equipment, COVID-19 tests, and testing materials also were in short supply in this country.
CBS News reported that the US was continuing to struggle with limited supplies of COVID-19 rapid antigen tests and long turnaround times for clinical laboratory polymerase chain reaction (PCR) tests as families gathered for the recent holiday season.
Thus, clinical laboratory leaders and laboratory scientists in this country should watch with keen interest at how New Zealand’s pathology laboratories fare as the Omicron variant further challenges the country’s testing capacity.
By automating clinical chemistry and immunoassay testing, clinical laboratory leaders can improve throughput while reducing the stress on staff, laboratory expert says
The American Society for Clinical Pathology regularly conducts a vacancy survey of medical laboratories throughout the US. While the problem of lab department vacancy rates has been ongoing, the last survey reported showed increased rates for laboratory positions across all departments surveyed. Last year, burnout among healthcare workers reached a crisis level, reported Clinical Laboratory News.
As a result, staffing the clinical laboratory with qualified lab professionals resounds as a top concern—and at a time when expectations are perhaps the highest they have ever been for performance in healthcare operations, from general hospitals to the most complex integrated delivery networks.
Even in the midst of the clinical laboratory workforce shortage and chronic strain, laboratory leaders must still improve their labs’ processes and workflows; increase productivity; and expand routine and specialty testing to better serve patient populations.
Faced with unrelenting pressures to do more with less, lab directors are turning to automating certain departments of the laboratory as a way to:
Relieve the problems caused by an ongoing workforce shortage;
Improve workflows and processes through standardization;
Keep lab staff working on the most important tasks; and
Enhance the laboratory’s reach and grow the lab business in necessary ways.
How UMC Southern Nevada Prioritized STAT Runs, Consolidated Operations
One case in point highlights the University Medical Center (UMC) of Southern Nevada’s clinical laboratory. Located in Las Vegas, UMC is among the largest public hospitals in the United States. It is part of a recent master-planned Las Vegas Medical District (LVMD), and it is the only Level I trauma center in Nevada.
The laboratory needed to improve turnaround time and expand the test menu, among other goals, explained Scott Keigley, one of two General Laboratory Services Managers at UMC. While limited laboratory automation had already been applied broadly, the lab took its automation initiative one step further by connecting three high-volume automated clinical chemistry and immunoassay analyzers (CC/IA), an automated hematology line, and a coagulation analyzer.
The University Medical Center of Southern Nevada improved efficiency andstreamlined workflow by integrating a consolidated automated clinical chemistry and immunoassay analyzer (above) into the laboratory’s workflow. (Photo copyright: Siemens Healthineers)
An immediate benefit that UMC realized was consolidation of clinical lab operations. “Up until implementing our automated platform, we had a dedicated laboratory in our emergency room specifically to triage our emergency room tests,” Keigley explained. “You’re talking about not only a duplication of consumables, resources, and supplies, but also personnel.
“A big part of automating was showing our administration we were going to be able to eliminate that emergency room lab and still turn our results around as quickly and as efficiently without it,” Keigley added.
One of the ways that using an automated platform enabled consolidation of lab operations was by decreasing the turnaround times of STAT samples. “Our STAT turnaround times are way below many of the national thresholds or standards,” Keigley explained. “I’ll use troponin as an example. National threshold is 60 minutes from received to result, but we average about 30 minutes.
“Throughput definitely increased,” Keigley added, emphasizing that this increased throughput was actually accompanied by a reduced workload. “We’ve seen a reduction in the amount of hands-on time required to do the daily maintenance and quality controls. Once the daily maintenance and controls are completed, the chemistry department can usually be run by one person.”
Choosing a Consolidated Automated Chemistry and Immunoassay Platform
Described as flexible for adding components, modular, and scalable, a consolidated clinical chemistry and immunoassay analyzer (CC/IA) can run from 1 million to 3 million tests per year. Designed with innovative technological internal controls and sample handling—and other capabilities that include automated instrument calibration, maintenance, and quality control (QC) functions—the CC/IA platform also works as a standalone and is a first step toward implementing laboratory automation.
At UMC, multiple factors influenced the decision to add the platform, explained Keigley. “One reason was the increased productivity that it (the Atellica Solution) from Siemens Healthineers offers. This technology frees up our techs to do what we went to school to do. I can show anyone how to load samples on these analyzers in five minutes, but that’s not what it’s about.
“We were able to expand our test menu and our services. The platform allowed us to grow.” Keigley estimates that UMC’s test menu grew up to 20% after the change, both expanding the types of testing that could be offered and decreasing the number of send-outs. He estimates that the chemistry lab now processes about 2.6 million reportable results per year.
There were several (QC) features that Keigley believes UMC’s laboratory benefits from. The key QC features Keigley identified include onboard temperature-controlled storage, programmable run times, and barcode-labelled tube options from the control manufacturer that eliminate manual programming.
Operational Evaluation—Nexus Global Solutions, Inc. (Nexus), Plano, TX
While the primary driving factor in UMC’s decision to use the Atellica Solution platform was based on its individual laboratory’s needs, a recent study commissioned by Siemens Healthineers illustrated the benefits of this system.
An operational comparison report by Nexus found that there are multiple advantages associated with this integrated automation platform—as a standalone component—when compared to a similar offering.
Specifically, the Nexus report found:
Start-up and maintenance time was almost an hour and a half less;
Manual start-up time requirements were 28 minutes, compared to 46 minutes;
From 65% to 69% of samples had a faster turnaround time; and
A system footprint that used 20square feet less space and four fewer analyzers.
Clinical laboratory leaders can review the methodology and results of the Nexus Global report by clicking on this link: www.siemens-healthineers.com/operational.
This article was produced in partnership with Siemens Healthineers.
As a Theranos insider and whistleblower, Tyler Schultz was able to provide information about the ongoing failures in medical laboratory testing at the once-high-flying Theranos to regulators and at least one journalist
What’s it like to be a whistleblower in a high-profile clinical laboratory? Few clinical laboratory workers will ever know. But former Theranos employee Tyler Shultz does know, after helping to expose the Silicon Valley blood-testing startup’s deceptions.
The 31-year-old Shultz reportedly celebrated the news of former Theranos CEO Elizabeth Holmes’ conviction on four charges of defrauding investors with champagne, joy, and a healthy dose of vindication, according to NPR.
“This story has been unfolding for pretty much my entire adult life,” Tyler Shultz (above), whistleblower in the Elizabeth Holmes fraud trial, told NPR from his parents’ home in Silicon Valley. “All of a sudden, it was just a weight was lifted. It’s over. I can’t believe it’s over,” he added. A former employee of now defunct clinical laboratory company Theranos, Shultz is CEO at Flux Biosciences, a company he co-founded. (Photo copyright: Deanne Fitzmaurice/NPR.)
Shultz Interns Briefly at Theranos
In 2011, Shultz was a biology major at Stanford University—where Elizabeth Holmes herself briefly attended—when his grandfather, former US Secretary of State George Shultz, a Theranos board member, introduced him to Holmes.
According to NPR, the younger Shultz was so impressed by the charismatic Holmes that he asked her if he could intern with Theranos after his junior year. Following his internship, he accepted a full-time position as a research engineer with Theranos, a stint that lasted only eight months. Shultz quit Theranos the day after he emailed Holmes in 2014 to alert her to failed quality-control checks and other troubling practices within the company’s clinical laboratory.
According a 2016 profile of Shultz in The Wall Street Journal (WSJ), his email to Holmes resulted in a “blistering” reply from then-Theranos President and COO Ramesh “Sunny” Balwani, who “belittled Shultz’s grasp of basic mathematics and his knowledge of laboratory science.”
Yet, Shultz told NPR, “It was clear that there was an open secret within Theranos that this technology simply didn’t exist.”
After leaving Theranos, Shultz became a key source for the WSJ’s 2015 exposé of Theranos. Using an alias, he also contacted state regulators in New York about the Theranos Edison blood-testing device’s shortcomings. In response, Theranos responded with threats of lawsuits and intimidation, the WSJ reported.
In an interview with CBS News, Shultz said, “I am happy that she was found guilty of these crimes and I feel like I got my vindication from that, and I feel good about that.”
Whistleblowers Were Critical to WSJ’s Investigation
Former WSJ reporter John Carreyrou, who authored the newspaper’s investigative series into Theranos, credits the Theranos whistleblowers for blowing the cover on the clinical lab company’s deceptions.
“I would not have been able to break this story without Rosendorff, Tyler, and Erika,” Carreyrou told NPR, referring to Shultz and two additional Theranos whistleblowers: one-time Theranos Laboratory Director Adam Rosendorff and laboratory associate Erika Cheung. “Tyler and Erika were corroborating sources, and that was absolutely critical.”
In the interview with CBS News, Tyler described the damage his role as a Theranos whistleblower caused to his relationship with his grandfather, former Secretary of State and Theranos board member George Shultz. Tyler said the elder Shultz did not believe his claims about Theranos’ regulatory deficiencies and the Edison device’s shortcomings until he neared the end of his life.
“That was extremely tough. This whole saga has taken a financial, emotional, and social toll on my relationships. The toll it took on my grandfather’s relationship was probably the worst. It is tough to explain. I had a few very honest conversations with him,” Shultz told CBS News.
While the elder Shultz never apologized to his grandson, Tyler said his grandfather ultimately acknowledged he was right.
“In one of my last conversations with him he told me a story about how he got Elizabeth invited during fleet week in San Francisco to go give a speech to United States Navy sailors. He said with tears in her eyes, she told the room about how she was so honored and humbled that her life’s work would be saving the lives of United States servicemen and women,” Shultz recalled in the CBS News interview.
“He said he could not believe that anybody could get in front of these men and women who are willing to put their lives in front of our country and lie directly to their face as convincingly as she lied,” he added.
George Shultz died in February 2021.
Jury’s Ruling on Defrauding Patients
In an interview with CNBC, Shultz said his one disappointment with the verdict was that Holmes was not found guilty of defrauding patients. Calling the patients “the real victims,” Shultz said, “I did what I did. I stuck my neck out to protect those patients, not to protect Betsy DeVos’ $100 million investment.” (The jury voted Holmes guilty on three counts of wire fraud and one count of conspiracy to commit fraud against Theranos’ investors, but not guilty on conspiracy to defraud and commit wire fraud against Theranos patients.)
Tyler Shultz was listed as a potential witness in the Holmes trial but was not called to take the stand. He—along with many clinical laboratory directors and pathologists who have closely followed the Holmes trial—will now await news of Holmes’ sentencing. Holmes could face up to 20 years in prison for each guilty verdict, but she’s likely to receive a lighter sentence.
The trail of Ramesh Balwani is expected to begin sometime in March. That trial can be expected to produce additional revelations about the problems of Theranos and how and why management is alleged to have knowingly reported inaccurate clinical laboratory test results to thousands of patients.