Changes in reimbursement models and federal compliance, as well as tougher payer audits, make it critical clinical laboratory managers are fully informed and prepared for what lies ahead in 2020
Not only does January 1st bring the new year of 2020, but it
also brings tough challenges for leaders of the nation’s clinical
laboratories and anatomic
pathology groups. Most of these challenges are triggered by the ongoing
transformation of the American healthcare system.
“Healthcare’s transformation in this country has two primary
elements,” said Robert L.
Michel, Editor-in-Chief of The Dark
Report, sister publication of Dark Daily. “One is the
integration of medical care to meet the related goals of keeping people out of
hospitals—the most expensive site of care—and to proactively manage patients to
keep them healthy.
“The second is reimbursement reform,” he continued.
“Healthcare policymakers want to eliminate fee-for-service
payments and move providers to different forms of value-based
reimbursement. The federal Medicare program seems to be taking the lead
over private payers as it introduces different pilot programs that reimburse
physicians and hospitals through such methods as bundled
payments, shared-savings arrangements, and per-member per-month (PMPM)
arrangements.”
Michel predicts that both the integration of care delivery
and the shift away from fee-for-service payment will become more urgent
challenges for clinical laboratory managers and pathologists during 2020.
“Take the integration of care, for example. Clinical laboratories,
since their inception, have been organized to serve the different provider
silos,” Michel stated. “Each client—whether it was a primary care physician, a
specialist doctor, a hospital, or a nursing home—could be served as a
stand-alone customer. That client ordered tests and the lab performed those
tests, submitted the results to that client, then billed insurance as
appropriate.
“Integration of clinical care changes that laboratory
service model in significant ways,” he continued. “Now, when a provider within
an integrated health system orders a medical laboratory test, the lab will want
those lab test results to be available, via the electronic
health record (EHR) system, to other providers within that health system.
“That is one example of how integrated care requires
clinical labs to realign their service model,” Michel added. “Combine that need
to change with the steady transition away from fee-for-service to reimbursement
based on value and you can see why all labs in the United States will be
uniquely challenged, not just in 2020, but in the succeeding years.”
Robert Michel (above) is Editor-in-Chief of The Dark Report and Dark Daily and founder of The Dark Intelligence Group. He will be hosting the 25th anniversary Executive War College on Lab and Pathology Management, which takes place April 28-29, 2020, in New Orleans. (Photo copyright: The Dark Report.)
Even Minor Changes in Care Require Major Responses by
Medical Laboratories
It is important for clinical laboratory managers, pathology
practice administrators, and the pathologists who are the business leaders of
their groups to understand the width and depth of the changes happening in
healthcare and laboratory medicine in the United States today. Even little
changes in how care is delivered can require a major response in how medical
laboratories are organized and how they deliver lab testing services.
For example, here are distinct trends associated with how
providers are responding to healthcare’s current transformation:
Meanwhile, the clinical laboratory industry is undergoing
its own transformation. Three major trends illustrate how labs are responding
to the new healthcare marketplace realities:
More use of Lean,
Six Sigma,
and process improvement techniques as labs strive to cut costs while protecting
quality and maintaining top-flight service levels.
More collaboration with providers, payers, and
even consumers, as innovative medical laboratory organizations move to deliver
more value, consistent with the Clinical Lab
2.0 business model.
Acquiring more robust information technologies
and analytics tools needed to leverage the lab’s clinical test data in ways to
provide increased value, not just to hospitals and physicians, but to payers,
patients, and a new class of care management companies that want to use big data and machine learning to
help payers and providers improve patient outcomes.
All of these trends will not only be high profile during
2020, but they will be driving forces throughout the decade of the 2020s.
This is why The Dark Report’s 25th anniversary Executive War College on Lab and
Pathology Management, which takes place April 28-29, 2020, in New Orleans,
will feature essential sessions and expert speakers who have the answers you need
to guide your lab through the challenging times yet to come.
Narrowing networks that exclude your lab from access to
patients? Executive War College has health plan lab network managers to share
insights with you, along with experienced lab managed care contracting
executives who can challenge these payers and teach you the secrets of winning
and keeping status as an in-network laboratory.
Concerned about new compliance issues—such as EKRA
(Eliminating Kickback in Recovery Act of 2018) and Medicare’s recent affiliation
disclosure rule for tougher government and private payer audits—that
challenge your lab’s financial integrity? Executive War College is bringing
together the nation’s smartest minds in compliance, billing/collections, and
lab accreditation to give you first-hand updates on the must-dos and the
must-avoids, so your lab is always inspection ready and compliant.
Because this is the 25th anniversary of the Executive War
College, we are pulling out all the stops to put on the biggest and best
conference on lab and pathology management that the nation has seen. There will
be more than 125 speakers and 90 sessions, along with our always-popular
two-roundtables for Lab CFOs, Academic Pathology, Lab CIOs, and Lab
Quality/Compliance Managers.
Most importantly for you, this year’s Executive War College
may be the most important lab management meeting you attend in 2020, because
there is no other place that puts you face-to-face with experts in every aspect
of clinical laboratories and anatomic pathology group management, while—at the
same time—giving you unparalleled networking with the lab profession’s
innovators.
This is the best investment you can make in both your professional management career and the successful operation of your laboratory.
Register today at https://dark.regfox.com/executive-war-college-2020 to reserve your seat and save $200 off regular registration rates, but act now while it’s fresh on your mind as these super-early-bird savings end January 31.
By offering DTC preventative gene sequencing, hospital leaders
hope to help physicians better predict cancer risk and provide more accurate
diagnoses
Two Boston health systems, Brigham and Women’s Hospital and Massachusetts General Hospital (MGH), are the latest to open preventative gene sequencing clinics and compete with consumer gene sequencing companies, such as 23andMe and Ancestry, as well as with other hospital systems that already provide similar services.
This may provide opportunities for clinical laboratories. However, some experts are concerned that genetic sequencing may not be equally available to patients of all socioeconomic classes. Nor is it clear how health systems plan to pay for the equipment and services, since health insurance companies continue to deny coverage for “elective” gene sequencing, or when there is not a “clear medical reason for it, such as for people with a long family history of cancer,” notes STAT.
Therefore, not everyone is convinced of the value of gene sequencing to either patients or hospitals, even though advocates tout gene sequencing as a key element of precision medicine.
Is Preventative Genetic Sequencing Ready for the Masses?
Brigham’s Preventive Genomics Clinic offers comprehensive DNA sequencing, interpretation, and risk reporting to both adults and children. And MGH “plans to launch its own clinic for adults that will offer elective sequencing at a similar price range as the Brigham,” STAT reported.
The Brigham and MGH already offer similar gene sequencing services as other large health systems, such as Mayo Clinic and University of California San Francisco (UCSF), which are primarily used for research and cancer diagnoses and range in price depending on the depth of the scan, interpretation of the results, and storage options.
However, some experts question whether offering the
technology to consumers for preventative purposes will benefit anyone other
than a small percentage of patients.
“It’s clearly not been demonstrated to be cost-effective to promote this on a societal basis,” Robert Green, MD, MPH, medical geneticist at Brigham and Women’s Hospital, and professor of genetics at Harvard, told STAT. “The question that’s hard to answer is whether there are long-term benefits that justify those healthcare costs—whether the sequencing itself, the physician visit, and any downstream testing that’s stimulated will be justified by the situations where you can find and prevent disease.”
Additionally, large medical centers typically charge more
for genomic scans than consumer companies such as 23andMe and Ancestry. Hospital-based
sequencing may be out of the reach of many consumers, and this concerns some
experts.
“The idea that genomic sequencing is only going to be
accessible by wealthy, well-educated patrons who can pay out of pocket is
anathema to the goals of the publicly funded Human Genome Project,” Jonathan
Berg, MD, PhD, Genetics Professor, University of North Carolina at Chapel
Hill, told Scientific
American.
And, according to the American Journal of Managed Care, “It’s estimated that by 2021, 100 million people will have used a direct-to-consumer (DTC) genetic test. As these tests continue to gain popularity, there is a need for educating consumers on their DTC testing results and validating these results with confirmatory testing in a medical-grade laboratory.”
This is why it’s critical that clinical laboratories and
anatomic pathology groups have a genetic testing and gene sequencing strategy,
as Dark
Daily reported.
David Bick, MD, Chief Medical Officer at the HudsonAlpha Institute for Biotechnology and Medical Director of the Smith Family Clinic for Genomic Medicine, told Scientific American, “there’s just more and more interest from patients and families not only because of 23andMe and the like, but because there’s just this understanding that if you can find out information about your health before you become sick, then really our opportunity as physicians to do something to help you is much greater.”
In an article he penned for Medium, Robert Green, MD, MPH (shown above counseling a patient), medical geneticist at Brigham and Women’s Hospital and professor of genetics at Harvard, wrote, “The ultimate aim of our Genomes2People Research Program is to contribute to the transformation of medicine from reactive to proactive, from treatment-oriented to preventive. We are trying to help build the evidence base that will justify societal decision to make these technologies and services accessible to anyone who wants them, regardless of means, education or race and ethnicity.” (Photo copyright: Wall Street Journal.)
Is Preventative Genomics Elitist?
As large medical centers penetrate the consumer genetic
testing market some experts express concerns. In a paper he wrote for Medium,
titled, “Is Preventive Genomics Elitist?” Green asked, “Is a service like this
further widening the inequities in our healthcare system?”
Green reported that while building the Preventive Genomics Clinic at Brigham, “we … struggled with the reality that there is no health insurance coverage for preventive genomic testing, and our patients must therefore pay out of pocket. This is a troubling feature for a clinic at Brigham and Women’s Hospital, which is known for its ties to communities in Boston with diverse ethnic and socioeconomic backgrounds.”
Most of Brigham’s early genetics patients would likely be “well-off,
well-educated, and largely white,” Green wrote. “This represents the profile of
typical early adopters in genetic medicine, and in technology writ large. It
does not, however, represent the Clinic’s ultimate target audience.”
More Data for Clinical Laboratories
Nevertheless, preventive genomics programs offered by large
health systems will likely grow as primary care doctors and others see evidence
of value.
Therefore, medical laboratories that process genetic
sequencing data may soon be working with growing data sets as more people reach
out to healthcare systems for comprehensive DNA sequencing and reporting.
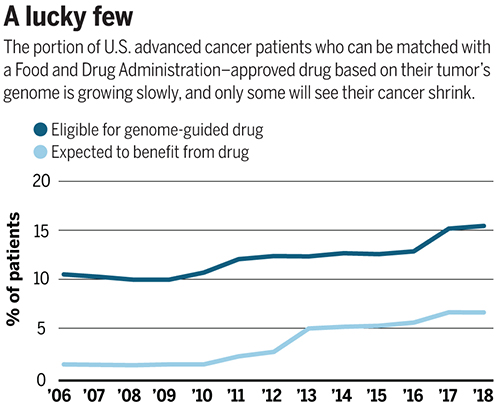
Number of patients eligible for genome-driven oncology therapy is increasing, but the percentage who reportedly benefit from the therapy remains at less than 5%
Advances in precision medicine in oncology (precision oncology) are fueling the need for clinical laboratory companion diagnostic tests that help physicians choose the best treatment protocols. In fact, this is a fast-growing area of clinical diagnostics for the nation’s anatomic pathologists. However, some experts in the field of genome-based cancer treatments disagree over whether such treatments offer more hype than hope.
Prasad and his colleagues evaluated 31 US Food and Drug
Administration (FDA) approved drugs, which were “genome-targeted” or
“genome-informed” for 38 indications between 2006 and 2018. The researchers
sought to answer the question, “How many US patients with cancer are eligible
for and benefit annually from genome-targeted therapies approved by the US Food
and Drug Administration?”
They found that in 2018 only 8.33% of 609,640 patients with
metastatic cancer were eligible for genome-targeted therapy—though this was an
increase from 5.09% in 2006.
Even more telling from Prasad’s view, his research team concluded
that only 4.9% had benefited from such treatments. Prasad’s study found the
percentage of patients estimated to have benefited from genome-informed therapy
rose from 1.3% in 2006 to 6.62% in 2018.
“Although the number of patients eligible for genome-driven treatment has increased over time, these drugs have helped a minority of patients with advanced cancer,” the researchers concluded. “To accelerate progress in precision oncology, novel trial designs of genomic therapies should be developed, and broad portfolios of drug development, including immunotherapeutic and cytotoxic approaches, should be pursued.”
The graph above is based on data from a study published in Science titled, “Estimation of the Percentage of US Patients With Cancer Who Benefit from Genome-Driven Oncology,” co-authored by Vinay Prasad, MD, MPH, et al. (Image copyright: Science.)
A Value versus Volume Argument?
Hyman, who leads a team of oncologists that conduct dozens
of clinical trials and molecularly selected “basket studies” each year,
countered Prasad’s assertions by noting the increase in the number of patients
who qualify for precision oncology treatments.
As reported in Science, Hyman said during his AACR
presentation that Sloan Kettering matched 15% of the 25,000 patients’ tumors it
tested with FDA-approved drugs and 10% with drugs in clinical trials.
“I think this is certainly not hype,” he said during the
conference.
Hyman added that another 10% to 15% of patient tumors have a
DNA change that matches a potential drug tested in animals. He expects “basket”
trials to further increase the patient pool by identifying drugs that can work
for multiple tumor types.
The US National Institute of Health (NIH) describes “basket studies” as “a new sort of clinical studies to identify patients with the same kind of mutations and treat them with the same drug, irrespective of their specific cancer type. In basket studies, depending on the mutation types, patients are classified into ‘baskets.’ Targeted therapies that block that mutation are then identified and assigned to baskets where patients are treated accordingly.”
Are Expectations of Precision Medicine Exaggerated?
A profile in MIT Technology Review, titled, “The Skeptic: What Precision Medicine Revolution?,” describes Prasad’s reputation as a “professional scold” noting the 36-year-old professor’s “sharp critiques of contemporary biomedical research, including personalized medicine.” Nevertheless, Prasad is not alone in arguing that precision oncology’s promise is often exaggerated.
“Like most ‘moonshot’ medical research initiatives,
precision medicine is likely to fall short of expectations,” Joyner wrote.
“Medical problems and their underlying biology are not linear engineering
exercises and solving them is more than a matter of vision, money, and will.”
“Although some niche applications have been found for
precision medicine—and gene therapy is now becoming a reality for a few rare
diseases—the effects on public health are miniscule while the costs are astronomical,”
they wrote.
Hope for Precision Medicine Remains High
However, optimism over precision oncology among some industry leaders has not waned. Cindy Perettie, CEO of molecular information company Foundation Medicine of Cambridge, Mass., argues genome-directed treatments have reached an “inflection point.”
“Personalized cancer treatment is a possibility for more patients than ever thanks to the advent of targeted therapies,” she told Genetic Engineering and Biotechnology News. “With a growing number of new treatments—including two pan-tumor approvals—the need for broad molecular diagnostic tools to match patients with these therapies has never been greater. We continue to advance our understanding of cancer as a disease of the genome—one in which treatment decisions can be informed by insight into the genomic changes that contribute to each patient’s unique cancer.”
Prasad acknowledges genome-driven therapies are beneficial for some cancers. However, he told MIT Technology Review the data doesn’t support the “rhetoric that we’re reaching exponential growth, or that is taking off, or there’s an inflection point” signaling rapid new advancements.
“Right now, we are investing heavily in immunotherapy and heavily in genomic therapy, but in other categories of drugs, such as cytotoxic drugs, we have stopped investigating in them,” he told Medscape Medical News. “But it’s foolish to do this—we need to have the vision to look beyond the fads we live by in cancer medicine and do things in a broader way,” he added.
“So, I support broader funding because you have to sustain
efforts even when things are not in vogue if you want to make progress,” Prasad
concluded.
Is precision oncology a fad? Dark Daily has covered the advancements in precision medicine extensively over the past decade, and with the launch of our new Precision Medicine Institute website, we plan to continue reporting on further advancements in personalized medicine.
Time will tell if precision oncology can fulfill its
promise. If it does, anatomic pathologists will play an important role in
pinpointing patients most likely to benefit from genome-driven treatments.
One thing that the debate between proponents of precision
medicine in oncology and their critics makes clear is that more and better
clinical studies are needed to document the true effectiveness of target
therapies for oncology patients. Such evidence will only reinforce the
essential role that anatomic pathologists play in diagnosis, guiding
therapeutic decisions, and monitoring the progress of cancer patients.
Combining consumers’ health data, including clinical laboratory test results, to genetic data for predispositions to chronic diseases could be key to developing targeted drugs and precision medicine treatments
Genetic testing company 23andMe is beta testing a method for combining customers’ private health data—including clinical laboratory test results and prescription drug usage—with their genetic data to create the largest database of its kind.
Such information—stored securely but accessible to 23andMe for sale to pharmaceutical companies for drug research and to diagnostics developers—would place 23andMe in a market position even Apple Health cannot claim.
Additionally, given the importance of clinical lab test data—which makes up more than 70% of a patient’s medical records—it’s reasonable to assume that innovative medical laboratories might consider 23andMe’s move a competitive threat to their own efforts to capitalize on combining lab test results with patients’ medical histories, drug profiles, and demographic data.
23andMe plans to use third-party medical network Human API to collect and manage the data. Involvement in the beta test is voluntary and currently only some of the genetic company’s customers are being invited to participate, CNBC reported.
Apple Healthcare, 23andMe, and Predicting Disease
The announcement did not go unnoticed by Apple, which has its own stake in the health data market. Apple Healthcare’s product line includes:
Mobile device apps for using at point-of-care in hospitals;
iPhone apps that let customers store and share their medical and pharmaceutical histories and be in contact with providers;
ResearchKit, which lets researchers build specialized apps for their medical research;
CareKit, which lets developers build specialized monitoring apps for patients with chronic conditions; and
Apple Watch, which doubles as a medical device for heart monitoring.
What Apple does not have is genetic data, which is an issue.
An Apple Insider post notes, “As structured, 23andMe’s system has advantages over Apple’s system including not just genetic data, but insights into risks for chronic disease.”
This is significant. The ability to predict a person’s predisposition to specific chronic diseases, such as cancer, is at the heart of Precision Medicine. Should this capability become not only viable and reliable but affordable as well, 23andMe could have a sizeable advantage in that aspect of the health data market.
Anne Wojcicki (above) is CEO and co-founder of 23andMe. The genetic company is inviting some of its customers to combine their medical information—including clinical laboratory test results and medication histories—with their stored genetic data. Customers would have access to the combined data and be able to share it with providers. In exchange, 23andMe gets to sell it to pharmaceutical companies and diagnostics developers. If successful and popular with the eight to 10-million peoplewho have reportedly purchased its test kits, 23andMe could produce a significant source of revenue. (Photo copyright: Inc.)
Genetic Test Results Combined with Clinical Laboratory
Test Results
23andMe is hopeful that after people receive their genetic test
results, they will then elect to add their clinical laboratory results, medical
histories, and prescription drug information to their accounts as well. 23andMe
claims its goal is to provide customers with easy, integrated access to health
data that is typically scattered across multiple systems, and to assist with
medical research.
“It’s a clever move,” Ruby Gadelrab, former Vice President of Commercial Marketing at 23andMe who now provides consulting services to health tech companies, told CNBC. “For consumers, health data is fragmented, and this is a step towards helping them aggregate more of it.”
CNBC also reported that Gadelrab said such a database
“might help 23andMe provide people with information about their risks for complex,
chronic ailments like diabetes, where it’s helpful for scientists to access a
data-set that incorporates information about individual health habits,
medications, family history and more.”
Of course, it bears saying that the revenue generated from cornering
the market on combined medical, pharmaceutical, and genetic data from upwards
of 10-million customers would be a sizable boon to the genetic test company.
CNBC reported that “the company confirmed that it’s a
beta program that will be gradually rolled out to all users but declined to
comment further on its plans. The service is still being piloted, said a person
familiar with the matter, and the product could change depending on how it’s
received.”
Will 23andMe Have to Take on Apple?
23andMe already earns a large portion of its revenue through
research collaborations with pharmaceutical companies, and it hopes to leverage
those collaborations to produce new drug therapies, CNBC reported.
This new venture, however, brings 23andMe into competition
with Apple on providing a centralized location from where consumers can access
and share their health data. But it also adds something that Apple does not
have—genetic data that can provide insight into consumers’ predispositions to
certain diseases, which also can aid in the development of precision medicine
treatments for those diseases.
Whether Apple Healthcare perceives 23andMe’s encroachment on
the health data market as a threat remains to be seen.
Nevertheless, this is another example of a prominent company
attempting to capitalize on marketable customer information. Adding medical information
to its collected genetic data could position 23andMe to generate significant
revenue by selling the merged data to pharmaceutical companies and diagnostics
developers, while also helping patients easily access and share their data with
healthcare providers.
It’s a smart move, and those clinical laboratory executives
developing ways to produce revenue from their lab organization’s patient lab test
data will want to watch closely as 23andMe navigates this new market.
In response to Harvard’s conclusions, the Joint Commission claimed the study contained “factual errors” and “multiple methodological flaws” in strong rebuttals to findings
Today’s emphasis on value-based healthcare rewards hospitals, physicians, clinical laboratories, and other healthcare service providers for improved patient outcomes. But does hospital accreditation play a role in those improved outcomes? A study published in the British Medical Journal (BMJ) suggests that hospital accreditation may not directly correlate to improved patient care and that one accrediting organization may be just as good as another.
Researchers at Harvard T.H. Chan School of Public Health (Harvard) conducted the study. They looked at healthcare outcomes from 4,400 US hospitals between 2014 and 2017, of which 3,337 were accredited (2,847 by The Joint Commission) and 1,063 received state-based reviews.
The researchers’ objective was “To determine whether
patients admitted to US hospitals that are accredited have better outcomes than
those admitted to hospitals reviewed through state surveys, and whether
accreditation by The Joint Commission (the largest and most well-known
accrediting body with an international presence) confers any additional
benefits for patients compared with other independent accrediting
organizations.”
In their published results, the Harvard researchers concluded:
“Patients treated at accredited hospitals had
lower 30-day mortality rates (although not statistically significant lower
rates, based on the prespecified P value threshold) than those at hospitals
that were reviewed by a state survey agency … but nearly identical rates of
mortality for the six surgical conditions;
“Readmissions for the 15 medical conditions at
30 days were significantly lower at accredited hospitals than at state survey …
but did not differ for the surgical conditions;
No statistically significant differences were
seen in 30-day mortality or readmission rates (for both the medical or surgical
conditions) between hospitals accredited by The Joint Commission and those
accredited by other independent organizations.”
Why is this finding important? As the largest independent
accrediting organization, The Joint Commission holds enormous influence over
doctors and other healthcare service providers. The Joint Commission accredits more
than 21,000 US healthcare providers, as well as hospitals throughout the world.
Most states require Joint Commission accreditation for hospitals to receive
Medicare/Medicaid reimbursements.
However, Harvard’s study found hospitals accredited by the
Joint Commission had no better patient outcomes than hospitals reviewed by
state survey agencies. The conclusions published by this research team casts
doubt on the perceived higher value of the Joint Commission’s accreditation
over other accrediting bodies, and on the value of accreditation itself.
“There was no evidence in this study to indicate that
patients choosing a hospital accredited by the Joint Commission confer any
healthcare benefits over choosing a hospital accredited by another independent
accrediting organization,” the researchers concluded in their paper.
Ashish Jha, MD, MPH (above) K. T. Li Professor of Global Health and Health Policy at the Harvard T. H. Chan School of Public, co-authored the Harvard study. He maintains that for accreditation to ensure hospital quality, accreditation standards must be refocused. “First, there must be a clear delineation of high-quality care (good outcomes, good experience) and that must be the guiding principle behind accreditation,” he wrote in JAMA Forum. “Hospitals should be held accountable for those outcomes. Accrediting bodies should focus on those processes and structural factors that have been convincingly shown to be associated with good outcomes.” (Photo copyright: Harvard.)
Not So Fast!
The Joint Commission is an independent, not-for-profit organization
that has accredited hospitals for nearly 70 years. Approximately 81% of
hospitals accredited in the US are accredited by the Joint Commission. So, of
course, the Joint Commission took issue with the Harvard researchers’ findings.
In a formal statement and a response published in BMJ, the Joint Commission cited “factual errors” and “multiple methodological flaws that make the [study] results invalid.”
Nonetheless, the Joint Commission also pointed out that
Joint Commission-accredited hospitals were found by the researchers to demonstrate
lower mortality than state-surveyed hospitals and lower readmission rates for
the medical conditions cited.
“While study authors considered the differences ‘modest,’
applying them to the more than three million patients with medical conditions
addressed in this study indicates that patients treated in Joint
Commission-accredited hospitals experienced 12,000 fewer deaths and 24,000
fewer readmissions,” the formal statement said. “We believe that makes a
difference to patients as much as it does to us.”
Joint Commission Partners with Leapfrog Group
Scrutiny of hospital accrediting bodies is not new. A 2002 article by The Dark Report, Dark Daily’s sister publication, reported on the Joint Commission’s decision to become a “formal partner” in the Leapfrog Group, a non-profit organization founded in 2000 that advocates for improved hospital safety and quality. (See TDR, “Provider Performance Ranking Now Hitting Healthcare System,” January 28, 2002.)
The Joint Commission announced the partnership one day before the Leapfrog Group’s release of data in the journal Quality Management in Healthcare showing “that a hospital’s accreditation status did not correlate to better quality and safety of patient care. The study specifically noted that hospitals with higher-than-average rates of deaths and complications often received favorable scores from the [Joint Commission],” TDR reported.
However, as Robert Michel, TDR’s Editor-in-Chief and Publisher, noted in the article, “The [Joint Commission’s] willingness to partner with the Leapfrog Group is a significant event. The timing of the [Joint Commission’s] announcement, one day before Leapfrog made its hospital data available to the public, demonstrates that it will become more responsive to the quality concerns of employers.
“For laboratory executives and pathologists,” Michel
continued, “this is a signal event in determining how the healthcare system
will evolve in the next few years. I believe it is the first of what will become
a major effort to identify, measure, and report on the quality performance of
all categories of healthcare providers.”
Michel made his comments in 2002. Today, hospital and
individual health provider reimbursements are increasingly based on those very
performance and quality-of-outcome reports.
Healthcare systems now publish data on healthcare providers so
patients can make informed decisions. It is consistent with the trend to rank
providers by patient outcomes and similar metrics, which TDR predicted
nearly two decades ago.
Moreover, the growing availability of the outcomes data from
hospitals, physicians, and other types of providers is a signal to both
clinical laboratories and individual pathologists that public scorecards on the
quality, outcomes, and costs of their labs or their professional pathology
services are coming.
However, since major change in the healthcare system takes
years to achieve, public scorecards for labs and pathologists are probably
still years away as well.
Through partnerships with CVS, Utah Health, and Kaiser Permanente the new UPSFF drone service could deliver savings to healthcare consumers and reduced TATs for clinical laboratories
United Parcel Service (UPS) successfully delivered by air medical prescriptions from a CVS pharmacy to customers’ residences in Cary N.C. This was the next step in the package delivery company’s plan to become a major player in the use of drones in healthcare and it has major implications for clinical laboratories and pathology groups.
Earlier this year, Dark Daily’s sister publication, The Dark Report (TDR), covered UPS’ launch of a drone delivery service on the WakeMed Health and Hospitals medical campus in Raleigh, N.C. The implementation followed a two-year test period during which UPS used drones manufactured by Matternet, a company in Menlo Park, Calif., to fly clinical laboratory specimens from a medical complex of physicians’ offices to the health system’s clinical laboratory more than 100 times. (See TDR, “WakeMed Uses Drone to Deliver Patient Specimens,” April 8, 2019.)
At the 24th Annual Executive War College on Lab and Pathology Management in April, Chairman and CEO David Abney (above) explained why UPS is investing in drone technology for clinical laboratory health network delivery. “Healthcare is a strategic imperative for us,” Abney said. “We deliver a lot of important things, but lab [shipments] are critical, and they’re very much a part of patient care.” (Photo copyright: Dark Daily.)
In October, UPS signed a letter of intent with CVS Health to “explore drone deliveries, expanding UPS’ sights from hospital campuses to the homes of CVS customers as it builds out its drone delivery subsidiary,” Modern Healthcare reported.
In November, UPS succeeded in these goals with UPS Flight Forward, Inc. (UPSFF), UPS’ new drone delivery service which, according to its website, is the first “drone airline” to receive full Part 135 certification (Package Delivery by Drone) from the Federal Aviation Administration (FAA).
“This drone delivery, the first of its kind in the industry, demonstrates what’s possible for our customers who can’t easily make it into our stores,” said Kevin Hourican, EVP, CVS Health and President of CVS Pharmacy, in a UPS press release. “CVS is exploring many types of delivery options for urban, suburban, and rural markets. We see big potential in drone delivery in rural communities where life-saving medications are needed and consumers at times cannot conveniently access one of our stores.”
Drones Deliver Clinical Lab Specimens and Pharmaceuticals
Since March, UPSFF has completed more than 1,500 drone
flights (with 8,000 clinical laboratory samples) at WakeMed in Raleigh, N.C.
UPS’ drone delivery decreased delivery time of clinical laboratory specimens
between WakeMed’s physician office building to the hospital-based lab from 19
minutes to three minutes, according to UPS data reported in October by an Advisory
Board daily briefing.
WakeMed is seeking to “provide advantages in patient care
that cannot be obtained in any other way” Michael
Weinstein, MD, PhD, Director of Pathology Laboratories at WakeMed, told TDR.
With the signing of the UPS (NYSE:UPS)-UPSFF (UPS Flight
Forward)-CVS (NYSE:CVS.N) agreement in October—and initial first flights which
took place on November 1 between a CVS pharmacy and customers’ residences in
Cary, NC—UPS completed the “the first revenue-generating drone delivery of a
medical prescription from a CVS pharmacy directly to a consumer’s home,” the
UPS press release states.
“When we launched UPS Flight Forward, we said we would move quickly to scale this business … and that’s exactly what we are doing,” Scott Price (above), UPS Chief Strategy and Transformation Officer, told Supply Chain Dive. “We started with a hospital campus environment and are now expanding scale and use-cases,” he added. Clinical laboratories can probably look forward to similar UPS drone delivery services in all 50 states and Washington, DC. (Photo copyright: UPS.)
Other Healthcare Organizations on Board
WakeMed and CVS are not alone in UPS drone deployment for
healthcare deliveries. Advisory Board reported that UPSFF also partnered
with other healthcare systems to provide drone flights for on-campus delivery of
pharmaceuticals and medical supplies, including:
AmerisourceBergen:
to move pharmaceuticals, supplies, and records to “qualifying” medical
campuses;
Kaiser
Permanente: to send medical supplies between buildings at different campus
sites; and
University
of Utah Health’s hospital campuses: to transport biological samples,
documents, supplies, and medical instruments between their facilities.
Drone delivery of clinical laboratory specimens is swiftly become a global reality that labs should watch closely. Past Dark Daily e-briefings reported on drone deliveries being conducted in Virginia, North Carolina, Australia, Switzerland, and Rwanda.
Pathologists and medical laboratory managers need to stay
abreast of these developments, as widespread drone delivery of clinical laboratory
specimens may happen on a surprisingly fast timeline. Drone delivery already
has TAT improvement implications and could be a way for labs to differentiate
their businesses and enhance workflow.