Clinical laboratory managers and pathology practice administrators should consider how these trends may affect their business and patients when planning for the future.
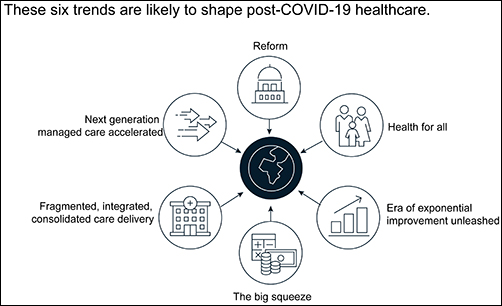
The McKinsey graphic above illustrates the “six trends that are likely to shape post-COVID-19 healthcare.” Clinical laboratories that support health networks struggling with any of these challenges should take steps to prepare for anticipated changes to healthcare delivery. (Graphic copyright: McKinsey and Company.)
1: Healthcare Reform
McKinsey identified three areas where the coronavirus pandemic may impact healthcare reform:
“COVID-19-era waivers that could become permanent.
“Actions that may be taken to strengthen the healthcare system to deal with pandemics.
“Reforms to address the COVID-19-induced crisis.”
McKinsey reports that “the Centers for Medicare and Medicaid Services has introduced more than 190 waivers since the beginning of March 2020.” These waivers can affect all aspects of healthcare, from clinical practice to reimbursement. Some of them, according to McKinsey, are “only relevant during the crisis (for example, the waiver of intensive care unit death reporting). A retrospective assessment of others (for example, expansion of telehealth access) could reveal beneficial innovation worth preserving.”
Several areas that McKinsey says are clearly ripe for reform include improving the resiliency of the healthcare system and the way the system is funded.
Public sector budgets are generally kept strictly separate, each with its own rules and policies that dictate operations. But in his article, “After COVID-19—Thinking Differently About Running the Health Care System,” published in JAMA Health Network, Stuart M. Butler, PhD, Senior Fellow in Economic Studies at the Brookings Institution, wrote, “The intensity of the COVID-19 pandemic … is forcing jurisdictions all across the country to find ways to be nimble so that multiple agencies can work together.”
Thus, McKinsey recommends, “Given the substantial shifts in relative market positioning among industry players that prior reforms have created, leaders would do well to plan ahead now.”
2: Better Access to Healthcare Services
Some people who develop COVID-19 are at far greater risk of hospitalization and death than others, including those who have:
Chronic health conditions, including obesity.
Mental and behavioral health challenges, such as substance abuse.
Unmet social needs, such as food or housing insecurity.
Poor access to healthcare.
McKinsey wrote that these “intersecting health and social conditions,” combined with certain races that have higher risk for severe complications, including Black, Indian, and Hispanic/Latino Americans, “correlated with poorer health outcomes.”
Value-based healthcare, telehealth, and greater attention to the social determinants of health may help address some of these issues, McKinsey notes, but the pandemic has shined a spotlight on how lack of care increases risk for certain populations during a public health crisis.
3: Era of Exponential Improvement Unleashed
Some of the trends that appear to be accelerating as a result of the pandemic are good news. McKinsey cites several benefits, including:
Improved understanding of patients.
Delivery of more convenient and individualized care.
$350-$410 billion in annual revenue by 2025.
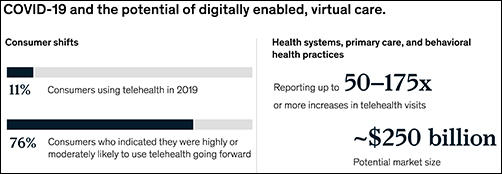
Through telehealth and other types of virtual care enabled by digital technology, “intuitive healthcare ecosystems” may arise and offer a more integrated experience for patients and their caregivers, McKinsey notes.
“While the pace of change in healthcare has lagged other industries in the past, potential for rapid improvement may accelerate due to COVID-19. An example is the exponential uptake of digitally enabled, virtual care,” McKinsey wrote. “Our analysis … showed that health systems, primary care, and behavioral health practices are reporting increases of more than 50–175 times in telehealth visits, and the potential market size for virtual care could reach around $250 billion.”
The graphic above is taken from the McKinsey and Co. report, which noted, “Proliferation of digitally enabled, virtual care could further contribute to the rise of personalized and intuitive healthcare ecosystems [that] have the potential to deliver an integrated experience to consumers, enhance productivity of providers, engage both formal and informal caregivers, and improve outcomes while lowering cost.” (Graphic copyright: McKinsey and Company.)
4: The Big Squeeze
The pandemic has caused an enormous outflow of cash from the healthcare system, and some experts don’t expect an injection of funding until 2022. “This outflow is expected to be primarily driven by coverage shifts out of employer-sponsored insurance and possible coverage reductions by employers as well as Medicaid rate pressures from states,” McKinsey states.
“We estimate that COVID-19 could depress healthcare industry earnings by between $35 billion and $75 billion compared with baseline expectations,” McKinsey predicted, adding, “Select high-growth segments will remain attractive (for example, virtual care, home health, software and platforms, specialty pharmacy) and will disproportionally drive growth. These high-growth areas are expected to increase more than 10% over the next five years, while other segments may stagnate or decline altogether.”
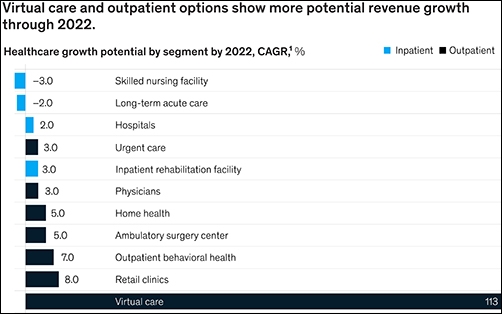
5: Fragmented, Integrated, Consolidated Care Delivery
McKinsey says, “The shift of care out of hospitals is not new but has been accelerated by COVID-19.” Rather than the hospital being the center of care delivery, patients are increasingly choosing to receive care at a range of sites across many healthcare ecosystems that are connected digitally and through analytics.
Early in the course of the pandemic, visits to ambulatory care facilities dropped nearly 60% by early April. But by mid-May, those visits were beginning to rebound.
In, “The Impact of the COVID-19 Pandemic on Outpatient Visits: A Rebound Emerges,” the Commonwealth Fund reported that “the relative decline in visits remains largest among surgical and procedural specialties and pediatrics” but is “smaller in other specialties, such as adult primary care and behavioral health.”
The McKinsey graphic above shows how “virtual care and outpatient options show more potential revenue growth through 2022.” Clinical laboratories that support those healthcare settings, especially ambulatory surgery, behavioral health, and retail clinics, should experience similar growth. (Graphic copyright: McKinsey and Company.)
6: Adoption of Next-Generation Managed Care Is Accelerating
How will COVID-19 affect the managed care industry? McKinsey says the “next generation” of managed care might use Medicare Advantage as a model.
“Payers pursuing the next generation of managed care model (through deep integration with care delivery) demonstrate better financial performance, capturing an additional 50 basis points of earnings before interest, taxes, depreciation, and amortization above expectation,” McKinsey noted, adding, “Employers and payers could consider fundamentally rethinking how employer-sponsored health coverage is structured. Learning from Medicare Advantage could provide inspiration for such a reimagination.”
What Should Clinical Laboratory Managers Do?
The McKinsey article concludes by stating, “While the challenges are numerous, leaders who seize the mindset that “disruptive change provides an opportunity to separate yourself from the pack” will build organizations meaningfully stronger than the ones they ran going into the crisis.”
The McKinsey article authors recommend that healthcare organizations take several proactive steps, including:
Launch a plan-ahead team.
Question your role and your future business model.
Prepare to transform your business.
Reimagine your organization to make faster decisions.
Take action to drive health equity.
Though the McKinsey and Company article covered healthcare in general, many of the authors’ observations and recommendations can apply to clinical laboratories and pathology groups as well and may be valuable in future planning.
Sophisticated cyberattacks have already hit hospitals and healthcare networks in Oregon, California, New York, Vermont, and other states
Attention medical laboratory managers and pathology group administrators: It’s time to ramp up your cyberdefenses. The FBI, the federal Department of Health and Human Services (HHS), and the federal Cybersecurity and Infrastructure Security Agency (CISA) issued a joint advisory (AA20-302A) warning US hospitals, clinical laboratories, and other healthcare providers to prepare for impending ransomware attacks, in which cybercriminals use malware, known as ransomware, to encrypt files on victims’ computers and demand payment to restore access.
The joint advisory, titled, “Ransomware Activity Targeting the Healthcare and Public Health Sector,” states, “CISA, FBI, and HHS have credible information of an increased and imminent cybercrime threat to US hospitals and healthcare providers.” It includes technical details about the threat—which uses a type of ransomware known as Ryuk—and suggests best practices for preventing and handling attacks.
In his KrebsOnSecurity blog post, titled, “FBI, DHS, HHS Warn of Imminent, Credible Ransomware Threat Against U.S. Hospitals,” former Washington Post reporter, Brian Krebs, wrote, “On Monday, Oct. 26, KrebsOnSecurity began following up on a tip from a reliable source that an aggressive Russian cybercriminal gang known for deploying ransomware was preparing to disrupt information technology systems at hundreds of hospitals, clinics, and medical care facilities across the United States. Today, officials from the FBI and the US Department of Homeland Security hastily assembled a conference call with healthcare industry executives warning about an ‘imminent cybercrime threat to US hospitals and healthcare providers.’”
Krebs went on to reported that the threat is linked to a notorious cybercriminal gang known as UNC1878, which planned to launch the attacks against 400 healthcare facilities.
Clinical Labs, Pathology Groups at Risk Because of the Patient Data They Keep
Hackers initially gain access to organizations’ computer systems through phishing campaigns, in which users receive emails “that contain either links to malicious websites that host the malware or attachments with the malware,” the advisory states. Krebs noted that the attacks are “often unique to each victim, including everything from the Microsoft Windows executable files that get dropped on the infected hosts to the so-called ‘command and control’ servers used to transmit data between and among compromised systems.”
Charles Carmakal, SVP and Chief Technology Officer of cybersecurity firm Mandiant told Reuters, “UNC1878 is one of the most brazen, heartless, and disruptive threat actors I’ve observed over my career,” adding, “Multiple hospitals have already been significantly impacted by Ryuk ransomware and their networks have been taken offline.”
John Riggi (above), senior cybersecurity adviser to the American Hospital Association (AHA), told the AP, “We are most concerned with ransomware attacks which have the potential to disrupt patient care operations and risk patient safety. We believe any cyberattack against any hospital or health system is a threat-to-life crime and should be responded to and pursued as such by the government.” Hospital-based medical laboratories and independent clinical laboratories that interface with hospital networks should be assess their vulnerability to cyberattacks and take appropriate steps to protect their patients’ data. (Photo copyright: American Hospital Association.)
Multiple Healthcare Provider Networks Under Attack
Hospitals in Oregon, California, and New York have already been hit by the attacks, Reuters reported. “We can still watch vitals and getting imaging done, but all results are being communicated via paper only,” a doctor at one facility told Reuters, which reported that “staff could see historic records but not update those files.”
Some of the hospitals that have reportedly experienced cyberattacks include:
In October, the Associated Press (AP) reported that a recent cyberattack disrupted computer systems at six hospitals in the University of Vermont (UVM) Health Network. The FBI would not comment on whether that attack involved ransomware, however, it forced the UVM Medical Center to shut down its computer system and reschedule elective procedures.
Threat intelligence analyst Allan Liska of US cybersecurity firm Recorded Future told Reuters, “This appears to have been a coordinated attack designed to disrupt hospitals specifically all around the country.”
He added, “While multiple ransomware attacks against healthcare providers each week have been commonplace, this is the first time we have seen six hospitals targeted in the same day by the same ransomware actor.”
An earlier ransomware attack in September targeted 250 healthcare facilities operated by Universal Health Services Inc. (UHS). A clinician at one facility reported “a high-anxiety scramble” where “medical staff could not easily see clinical laboratory results, imaging scans, medication lists, and other critical pieces of information doctors rely on to make decisions,” AP reported.
Outside of the US, a similar ransomware attack in October at a hospital in Düsseldorf, Germany, prompted a homicide investigation by German authorities after the death of a patient being transferred to another facility was linked to the attack, the BBC reported.
CISA, FBI, HHS, Advise Against Paying Ransoms
To deal with the ransomware attacks, CISA, FBI, and HHS advise against paying ransoms. “Payment does not guarantee files will be recovered,” the advisory states. “It may also embolden adversaries to target additional organizations, encourage other criminal actors to engage in the distribution of ransomware, and/or fund illicit activities.” The federal agencies advise organizations to take preventive measures and adopt plans for coping with attacks.
The advisory suggests:
Training programs for employees, including raising awareness about ransomware and phishing scams. Organizations should “ensure that employees know who to contact when they see suspicious activity or when they believe they have been a victim of a cyberattack.”
Regular backups of data and software. These should be “maintained offline or in separated networks as many ransomware variants attempt to find and delete any accessible backups.” Personnel should also test the backups.
Continuity plans in case information systems are not accessible. For example, organizations should maintain “hard copies of digital information that would be required for critical patient healthcare.”
“Without planning, provision, and implementation of continuity principles, organizations may be unable to continue operations,” the advisory states. “Evaluating continuity and capability will help identify continuity gaps. Through identifying and addressing these gaps, organizations can establish a viable continuity program that will help keep them functioning during cyberattacks or other emergencies.”
Dark Daily Publisher and Editor-in-Chief, Robert Michel, suggests that clinical laboratories and anatomic pathology groups should have their cyberdefenses assessed by security experts. “This is particularly true because the technologies and methods used by hackers change rapidly,” he said, “and if their laboratory information systems have not been assessed in the past year, then this proactive assessment could be the best insurance against an expensive ransomware attack a lab can purchase.”
Breakthrough assay a ‘tenfold improvement over any prior assay for TERT mutations in the blood for brain tumors,’ MGH says in an affirmation of a diagnostic technology clinical labs might soon use
In recent years, investors have poured tens of millions of dollars into companies that promised to create non-invasive cancer tests which use liquid biopsy technology. Medical laboratory scientists even watched some of these companies hype their particular liquid biopsy tests before clinical studies generated data demonstrating that these tests produced accurate, reliable, and reproducible results.
For diagnosing cancer, a liquid biopsy test typically uses a blood sample with the goal of finding and identifying circulating tumor cells. Harvard Medical School researchers at Massachusetts General Hospital (MGH) believe they have developed just such a blood test. Their assay utilizes an enhanced form of liquid biopsy to detect and monitor one of the more prevalent types of brain tumor in adults—a glioma—and, according to a Harvard news release, can detect the presence of glioma at a significantly higher “overall sensitivity” than other similar liquid-biopsy tests.
Gliomas start in glia cells contained in the brain or spine. They account for about 30% of all brain and central nervous system tumors and 80% of all malignant brain tumors.
During their study, MGH researchers compared blood samples and tumor biopsy tissues from patients diagnosed with a glioma. They discovered that an assay they developed—a droplet digital polymerase chain reaction (ddPCR) blood test—could detect and monitor two types of telomerase reverse transcriptase (TERT) promoter gene mutations—C228T and C250T. These two gene mutations promote cancer growth and are present in more than 60% of all gliomas. The mutations are also present in 80% of all high-grade gliomas, which are the most aggressive and life-threatening types of the cancer.
In the press release, instructor in Neurosurgery at MGH and one of the study’s authors, Leonora Balaj, PhD, said, “By ‘supercharging’ our ddPCR assay with novel technical improvements, we showed for the first time that the most prevalent mutation in malignant gliomas can be detected in blood, opening a new landscape for detection and monitoring of the tumors.”
Bob Carter, MD, PhD (above), is neurosurgical oncologist and Chief of Neurosurgery at MGH, a Professor of Neurosurgery at Harvard Medical School, and one of the study’s authors. In the MGH press release he said, “We envision the future integration of tests like this one into the clinical care of our patients with brain tumors. For example, if a patient has a suspected mass on MRI scanning, we can take a blood sample before the surgery and assess the presence of the tumor signature in the blood and then use this signature as a baseline to monitor as the patient later receives treatment, both to gauge response to the treatment and gain early insight into any potential recurrence.” What Carter describes is precision medicine and could open new diagnostic opportunities for anatomic pathology groups and clinical laboratories. (Photo copyright: Massachusetts General Hospital.)
MGH’s Ten-Fold Improvement over Previous ddPCR Assays
A liquid biopsy is the sampling and analysis of non-solid tissue in the body—primarily blood. MGH’s liquid-biopsy method detects cancer by examining fragments of tumor DNA circulating in the bloodstream. Since the technique is mostly non-invasive, tests can be performed more frequently to track tumors and mutations and monitor treatment progression. Prior to this new method, brain tumors had been difficult to detect using liquid biopsies.
“Liquid biopsy is particularly challenging in brain tumors because mutant DNA is shed into the bloodstream at a much lower level than any other types of tumors,” Balaj said in the press release.
However, MGH’s new ddPCR assay has an overall sensitivity rate of 62.5% and a specificity of 90%, which represents a tenfold improvement over prior assays for TERT mutations in the blood.
And when testing the performance of the ddPCR assay in tumor tissue, the MGH researchers discovered their results were the same as results from a previous independently-performed clinical laboratory assessment of TERT mutations within collected tumor specimens. They also found that their assay could detect TERT mutations when looking at blood plasma samples collected at other facilities.
The researchers believe that their test could be performed in most clinical laboratories and can be utilized to follow the course of disease in cancer patients. The MGH researcher’s goal is to expand and adapt the blood test to diagnose, differentiate, and monitor other types of brain tumors in addition to gliomas.
Of course, more research will be needed before MGH’s new assay can become a vital tool in the fight against disease. However, this type of genetic analysis may soon provide pathologists with new techniques to more accurately diagnose and monitor cancers, and to provide healthcare providers with valuable data regarding which therapies would be the most beneficial for individual patients, a key element of precision medicine.
Critical shortages in medical laboratory workers and supplies are yet to be offset by new applicants and improved supply chains. But there is cause for hope.
Medical laboratory scientists (aka, medical technologists) can be hard to find and retain under normal circumstances. During the current coronavirus pandemic, that’s becoming even more challenging. As demand for COVID-19 tests increases, clinical laboratories need more technologists and lab scientists with certifications, skills, and experience to perform these complex assays. But how can lab managers find, attract, and retain them?
The Johns Hopkins Coronavirus Resource Center reports that as of mid-October more than one million tests for SARS-CoV-2 were being performed daily in the US. And as flu season approaches, the pandemic appears to be intensifying. However, supply of lab technologists remains severely constrained, as it has been for a long time.
Still, qualified medical technologists (MT) and clinical laboratory scientists (CLS) are hard to find.
Demand for COVID Tests Exceeds Available Clinical Lab Applicants
“I can replace hardware and I can manage not having enough reagents, but I can’t easily replace a qualified [medical] technologist,” said David Grenache, PhD, Chief Scientific Officer at TriCore Reference Laboratories, Albuquerque, N.M., in the WSJ.
Another area where demand outstrips supply is California. Megan Crumpler, PhD, Laboratory Director, Orange County Public Health Laboratory, told the WSJ, “We are constantly scrambling for personnel, and right now we don’t have a good feel about being able to fill these vacancies, because we know there’s not a pool of applicants.”
Are Reductions in Academic Programs Responsible for Lack of Available Lab Workers?
Recent data from the US Bureau of Labor Statistics (BLS) show 337,800 clinical laboratory technologists and technicians employed by hospitals, public health, and commercial labs, with Job Outlook (projected percent change in employment) growing at 7% from 2019 to 2029. This, according to the BLS’ Occupational Outlook Handbook on Clinical Laboratory Technologists and Technicians, is “faster than average.”
“The average growth rate for all occupations is 4%,” the BLS notes.
Medical laboratories have the most staff vacancies in phlebotomy (13%) and the least openings in point-of-care (4%), according to an American Society for Clinical Pathology 2018 Vacancy Survey published in the American Journal of Clinical Pathology (AJCP).
Becker’s Hospital Review reported that “Labor shortages in [clinical] testing labs have existed for years due to factors including low recruitment, an aging workforce, and relatively low pay for [medical] lab technicians and technologists compared to that of other healthcare workers with similar education requirements.
“In 2019, the median annual salary for clinical laboratory technologists and technicians was $53,000, according to the US Bureau of Labor Statistics. The skills required for lab workers also are often specialized and not easily transferred from other fields.”
At the “root” of the problem, according to an article in Medical Technology Schools, is a decrease in available academic programs. Laboratory technologists require a Bachelor of Science (BS) degree and technicians need an associate degree or post-secondary certificate.
“(The programs) are expensive to offer, so when it comes to cuts and budgets, some of those cuts have been based on how much it costs to run them. That, and they may not have high enough enrollments,” said Lisa Cremeans, MMDS, CLS(NCA), MLS(ASCP), Clinical Assistant Professor at University of North Carolina at Chapel Hill, in the Medical Technology Schools article. (Photo copyright: University of North Carolina.)
AACC has called for federal funding of these programs, which now number 608, down from 720 programs for medical laboratory scientists in 1990.
“The pandemic has shone a spotlight on how crucial testing is to patient care. It also has revealed the weak points in our country’s [clinical laboratory] testing infrastructure, such as the fact that the US has allowed the number of laboratory training programs to diminish for years now,” said Grenache, who is also AACC President, in a news release.
Creative Staffing Strategies Clinical Labs Can Take Now
select “apply code” and complete the registration.
How Some Clinical Labs are Coping with Staff and Recruitment Challenges
The Arizona Chamber Business News reported that Sonora Quest Laboratories in Tempe earlier this year launched “Operation Catapult” to help with a 60,000 COVID-19 test increase in daily test orders. The strategy involved hiring 215 employees and securing tests with the help of partners:
Meanwhile, students in the UMass Lowell (UML) medical laboratory science (MLS) program, see brighter skies ahead.
“The job outlook even before COVID-19 was so amazing,” said Dannalee Watson, a UML MLS student, in a news release. “It’s like you’re figuring out a puzzle with your patient. Then, we help the doctor make decisions.”
Such enthusiasm is refreshing and reassuring. In the end, the SARS-CoV-2 pandemic and the resultant demand for clinical laboratory testing may call more students’ attention to careers in medical laboratories and actually help to solve the lab technologist/technician shortage. We can hope.
About 50% of South Asians and 16% of Europeans carry gene cluster associated with respiratory failure after SARS-CoV-2 infection and hospitalization
Clinical pathology laboratories and medical laboratory scientists may be intrigued to learn that scientists from two research institutes in Germany and Sweden have determined that a strand of DNA associated with a higher risk of severe COVID-19 in humans is similar to the corresponding DNA sequences of a roughly 50,000-year-old Neanderthal from Croatia.
The researchers concluded that this gene cluster—passed down from Neanderthals to homo sapiens—triples the risk of developing severe COVID-19 respiratory symptoms for some modern day humans.
In a press release, Pääbo said, “It is striking that the genetic heritage from the Neanderthals has such tragic consequences during the current pandemic. Why this is must now be investigated as quickly as possible.”
Might Useful Biomarkers for Clinical Laboratory Tests Be Identified?
Though it is not immediately clear how these findings may alter current approaches to developing treatments and a vaccine for the SARS-CoV-2 coronavirus, it is another example of how increased knowledge of human DNA leads to new understandings about genetic sequences that can spur development of useful biomarkers for clinical laboratory diagnostics tests.
Swedish geneticist Svante Pääbo, PhD (above right), Director of the Max Planck Institute for Evolutionary Anthropology in Germany, is co-author of a recent study that traced a gene cluster linked to a higher risk of severe COVID-19 to 50,000-year-old Neanderthals from Croatia. “It is striking that the genetic heritage from the Neanderthals has such tragic consequences during the current pandemic,” he said. Nevertheless, such discoveries sometimes lead to new biomarkers for clinical laboratory tests and diagnostics. (Photo copyright: Max Planck Institute for Evolutionary Anthropology.)
This latest research reveals that people who inherit a specific six-gene combination on chromosome 3—called a haplotype—are three times more likely to need artificial ventilation if they are infected by the SARS-CoV-2 coronavirus. Yet, the researchers can only speculate as to why the gene cluster confers a higher risk.
“The genes in this region may well have protected the Neanderthals against some other infectious diseases that are not around today. And now, when we are faced with the [SARS-CoV-2] coronavirus, these Neanderthal genes have these tragic consequences,” Pääbo told the Guardian.
According to the study, the gene risk variant is most common in South Asia where about half of the population carries the Neanderthal risk variant. In comparison, one in six Europeans have inherited the gene sequence and the trait is almost nonexistent in Africa and East Asia.
“About 63% of people in Bangladesh have at least one copy of the disease-associated haplotype, and 13% have two copies (one from their mother and one from their father). For them, the Neandertal DNA might be partially responsible for increased mortality from a coronavirus infection. People of Bangladeshi origin living in the United Kingdom, for instance, are twice as likely to die of COVID-19 as the general population,” Science News reported.
Other Research Connecting Genes to Severe COVID-19 Symptoms
The haplotype on chromosome 3 first made headlines in June when the New England Journal of Medicine (NEJM) published the “Genomewide Association Study of Severe COVID-19 with Respiratory Failure,” which analyzed COVID-19 patients in seven hospitals in Italy and Spain. The researchers found an association between the gene cluster on chromosome 3 and severe symptoms of SARS-CoV-2 after infection and hospitalization. The study also pointed to the potential involvement of chromosome 9, which contains the ABO blood-group system gene, indicating that humans with type A blood may have a 45% higher risk of developing severe COVID-19 infections.
However, Mark Maslin, PhD, Professor of Climatology at University College London, cautions against drawing strong conclusions from the initial research tying disease risk to the genetic legacy of Neanderthals, the Guardian reported. He suggested that, while the Neanderthal-derived variant may contribute to COVID-19 risk in certain populations, genes are more likely to be just one of multiple risk factors for COVID-19 that include age, gender, and pre-existing conditions.
“COVID-19 is a complex disease, the severity of which has been linked to age, gender, ethnicity, obesity, health, virus load among other things,” Maslin told the Guardian. “This paper links genes inherited from Neanderthals with a higher risk of COVID-19 hospitalization and severe complications. But as COVID-19 spreads around the world it is clear that lots of different populations are being severely affected, many of which do not have any Neanderthal genes.
“We must avoid simplifying the causes and impact of COVID-19, as ultimately a person’s response to the disease is about contact and then the body’s immunity response, which is influenced by many environmental, health and genetic factors.”
Andre Franke, PhD, Director of the Institute of Clinical Molecular Biology, Kiel University in Germany, agrees with Maslin, the Associated Press reported. In a statement “ahead of the study’s final publication,” he said these latest findings have no immediate impact on the treatment of COVID-19, and he questioned “why that haplotype—unlike most Neanderthal genes—survived until today,” AP reported.
All of this deepens the mystery of the SARS-CoV-2 coronavirus. Genomics research continues to add new insights into what is known about COVID-19 and may ultimately provide answers on why some people contract the disease and remain asymptomatic—or have mild symptoms—while others become seriously ill or die. Understanding why and how certain genes increase the risk of severe COVID-19 could give rise to targeted clinical laboratory tests and therapies to fight the disease.
Clinical laboratory managers may want to follow the debate that surfaced shortly after publication of the study in a peer-reviewed journal, when editors of the journal issued concerns over the researchers’ claims
Virologists and medical laboratory scientists continue to investigate ways the SARS-CoV-2 coronavirus can be defeated using the body’s own defenses in conjunction with medical treatments and a possible vaccine. Now, researchers at the Boston University School of Medicine have discovered that higher levels of vitamin D in the blood may improve chances of recovering from a COVID-19 infection.
“This study provides direct evidence that Vitamin D sufficiency can reduce the complications, including the cytokine storm (release of too many proteins into the blood too quickly) and ultimately death from COVID-19,” Michael F. Holick, PhD, MD, Professor of Medicine, Physiology and Biophysics at Boston University School of Medicine and one of the authors of the study, told SciTechDaily.
Holick is well-known in the scientific community for his many published studies on Vitamin D. In 2018, Kaiser Health News and The New York Times published a retrospective on Holick and his advocacy on behalf of Vitamin D, titled, “The Man Who Sold America On Vitamin D—and Profited in the Process.” In that story, Holick acknowledged working as a consultant for several organizations, including Quest Diagnostics in a relationship that dates back to 1979. KHN and NYT noted that Quest Diagnostics performs Vitamin D tests.
The Boston University researchers published their study in PLOS ONE, a peer-reviewed open-access scientific journal published by the Public Library of Science (PLOS). The paper’s apparent conclusions, however, invoked an “expression of concern” from the journal’s editors, which, along with direct responses from the Boston University researchers, can be read on PLOS ONE.
Can Vitamin D Save Lives?
To perform their research, the Boston University researchers examined the Vitamin D levels of 235 patients who had been admitted to a hospital with a SARS-CoV-2 infection. The patients were then tracked for clinical outcomes, including:
Blood samples were also analyzed for the number of lymphocytes and inflammatory markers. The researchers compared the collected data between patients who were sufficient to those who were deficient in Vitamin D levels.
They determined that patients over the age of 40 who were Vitamin D sufficient were 51.5% less likely to die from a COVID-19 infection than those who were deficient in the vitamin.
“Because Vitamin D deficiency and insufficiency is so widespread in children and adults in the United States and worldwide, especially in the winter months, it is prudent for everyone to take a vitamin D supplement to reduce risk of being infected and having complications from COVID-19,” Michael F. Holick, PhD, MD (above), told SciTechDaily. The Boston University School of Medicine professor and study author has been praising the health benefits of Vitamin D for years. He played a role in drafting national guidelines for the vitamin and also authored books that tout the advantages of Vitamin D, the importance of UV rays, and the biologic effects of light. (Photo copyright: Boston Herald.)
How Vitamin D Works and Why It’s So Important
In a fact sheet, the National Institutes of Health (NIH) recommend that adults between the ages of 19 and 70 take 15 micrograms (mcg) or 600 International Units (IU) of Vitamin D per day. Adults over the age of 70 should increase that amount to 20 mcg or 800 IUs per day.
According NBC News, Americans spent $936 million on supplements in 2017, which was nine times more than the previous decade. That article also stated that medical laboratory testing for Vitamin D levels have exponentially increased over the years. More than 10 million tests for Vitamin D levels were ordered for Medicare patients in 2016 at a cost of $365 million, which represents an increase of 547% since 2007. Currently, approximately one in four adults over the age of 60 in the US take Vitamin D supplements.
The NIH fact sheet notes that Vitamin D is a nutrient found in cells throughout the body and is needed for good health and to maintain strong bones. Individuals who are deficient in Vitamin D may develop soft, thin, brittle bones, as well as rickets in children and osteomalacia in adults. Vitamin D also helps the immune system fight off invading bacteria and viruses, helps nerves carry messages between the brain and other body parts, and helps muscles move. It can also play a role in warding off osteoporosis in older adults.
Very few foods naturally contain Vitamin D. The best dietary sources for the vitamin are fatty fish such as salmon, tuna, and mackerel, and foods fortified with Vitamin D, such as milks, some breakfast cereals, and yogurt. Being outside on sunny days is another way to obtain Vitamin D, as the body makes the vitamin when skin is directly exposed to the sun.
The Boston University study outlines the advantages of having sufficient Vitamin D levels, as well as how the vitamin may help ward off and possibly lessen the effects of infections like COVID-19, though those conclusions have been called into question.
Nevertheless, individuals who are deficient in the vitamin may want to take a supplement or get plenty of sunshine, just to be on the safe side. And clinical laboratory managers will want to keep in mind that over the years “the steady increase in physician and patient demand for Vitamin D tests has kept most clinical and pathology laboratories scrambling to maintain turnaround times and quality,” which Dark Daily reported in “Why Vitamin D Continues to Be the World’s Fastest-Growing Clinical Laboratory Test.”