Proven success at providing quality care to patients at home while lowering costs has both investors and health insurance companies intrigued
Some call it “hospital in the home.” Whatever name it is given, the high cost of keeping a patient overnight in a hospital is motivating a range of healthcare players to develop innovative ways to provide care to patients—even patients with acute conditions—in their home. This is a trend that clinical laboratories will want to watch.
With hospital beds costing $1,000 to $2,000 per night, the
economics of being treated in the comfort of their homes can be attractive to
patients. But it’s also popular with caregivers, investors, and payers, as well.
That’s why in-home healthcare services are becoming increasingly common
nationwide, and why clinical laboratories may be supplying services to more in-home
healthcare companies in the future.
One such company is DispatchHealth of Denver, Colo., which recently brought its “ER-at-Home” in-home healthcare model to cities in Texas, Massachusetts, and Washington State.
Focused primarily on seniors with high-acuity medical conditions, “Patients or caregivers contact DispatchHealth through their smartphone app, website, or phone call line and the company sends over a home care team consisting of a physician assistant or nurse practitioner, along with an [emergency] medical technician. The team has the ability to perform clinical laboratory studies, infusion, EKGs, and some higher-level procedures, such as the repair of complex lacerations,” MedCity News reported.
The DispatchHealth team arrives prepared to treat Influenza
(Flu), fever, joint or back pain, sprains, strains, eye infections, urinary
tract infections, skin rashes, and lacerations. The team also can treat more
severe conditions that cause nausea, vomiting, and diarrhea, as well as asthma
and other respiratory conditions, and illnesses of the ear, nose, and throat.
In addition, the DispatchHealth team can perform certain
clinical laboratory tests onsite, including:
High-acuity home care is a development that clinical
laboratory leaders will want to monitor because these services save people
trips to medical laboratories, urgent care centers, primary care doctors’
offices, and even emergency rooms.
“We strive to treat conditions between the ER and true emergencies—so COPD (chronic obstructive pulmonary disease) exacerbation, pneumonia, severe migraines, and other issues we can treat with IV (intravenous therapy) medication … and laboratory studies,” Mark Prather, MD, DispatchHealth Chief Executive Officer, told MedCity News, which noted the company’s partnership with Centura Health, Colorado Springs, Colo., among others.
Established in 2013 in Denver, DispatchHealth provides both
mobile and virtual healthcare, is in-network with healthcare insurance
companies, and has relationships with healthcare systems.
The company expanded this year into new markets and added
partnerships with more healthcare systems, including:
a “major nonprofit health system” in North Texas, according to a news release.
Through in-home care teams (such as shown above), DispatchHealth estimates delivery of acute care to about 80,000 patients nationwide in 2019 for a savings of $100 million in medical expenses. “Up to 50% of people who visit the emergency room every day could be treated in a lower cost setting,” said DispatchHealth Chief Executive Officer Mark Prather, MD, in a news release. (Photo copyright: Philips.)
In the Spokane market, the company’s six teams and two vehicles can see about seven patients per day for an average of 45 minutes to an hour per visit, reported the Spokesman-Review. DispatchHealth employs more than 200 people and has raised more than $33 million in growth capital financing, according to a company statement.
The project involved and recognized medical practices that
effectively and efficiently cared for Medicare beneficiaries with chronic
conditions at home.
More recently, Northwell Health Labs, a division of Northwell Health, launched LabFly, a smartphone app that enables patients to schedule blood draws at home or at work, according to a news release.
“The app is a new way to give our patients access to the quality experience they would receive at one of our patient service centers, but in their living room or place of work,” said Dwayne Breining, MD, Executive Director, Northwell Health Labs, in the news release.
Investors Are Intrigued with In-Home Care
The business of treating people in their homes or offices
has some investors excited at the opportunity.
“To us, this feels like we’re investing in Uber in 2010. This is going to revolutionize and change the entire healthcare industry,” Samir Patel, Principal and co-founder of IRA Capital told the New York Times. Patel was commenting on his firm’s investment in Heal, a Los Angeles-based in-home healthcare company that launched in 2014.
In response to being contacted by smartphone app, computer, or phone, Heal sends primary care doctors and medical assistants to treat people in their homes, workplace, or at hotels.
Heal estimates completion of more than 100,000 house calls in 2019 and savings in healthcare expenses of more than $53 million due to treating people in lower cost ways, a news release stated. The company said it has experienced a 310% growth rate over 12 months and now operates in Atlanta, Georgia, California, New York, North Virginia, and the District of Columbia.
“Ten years from now, we will think of going to the doctor’s office as dated and arbitrary as going to the store to buy diapers compared to buying diapers on Amazon,” Nick Desai, co-founder of Heal, told FierceHealthcare, which reported Heal had raised $71 million from investors.
Payers Are Onboard as Well
High-acuity home care services also seem to align with health insurance company benefits and new federal payment models. Heal’s website states their services are in-network with most Medicare Advantage plans. Heal’s smartphone app also can verify insurance coverage.
DispatchHealth explains on its website that it contracts
with major payers, including Medicare and Medicaid, and charges self-pay
customers $275.
Medical laboratory leaders should consider developing
relationships with high-acuity home healthcare companies and other care
providers that deliver care to people in unconventional ways and in
non-traditional locations.
Though medical laboratory testing is key to confirming sepsis, predictive analytics systems can identify early indications and alert caregivers, potentially saving lives
Medical laboratory testing has long been the key element in hospitals’ fight to reduce deaths caused by sepsis, a complication caused by the human body’s response to infection which can injure organs and turn fatal. But clinical laboratory testing takes time, particularly if infectious agents must be cultured in the microbiology lab. And sepsis acts so quickly, by the time the condition is diagnosed it is often too late to prevent the patient’s death.
One example is HCA Healthcare (NYSE:HCA), the for-profit corporation with 185 hospitals, 119 freestanding surgery centers, and approximately 2,000 sites of care in 21 US states and in the United Kingdom.
HCA employs an electronic information and alert system called SPOT (Sepsis Prediction and Optimization of Therapy), which is embedded in each hospital patient’s electronic health record (EHR).
SPOT receives clinical data in real time directly from
monitoring equipment at the patient’s bedside and uses predictive analytics to examine
the data, including medical laboratory test results. If the data indicate that
sepsis is present, SPOT alerts physicians and other caregivers.
With SPOT, HCA’s physicians have been detecting sepsis in
its earliest stages and saving lives. This lends support to the growing belief
that AI and machine learning can improve speed to diagnosis and diagnostic
accuracy, which Dark Daily has covered in multiple
e-briefings.
SPOT displays its data on screens that are monitored 24/7 (shown above). The clinical data include the patient’s vital signs as well as medical laboratory test results and nursing reports. HCA says the system has been used on about 2.5 million patients and has helped save up to 8,000 lives, Business Wire reported. (Photo copyright: HCA.)
Code Sepsis
HCA began developing the software in 2016. It was initially deployed in 2018 at TriStar Centennial Medical Center, HCA’s flagship hospital in Nashville,The Tennessean reported. It is now installed in most of the hospitals owned or operated by HCA.
Michael Nottidge, MD, is ICC Division Medical Director for Critical Care at HCA Healthcare Physician Services Group, and a critical care physician at TriStar Centennial. Nottidge told The Tennessean that unlike a heart attack or stroke, “sepsis begins quietly, then builds into a dangerous crescendo.”
Since its implementation, “[SPOT] has alerted clinicians to
a septic patient nearly every day, often hours sooner than they would have been
detected otherwise,” Nottidge told The Tennessean.
HCA’s SPOT system uses machine learning to ingest “millions of data points on which patients do and do not develop sepsis,” according to an HCA blog post. “Those computers monitor clinical data every second of a patient’s hospitalization. When a pattern of data consistent with sepsis risk occurs, it will signal with an alert to trained technicians who call a ‘code sepsis.’”
More Accurate than Clinicians
The federal Centers for Disease Control and Prevention (CDC) estimates that more than 250,000 Americans die from sepsis each year. The Sepsis Alliance describes the life-threatening complication as the “leading cause of death in US hospitals.”
Early detection and treatment are key to reducing sepsis mortalities. However, a study in the journal Clinical Medicine reported that, despite recent advances in identifying at-risk patients, “there is still no molecular signature able to diagnose sepsis.”
And according to a study published in Critical Care Medicine, the survival rate is about 80% when treatment is administered in the first hour, but each hour of delay in treatment decreases the average survival rate by 7.6%.
In an interview with Becker’s Hospital Review, HCA’s Chief Medical Officer and President of Clinical Services, Jonathan Perlin, MD, PhD, touted SPOT’s reliability, having “very few false positives. In fact, it is more than 50% more accurate at excluding patients who don’t have sepsis than even the best clinician.”
Perlin also told The Tennessean that SPOT can detect
sepsis “about eight to 10 hours before clinicians ever could.”
“It’s no coincidence that we call the technology ‘SPOT’—a common name for a child’s dog—because it really does act as our sepsis sniffer,” said Jonathan Perlin, MD, PhD (above), in the HCA blog post. “The whole point is for it to sniff smoke and put the ‘fire’ out before it becomes catastrophic. With SPOT, we’re identifying at least one-third more cases of sepsis that would not previously have come to caregivers’ attention until it was too late.” [Photo copyright: Nashville Business Journal.)
Other Healthcare Providers Using AI-Enabled Early-Warning
Tools
In November 2018, the emergency department at Duke University Hospital in Durham, N.C., began a pilot program to test an AI-enabled system dubbed Sepsis Watch, reported Health Data Management. The software, developed by the Duke Institute for Health Innovation, “was trained via deep learning to identify cases based on dozens of variables, including vital signs, medical laboratory test results, and medical histories,” reported IEEE Spectrum. “In operation, it pulls information from patients’ medical records every five minutes to evaluate their conditions, offering intensive real-time analysis that human doctors can’t provide.”
Earlier this year, Sentara Norfolk General Hospital in Norfolk, Va., installed an AI-enabled sepsis-alert system developed by Jvion, a maker of predictive analytics software. “The new AI tool grabs about 4,500 pieces of data about a patient that live in the electronic record—body temperature, heart rate, blood tests, past medical history, gender, where they live and so on—and runs it all through an algorithm that assesses risk for developing sepsis,” reported The Virginian Pilot.
Geisinger Health System, which operates 13 hospitals in Pennsylvania and New Jersey, is working on its own system to identify sepsis risk. It announced in a September news release that it had teamed with IBM to develop a predictive model using a decade’s worth of data from thousands of Geisinger patients.
“The model helped researchers identify clinical biomarkers associated with higher rates of mortality from sepsis by predicting death or survival of patients in the test data,” Geisinger stated in the news release. “The project revealed descriptive and clinical features such as age, prior cancer diagnosis, decreased blood pressure, number of hospital transfers, and time spent on vasopressor medicines, and even the type of pathogen, all key factors linked to sepsis deaths.”
So, can artificial intelligence and predictive analytics
added to medical laboratory test results help prevent sepsis-related deaths in
all hospitals? Perhaps so. Systems like SPOT, Sepsis Watch, and others
certainly are logging impressive results.
It may not be long before similar technologies are aiding
pathologists, microbiologists, and clinical laboratories achieve improved
diagnostic and test accuracy as well.
The self-cleaning material has been proven to repel even the deadliest forms of antibiotic resistant (ABR) superbugs and viruses. This ultimate non-stick coating is a chemically treated form of transparent plastic wrap which can be adhered to surfaces prone to gathering germs, such as door handles, railings, and intravenous therapy (IV) stands.
“We developed the wrap to address the major threat that is posed by multi-drug resistant bacteria,” Leyla Soleymani, PhD, Associate Professor at McMaster University and one of the leaders of the study, told CNN. “Given the limited treatment options for these bugs, it is key to reduce their spread from one person to another.”
According to research published in the peer-reviewed Southern Medical Journal, “KPC-producing bacteria are a group of emerging highly drug-resistant Gram-negative bacilli causing infections associated with significant morbidity and mortality.”
Were those surfaces covered in this new bacterial-resistant
coating, life-threatening infections in hospital ICUs could be prevented.
Taking Inspiration from Nature
In designing their new anti-microbial wrap, McMaster researchers took their inspiration from natural lotus leaves, which are effectively water-resistant and self-cleaning thanks to microscopic wrinkles that repel external molecules. Substances that come in contact with surfaces covered in the new non-stick coating—such as a water, blood, or germs—simply bounce off. They do not adhere to the material.
The “shrink-wrap” is flexible, durable, and inexpensive to
manufacture. And, the researchers hope to locate a commercial partner to
develop useful applications for their discovery.
“We’re structurally tuning that plastic,” Soleymani told SciTechDaily. “This material gives us something that can be applied to all kinds of things.”
In the video above, Leyla Soleymani, PhD, Associate Professor at McMaster University, explains how “The new plastic surface—a treated form of conventional transparent wrap—can be shrink-wrapped onto door handles, railings, IV stands, and other surfaces that can be magnets for bacteria such as MRSA and C. difficile. This may be technology that has great value to clinical laboratories and microbiology laboratories. Click here to watch the video. (Image and video copyright: McMaster University/YouTube.)
Industries Outside of Healthcare Also Would Benefit
According to the US Centers for Disease Control and Prevention (CDC), at least 2.8 million people get an antibiotic-resistant infection in the US each year. More than 35,000 people die from these infections, making it one of the biggest health challenges of our time and a threat that needs to be eradicated. This innovative plastic coating could help alleviate these types of infections.
And it’s not just for healthcare. The researchers said the coating could be beneficial to the food industry as well. The plastic surface could help curtail the accidental transfer of bacteria, such as E. coli, Salmonella, and Listeria in food preparation and packaging, according to the published study.
“We can see this technology being used in all kinds of institutional and domestic settings,” Tohid Didar, PhD, Assistant Professor at McMaster University and co-author of the study, told SciTechDaily. “As the world confronts the crisis of anti-microbial resistance, we hope it will become an important part of the anti-bacterial toolbox.”
Clinical laboratories also are tasked with preventing the
transference of dangerous bacteria to patients and lab personnel. Constant
diligence in application of cleaning protocols is key. If this new anti-bacterial
shrink wrap becomes widely available, medical laboratory managers and
microbiologists will have a new tool to fight bacterial contamination.
Experts list the top challenges facing widespread adoption of proteomics in the medical laboratory industry
Year-by-year, clinical
laboratories find new ways to use mass spectrometry to
analyze clinical specimens, producing results that may be more precise than
test results produced by other methodologies. This is particularly true in the
field of proteomics.
However, though mass spectrometry is highly accurate and
fast, taking only minutes to convert a specimen into a result, it is not fully
automated and requires skilled technologists to operate the instruments.
Thus, although the science of proteomics is advancing
quickly, the average pathology laboratory isn’t likely to be using mass
spectrometry tools any time soon. Nevertheless, medical
laboratory scientists are keenly interested in adapting mass spectrometry
to medical lab test technology for a growing number of assays.
Molly Campbell, Science Writer and Editor in Genomics, Proteomics, Metabolomics, and Biopharma at Technology Networks, asked proteomics experts “what, in their opinion, are the greatest challenges currently existing in proteomics, and how can we look to overcome them?” Here’s a synopsis of their answers:
Lack of High Throughput Impacts Commercialization
Proteomics isn’t as efficient as it needs to be to be
adopted at the commercial level. It’s not as efficient as its cousin genomics. For it to become
sufficiently efficient, manufacturers must be involved.
John Yates
III, PhD, Professor, Department of Molecular Medicine at Scripps Research California
campus, told Technology
Networks, “One of the complaints from funding agencies is that you can
sequence literally thousands of genomes very quickly, but you can’t do the same
in proteomics. There’s a push to try to increase the throughput of proteomics
so that we are more compatible with genomics.”
For that to happen, Yates says manufacturers need to
continue advancing the technology. Much of the research is happening at
universities and in the academic realm. But with commercialization comes
standardization and quality control.
“It’s always exciting when you go to ASMS [the conference for the American Society
for Mass Spectrometry] to see what instruments or technologies are going to be
introduced by manufacturers,” Yates said.
There are signs that commercialization isn’t far off. SomaLogic, a privately-owned American protein
biomarker discovery and clinical diagnostics company located in Boulder, Colo.,
has reached the commercialization stage for a proteomics assay platform called SomaScan. “We’ll be
able to supplant, in some cases, expensive diagnostic modalities simply from a
blood test,” Roy
Smythe, MD, CEO of SomaLogic, told Techonomy.
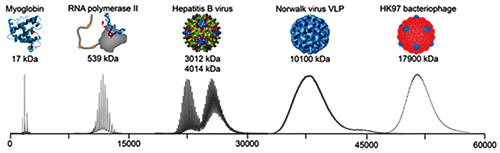
The graphic above illustrates the progression mass spectrometry took during its development, starting with small proteins (left) to supramolecular complexes of intact virus particles (center) and bacteriophages (right). Because of these developments, today’s medical laboratories have more assays that utilize mass spectrometry. (Photo copyright: Technology Networks/Heck laboratory, Utrecht University, the Netherlands.)
Achieving the Necessary Technical Skillset
One of the main reasons mass spectrometry is not more widely
used is that it requires technical skill that not many professionals possess.
“For a long time, MS-based proteomic analyses were technically demanding at
various levels, including sample processing, separation science, MS and the
analysis of the spectra with respect to sequence, abundance and
modification-states of peptides and proteins and false discovery rate
(FDR) considerations,” Ruedi
Aebersold, PhD, Professor of Systems Biology at the Institute of Molecular Systems Biology (IMSB) at
ETH Zurich, told Technology
Networks.
Aebersold goes on to say that he thinks this specific
challenge is nearing resolution. He says that, by removing the problem created
by the need for technical skill, those who study proteomics will be able to
“more strongly focus on creating interesting new biological or clinical
research questions and experimental design.”
Yates agrees. In a paper titled, “Recent Technical Advances in
Proteomics,” published in F1000 Research, a peer-reviewed open research
publishing platform for scientists, scholars, and clinicians, he wrote, “Mass
spectrometry is one of the key technologies of proteomics, and over the last
decade important technical advances in mass spectrometry have driven an
increased capability of proteomic discovery. In addition, new methods to
capture important biological information have been developed to take advantage
of improving proteomic tools.”
No High-Profile Projects to Stimulate Interest
Genomics had the Human Genome Project
(HGP), which sparked public interest and attracted significant funding. One of
the big challenges facing proteomics is that there are no similarly big,
imagination-stimulating projects. The work is important and will result in
advances that will be well-received, however, the field itself is complex and difficult
to explain.
Emanuel
Petricoin, PhD, is a professor and co-director of the Center for Applied
Proteomics and Molecular Medicine at George
Mason University. He told Technology
Networks, “the field itself hasn’t yet identified or grabbed onto a
specific ‘moon-shot’ project. For example, there will be no equivalent to the
human genome project, the proteomics field just doesn’t have that.”
He added, “The equipment needs to be in the background and
what you are doing with it needs to be in the foreground, as is what happened
in the genomics space. If it’s just about the machinery, then proteomics will
always be a ‘poor step-child’ to genomics.”
Democratizing Proteomics
Alexander
Makarov, PhD, is Director of Research in Life Sciences Mass Spectrometry
(MS) at Thermo Fisher
Scientific. He told Technology
Networks that as mass spectrometry grew into the industry we have today,
“each new development required larger and larger research and development teams
to match the increasing complexity of instruments and the skyrocketing
importance of software at all levels, from firmware to application. All this
extends the cycle time of each innovation and also forces [researchers] to
concentrate on solutions that address the most pressing needs of the scientific
community.”
Makarov describes this change as “the increasing democratization of MS,” and says that it “brings with it new requirements for instruments, such as far greater robustness and ease-of-use, which need to be balanced against some aspects of performance.”
One example of the increasing democratization of MS may be
several public proteomic datasets available to scientists. In European
Pharmaceutical Review, Juan
Antonio Viscaíno, PhD, Proteomics Team Leader at the European Bioinformatics Institute (EMBL-EBI)
wrote, “These datasets are increasingly reused for multiple applications, which
contribute to improving our understanding of cell biology through proteomics
data.”
Sparse Data and Difficulty Measuring It
Evangelia
Petsalaki, PhD, Group Leader EMBL-EBI, told Technology
Networks there are two related challenges in handling proteomic data.
First, the data is “very sparse” and second “[researchers] have trouble
measuring low abundance proteins.”
Petsalaki notes, “every time we take a measurement, we
sample different parts of the proteome or phosphoproteome and
we are usually missing low abundance players that are often the most important
ones, such as transcription
factors.” She added that in her group they take steps to mitigate those
problems.
“However, with the advances in MS technologies developed by
many companies and groups around the world … and other emerging technologies
that promise to allow ‘sequencing’ proteomes, analogous to genomes … I expect
that these will not be issues for very long.”
So, what does all this mean for clinical laboratories? At the
current pace of development, its likely assays based on proteomics could become
more common in the near future. And, if throughput and commercialization ever
match that of genomics, mass spectrometry and other proteomics tools could
become a standard technology for pathology laboratories.
If insurance plans are removed from the billing cycle for primary care, it’s not clear how clinical laboratories will be reimbursed for their services
Direct Primary Care (DPC) is gaining popularity in the United States. This emerging movement enables primary care providers to bill patients directly for services rendered, bypassing traditional health plans. On a large scale, employers can contract with primary care practices directly for their employees’ primary care coverage. The idea is to lower healthcare costs. But what exactly is DPC and how are clinical laboratories affected by it?
In operation, direct primary care is similar to concierge medicine, where a patient pays an annual retainer for direct access to a specific healthcare provider. DPC practices offer members unlimited, on-demand visits to primary care physicians for a flat, monthly fee.
The DPC movement has its own lobbying group—the Direct Primary Care Coalition—which supports physicians who opt to practice direct primary care. According to the group’s website, there are currently about 1,000 DPC practices in 48 states which serve over 300,000 patients.
DPC has gained Senatorial support. In December, Senators Bill Cassidy, MD (R-LA), Doug Jones (D-AL), Jerry Moran (R-KS) and Jeanne Shaheen (D-NH) introduced legislation to “lower the cost of healthcare and expand patients’ access to their primary care providers.”
Their bill (H.R. 3708), titled the “Primary Care Enhancement Act of 2019,” would amend the Internal Revenue Code of 1986 to “allow individuals with direct primary care service arrangements to remain eligible individuals for purposes of health savings accounts, and for other purposes.”
A press release announcing the Senate version of the bill (S. 2999), described DPC as a model that “encourages patients to develop personal relationships with their primary care physician, including extending access to care beyond office visits and business hours and through telemedicine. It focuses on prevention and primary care, relying less on specialist and hospital referrals. It is a growing model used by more than 1,000 practices across 48 states and the District of Columbia.”
The press release also states, “DPC models replace copays and deductibles with flat, affordable monthly fees. Current law makes DPC incompatible with health savings accounts (HSAs) paired with high-deductible health plans (HDHPs).”
Direct Primary Care in Practice
Physicians seem to like the DPC model. It frees them, they
say, from the unnecessary interference of insurance providers, the burdens of excessive
paperwork, and ever-increasing administration costs, while allowing them to
have a better patient-doctor relationship.
“I know all my patients by name. I have time for them,” Matthew Abinante, DO, told The DO, a journal of the American Osteopathic Association (AOA). “I probably interact with about 20 patients a day when you factor in the electronic communication.”
Abinante is a board-certified family physician. He practices at Elevated Health, a direct primary care practice in Huntington Beach, CA. Patients pay an average of $75 per month for membership. This fee includes unlimited same day/next day appointments and the ability to talk to a doctor via telephone, e-mail, text, or video chat—24/7.
Matthew Abinante, DO, is shown above treating a patient at Elevated Health, a DPC practice in California. “Our goal is to keep you as healthy as possible, while saving you time and money. We remove the barriers of traditional insurance and provide you with a modern take on the personal, old-fashioned care missing in today’s healthcare industry,” he said. (Photo copyright: Elevated Health.)
At Elevated Health, some minor clinical laboratory tests and
procedures are included in the monthly fee. They include:
Other medical laboratory testing, imaging, and medications
are available to patients at contracted wholesale prices, which are quoted up
front. This is consistent with the trend for price transparency in healthcare.
“What everyone really needs to know is that patients do get better care when their doctor is more satisfied with what they’re doing. And that takes time. What the [fee-for-service] system cannot provide us is time with the patient,” Tiffanny Blythe, DO, told The DO. Blythe runs Blue Lotus Family Medicine, a DPC practice in Kansas City, MO.
When Direct Primary Care Does Not Work
The DPC model has been tried before. In 2010, a DPC provider called Qliance was formed primarily on investment capital from Jeff Bezos of Amazon. The goal was to free doctors and patients from the constraints of traditional health insurance.
Qliance opened several clinics in the Seattle area and by
2014 had nearly 50,000 DPC patients—including employees of Expedia and Comcast. It also had a contract to
provide primary care services with a state Medicaid insurer. Nevertheless, Qliance
closed in 2017.
“We would open up a clinic and add a bunch of docs before we had enough patients to pay for it,” Nick Hanauer, a Seattle venture capitalist and investor in Qliance, told STAT.
“It’s just hard to get the customers because you had to
break the paradigm that was in everyone’s heads about how healthcare had to
work, and you had to disrupt the relationships people had with their insurance
companies,” Hanauer explained.
“Somebody with more economic power than we had could do
this—and should,” he added.
Not All Physicians Support Direct Primary Care
Since the DPC model is so new, there is little research or statistics to confirm it will have a positive effect on healthcare outcomes or lower healthcare costs. Some healthcare professionals have reservations about direct primary care. Their concerns include the potential for less oversight of practitioners and the possibility that patients will slight themselves regarding insurance coverage.
“What we don’t hear about are the people who need more than can cover and what happens to them when they fall into that gap,” Carolyn Engelhard, a health policy analyst and Assistant Professor at the University of Virginia School of Medicine. “We don’t know if they just don’t get care or then enter the traditional healthcare system and start over.”
There are also concerns that DPC plans could draw a large
percentage of healthier patients, which could raise costs for those in
traditional insurance plans, and that it may be more difficult for DPC patients
to gain access to needed specialists and other services.
“Healthcare is fragmented, and if we continue to have little
carve-outs so some [doctors] can practice medicine the way they want, it is not
helping to make the system more responsive and integrated,” Engelhard added.
Nonetheless, both Direct Primary Care and Concierge Medicine
are growing in popularity in the US. And because it’s unclear how clinical
laboratories would interact with or bill DPC practices, clinical laboratory
leaders should keep a close eye on this trend.
As more patients opt for these models of care, healthcare
organizations, pathology groups, and clinical laboratories will have to create
ways to adapt. Since DPC practices are out of most networks, clinical labs may
have to bill patients directly for their services. Not all clinical labs are
prepared to do that, and those that are could experience a slowdown in the
payment process. Labs may also have to contract with physicians to provide
testing services on a pre-determined wholesale cost basis.
These virtual office visits use artificial intelligence and text messaging to allow real physicians to diagnose patients, write prescriptions, and order clinical laboratory tests
Clinical laboratories may soon be receiving test orders from physicians who never see their patients in person, instead evaluating and diagnosing them through a smartphone app. In response to major changes in the primary care industry—mostly driven by consumer demand—mobile app developers are introducing new methods for delivering primary care involving smartphones and artificial intelligence (AI).
Medical laboratories and pathology groups should prepare for consumers who expect their healthcare to be delivered in ways that don’t require a visit to a traditional medical office. One question is how patients using virtual primary care services will provide the specimens required for clinical laboratory tests that their primary care providers want performed?
Two companies on the forefront of such advances are 98point6 and K Health, and they provide a glimpse of primary care’s future. The two companies have developed smartphone apps that incorporate AI and the ability to interact with real physicians via text messaging.
Virtual Primary Care 24/7 Nationwide
Dark Daily has repeatedly reported that primary care in America is undergoing major changes driven by many factors including increasingly busy schedules, the popularity of rapid retail and urgent care clinics, consumer use of smartphones and the Internet to self-diagnose, and decreasing numbers of new doctors choosing primary care as a career path.
Writing in Stat, two physicians who had just completed internal medicine residencies, explained their own decisions to leave primary care. In their article, titled, “We were inspired to become primary care physicians. Now we’re reconsidering a field in crisis,” Richard Joseph, MD, and Sohan Japa, MD, cited factors that include long hours, low compensation in comparison with specialty care, and deficiencies in primary care training. At the time of their writing they were senior residents in primary care-internal medicine at Brigham and Women’s Hospital in Boston.
They also pointed to a decline in office visits to primary care doctors. “Patients are increasingly choosing urgent care centers, smartphone apps, telemedicine, and workplace and retail clinics that are often staffed by nurse practitioners and physician assistants for their immediate health needs,” they wrote.
One solution to declining populations of primary care physicians is a smartphone app created by Seattle-based 98point6. The service involves “providing virtual text-based primary care across the entire country, 24/7 of everyday,” explained Brad Younggren, MD, an emergency physician and Chief Medical Officer at 98point6, in a YouTube interview. “It’s text-based delivery of care overlaid with an AI platform on top of it.”
The service launched on May 1, 2018, in 10 states and is now available nationwide, according to press releases. 98point6 offers the service through individual subscriptions or through deals with employers, health plans, health systems, and other provider organizations. The personal plan costs $20 for the first year and $120 for the second, plus $1 per “visit.”
Subscribers use text messaging to interact with
an “automated assistant” that incorporates artificial intelligence. While
messaging, they can describe symptoms or ask questions about medical topics.
“After the automated assistant has gathered as many
questions as it deems necessary, it hands [the information] off to a
physician,” Younggren said. In most cases, all communication is via text
messaging. However, the doctor may ask the subscriber to send a photo or participate
in a video meeting.
The doctor then makes a diagnosis and treatment plan. Prescriptions can be sent to a local pharmacy and the subscriber can be referred to a clinical laboratory for tests. LabCorp or Quest Diagnostics are preferred providers, but subscribers can choose to have orders sent to independent labs as well, states the company’s website.
Younggren claims the company’s physicians can resolve more
than 90% of the cases they encounter. If, however, they can’t resolve a case, they
can refer the patient to a local physician. And because most of 98point6’s
interactions with subscribers are text-based, that messaging serves as reference
documentation for other doctors, he said.
“We’ve set out to dramatically augment the primary-care physician with deep technology by delivering an on-demand primary-care experience,” Robbie Cape (above), CEO and co-founder of 98point6, told Modern Healthcare. (Photo copyright: Seattle Business Magazine.)
The 98point6 physicians are full-time employees and work with the company’s technologists to improve the AI’s capabilities, Younggren said. The company claims its doctors can diagnose and treat more than 400 conditions, including: allergies, asthma, skin problems, coughs, flu, diabetes, high blood pressure, and infections. For medical emergencies, subscribers are advised to seek emergency help locally.
98point6 also can function as a front end for interacting
with patients in health systems that have their own primary-care doctors,
Younggren said. The company’s health system clients “don’t actually have a good
digital primary care front end to deliver care,” he said. “So, we can
essentially give them that, and then we can also get some detailed
understanding of how to coordinate care within the health system to drive
patients to the care that they need.” For example, this can include directing the
patient to an appropriate sub-specialist.
Leveraging Patient Data to Answer Health Questions
K Health in New York City offers a similar service based on its own AI-enabled smartphone app. The app incorporates data gleaned from the records of more than two million anonymous patients in Israel over the past 20 years, explained company co-founder Ran Shaul, co-founder and Chief Product Officer, in a blog post.
The software asks users about their “chief complaint” and
then compares the answers with data from similar cases. “We call this group
your ‘People Like Me’ cohort,” Shaul wrote. “It shows you how doctors diagnosed
those people and all the ways they were treated.”
The K Health app is free, but for a fee ranging from $14 for a one-time visit to $39 for an annual subscription, users can text with doctors, the company’s website states.
Unlike 98point6, K Health’s doctors are employed by “affiliated physician-owned professional corporations,” the company says, not K Health itself.
“The doctor you chat with will discuss a recommended treatment plan that may include a physical exam, lab tests, or radiology scans,” states K Health’s website. “They may send you directly for some of these tests, but others will require you to visit a local doctor.”
These are just the latest examples of new technologies and
services devised to help patients receive primary care. How a patient who uses
a smartphone app gets the necessary clinical laboratory tests performed is a
question yet to be answered.
Clinical laboratory leaders will want to watch this shift in
the delivery of primary care and look for opportunities to serve consumers who
are getting primary care from nontraditional sources.