This is important for clinical laboratory leaders to watch, because medical labs often interface with hospital EHRs to exchange vital patient data, a key component of complying with Medicare’s EHR incentive programs. If claims of interoperability are shown to be false, could labs engaged with those hospital systems under scrutiny be drawn into the DOJ’s investigations?
Violating the False Claims Act
In May, Coffey Health System (CHS), which includes Coffey County Hospital, a 25-bed critical access hospital located in Burlington, Kan., agreed to pay the US government a total of $250,000 to settle a claim that it violated the False Claims Act.
CHS’ former CIO filed the qui tam (aka, whistleblower) lawsuit, which allows individuals to sue on behalf of the government and share in monetary recovery. He alleged that CHS provided false information to the government about being in compliance with security standards to receive incentive payments under the EHR Incentive Program.
According to a DOJ press release, “the United States alleged that Coffey Health System falsely attested that it conducted and/or reviewed security risk analyses in accordance with requirements under a federal incentive program for the reporting periods of 2012 and 2013. The government contended that the hospital submitted false claims to the Medicare and Medicaid Programs pursuant the Electronic Health Records (EHR) Incentive Program.”
“Medicare and Medicaid beneficiaries expect that providers ensure the accuracy and security of their electronic health records,” said Stephen McAllister (above), United States Attorney for the District of Kansas, in the DOJ press release. “This office remains committed to protecting the federal health programs and to hold accountable those whose conduct results in improper payments.” (Photo copyright: US Department of Justice.)
The Recovery Act allocated $25 billion to incentivize healthcare professionals and facilities to adopt and demonstrate meaningful use (MU) of electronic health records by January 1, 2014. The federal Centers for Medicare and Medicaid Services (CMS) released the incentive funds when providers attested to accomplishing specific goals set by the program.
The website of the Office of the National Coordinator for Health Information Technology (ONC), HealthIt.gov, defines “meaningful use” as the use of digital medical and health records to:
Improve quality, safety, efficiency, and reduce
health disparities;
Engage patients and their families;
Improve care coordination and population and
public health; and
Maintain privacy and security of patient health
information.
The purpose of the HITECH Act was to address privacy and security concerns linked to electronic storage and transference of protected health information (PHI). HITECH encourages healthcare organizations to update their health records and record systems, and it offers financial incentives to institutions that are in compliance with the requirements of the program.
When eligible professionals or eligible hospitals attest to being in compliance with Medicare’s EHR incentive program requirements, they can file claims for federal funds, which are paid and audited by the Department of Health and Human Services (HHS) through Medicare and Medicaid.
Institutions receiving funds must demonstrate meaningful use
of EHR records or risk potential penalties, including the delay or cancellation
of future payments and full reimbursement of payments already received. In
addition, false statements submitted in filed documents are subject to criminal
laws and civil penalties at both the state and federal levels.
EHR Developers Under Scrutiny by DOJ
EHR vendors also have been investigated and ordered to make
restitutions by the DOJ.
In February, Greenway Health, a Tampa-based EHR developer, agree to pay $57.25 million to resolve allegations related to the False Claims Act. In this case, the government contended that Greenway obtained certification for its “Prime Suite” EHR even though the technology did not meet the requirements for meaningful use.
And EHR vendor eClinicalWorks paid the government $155 million to settle allegations under the False Claims Act. The government maintained that eClinicalWorks misrepresented the capabilities of their software and provided $392,000 in kickbacks to customers who promoted its product.
Legal cases such as these demonstrate that the DOJ will
pursue both vendors and healthcare organizations that misrepresent their
products or falsely attest to interoperability under the terms laid out by
Medicare’s EHR Incentive Program.
Clinical laboratory leaders and pathology groups should carefully
study these cases. This knowledge may be helpful when they are asked to create
and maintain interfaces to exchange patient data with client EHRs.
“Pathologists and medical laboratories may have to demonstrate efficiency and effectiveness to stay in the insurer’s networks and get paid for their services
In recent years, Medicare officials have regularly introduced new care models that include quality metrics for providers involved in a patient’s treatment. Now comes news that a national health insurer is launching an innovative cancer-care model that includes quality metrics for medical laboratories and anatomic pathology groups that deliver diagnostic services to patients covered by this program.
Anatomic pathologists and clinical laboratories know that cancer patients engage with many aspects of healthcare. And that, once diagnoses are made, the continuum of cancer care for these patients can be lengthy, uncomfortable, and quite costly. Thus, it will be no surprise that health insurers are looking for ways to lower their costs while also improving the experience and outcomes of care for their customers.
To help coordinate care for cancer patients while simultaneously addressing costs, Humana, Inc., (NYSE:HUM) has started a national Oncology Model-of-Care (OMOC) program for its Medicare Advantage and commercial members who are being treated for cancer, Humana announced in a press release.
What’s important for anatomic pathologists and clinical
laboratories to know is that the program involves collecting performance
metrics from providers and ancillary services, such as clinical laboratory,
pathology, and radiology. These metrics will determine not only if doctors and
ancillary service providers can participate in Humana’s networks, but also if
and how much they get paid.
Anatomic pathologists and medical laboratory leaders will want to study Humana’s OMOC program carefully. It furthers Humana’s adoption of value-based care over a fee-for-service payment system.
How Humana’s OMOC Program Works
According to Modern Healthcare, “Humana will be looking at several measures to determine quality of cancer care at the practices including inpatient admissions, emergency room visits, medications ordered, and education provided to patients on their illness and treatment.”
As Humana initiates the program with the first batch of
oncologists and medical practices across the US, it also will test performance criteria
that anatomic pathologist groups will need to meet to participate in the
insurer’s network and be paid for services.
The insurer’s metrics address access to care, clinical status assessments, and patient education. Physicians can earn rewards for enhancing their patients’ navigation through healthcare, while addressing quality and cost of care, reported Health Payer Intelligence.
“The experience for cancer care is fragmented,” Bryan Loy, MD (above), Corporate Medical Director of Humana’s Oncology, Laboratory, and Personalized Medicine Strategies Group, told Modern Healthcare. Loy is board-certified in anatomic and clinical pathology, as well as hematology. “Humana wants to improve the patient experience and health outcomes for members. We are looking to make sure the care is coordinated.” (Photo copyright: National Lung Cancer Roundtable/American Cancer Society.)
Humana claims its OMOC quality and cost measurements are
effective in the areas of:
inpatient admissions,
emergency room visits,
medical and pharmacy drugs,
laboratory and pathology services, and
radiology.
To help cover reporting and other costs associated with
participation in the OMOC program, Humana is offering physician practices
analytics data and care coordinating payments, notes Modern Healthcare.
“The practices that improve their own performance over a one-year period will see the care coordination fee from Humana increase,” Julie Royalty, Humana’s Director of Oncology and Laboratory Strategies, told Modern Healthcare.
Value-Based Care Programs are Expensive
Due to the cost of collecting data and increasing staff capabilities to meet program parameters, participating in value-based care models can be costly for medical practices, according to Scottsdale, Ariz.-based Darwin Research Group (DRG), which studies emerging payer models.
Some of the inaugural medical practices in the Humana OMOC
include:
Southern Cancer Center, Alabama;
US Oncology Network, Arizona;
Cancer Specialists of North Florida;
Michigan Healthcare Professionals;
University of Cincinnati Physicians Company; and
Center for Cancer and Blood Disorders, Texas.
Other Payers’ Value-Based Cancer Care Programs
“Depending upon which part of the country you’re in,
alternative payment models in oncology are becoming the norm not the exception,”
noted the DRG study. “Humana is a little late to the party.”
Darwin Research added that Humana may realize benefits from
having observed other insurance company programs, such as:
Humana is not the only payer offering value-based cancer care programs. The Centers for Medicare and Medicaid Services (CMS) Oncology Care Model is a five-year model (2016 through 2021) involving approximately 175 practices and 10 payers throughout America (see above). The healthcare networks and insurers have made payment arrangements with their patients for chemotherapy episode-of-care services, noted a CMS fact sheet. (Graphic copyright: Centers for Medicare and Medicaid Services.)
Humana’s Other Special Pay Programs
Humana has developed other value-based bundled payment
programs as well. It has episode-based
models that feature open participation for doctors serving Humana Medicare
Advantage members needing:
total hip or knee joint replacement (available
nationwide since 2018); and
spinal fusion surgery (launched in 2019).
Humana also started a maternity episode-of-care bundled
payment program last year for its commercial plan members.
In fact, more than 1,000 providers and Humana value-based
relationships are in effect. They involve more than two-million Medicare
Advantage members and 115,000 commercial members.
Clearly, Humana has embraced value-based care. And, to
participate, anatomic pathology groups and medical laboratories will need to be
efficient and effective in meeting the payer’s performance requirements, while
serving their patients and referring doctors with quality diagnostic services.
Doctors may begin ordering FITs in greater numbers, increasing the demand on clinical laboratories to process these home tests
All clinical laboratory managers and pathologists know that timely screening for colon cancer is an effective way to detect cancer early, when it is easiest to treat. But, invasive diagnostic approaches such as colonoscopies are not popular with consumers. Now comes news of a large-scale study that indicates the non-invasive fecal immunochemical test (FIT) can be as effective as a colonoscopy when screening for colon cancer.
FITs performed annually may be as effective as colonoscopies at detecting colorectal cancer (CRC) for those at average risk of developing the disease. That’s the conclusion of a study conducted at the Regenstrief Institute, a private, non-profit research organization affiliated with the Indiana University School of Medicine in Indianapolis, Ind.
The researchers published their findings in the Annals of Internal Medicine (AIM), a journal published by the American College of Physicians (ACP). The team reviewed data from 31 previous studies. They then analyzed the test results from more than 120,000 average-risk patients who took a FIT and then had a colonoscopy. After comparing the results between the two tests, the researchers concluded that the FIT is a sufficient screening tool for colon cancer.
FIT is Easy, Safe, and Inexpensive
As a medical laboratory test, the FIT is low risk, non-invasive,
and inexpensive. In addition, the FIT can detect most cancers in the first
application, according to the Regenstrief Institute researchers. They recommend
that the FIT be performed on an annual basis for people at average risk for
getting colorectal cancers.
“This non-invasive test for colon cancer screening is available for average risk people,” Imperiale told NBC News. “They should discuss with their providers whether it is appropriate for them.”
FIT is performed in the privacy of the patient’s home. To
use the test, an individual collects a bowel specimen in a receptacle provided
in a FIT kit. They then send the specimen to a clinical laboratory for
evaluation. The FIT requires no special preparations and medicines and food do
not interfere with the test results.
Thomas Imperiale, MD (above), is a Lawrence Lumeng Professor of Gastroenterology and Hepatology at Indiana University School of Medicine, and a research scientist at the Regenstrief Institute. He led a study which concluded that FITs are as effective as colonoscopies at detecting cancer in average risk patient populations. Should these conclusions become widely accepted, doctors may begin ordering FITs in greater numbers, increasing the demand on clinical laboratories that process the tests. (Photo copyright: Indiana University School of Medicine.)
‘A Preventative Health Success Story’
The FIT can be calibrated to different sensitivities at the
lab when determining results. Imperiale and his team found that 95% of cancers
were detected when the FIT was set to a higher sensitivity, however, that
setting resulted in 10% false positives. At lower sensitivity the FIT produced
fewer false positives (5%), but also caught fewer cancers (75%). However, when
the FIT was performed every year, the cancer detection rate was similar at both
sensitivities over a two-year period.
“FIT is an excellent option for colon cancer screening only if it is performed consistently on a yearly basis,” Felice Schnoll-Sussman, MD, told NBC News. Sussman is a gastroenterologist and Professor of Clinical Medicine at Weill Cornell Medicine. “Colon cancer screening and its impact on decreasing rates of colon cancer is a preventative health success story, although we have a way to go to increase rates to our previous desired goal of 80% screened in the US by 2018.”
The FIT looks for hidden blood in the stool by detecting protein hemoglobin found in red blood cells. A normal result indicates that FIT did not detect any blood in the stool and the test should be repeated annually. If the FIT comes back positive for blood in the stool, other tests, such as a sigmoidoscopy or colonoscopy should be performed. Cancers in the colon may not always bleed and the FIT only detects blood from the lower intestines.
Patients are Skipping the Colonoscopy
Approximately 35% of individuals who should be receiving colonoscopies do not undergo the test, NBC News noted. The American Cancer Society (ACS) lists the top five reasons people don’t get screened for colorectal cancer are that they:
fear the test will be difficult or painful;
have no family history of the disease and feel
testing is unnecessary;
have no symptoms and think screening is only for
those with symptoms;
are concerned about the costs associated with
screening; and
they are concerned about the complexities of
taking the tests, including taking time off from work, transportation after the
procedure, and high out-of-pocket expenses.
“Colorectal cancer screening is one of the best opportunities to prevent cancer or diagnose it early, when it’s most treatable,” Richard Wender, MD, Chief Cancer Control Officer for the ACS stated in a press release. “Despite this compelling reason to be screened, many people either have never had a colorectal cancer screening test or are not up to date with screening.”
Colorectal cancer is the third most common cancer diagnosed in both men and women in the United States. The ACS estimates there will be 101,420 new cases of colon cancer and 44,180 new cases of rectal cancer diagnosed this year. The disease is expected to be responsible for approximately 51,020 deaths in 2019.
New cases of the disease have been steadily decreasing over
the past few decades in most age populations, primarily due to early screening.
However, the overall death rate among people younger than age 55 has increased
1% per year between 2007 and 2016. The ACS estimates there are now more than
one million colorectal cancer survivors living in the US.
The ACS recommends that average-risk individuals start
regular colorectal cancer screenings at age 45. The five-year survival rate for
colon cancer patients is 90% when there is no sign that the cancer has spread
outside the colon.
Clinical laboratory professionals may find it unpleasant to
test FIT specimens. Opening the specimen containers and extracting the samples
can be messy and malodorous. However, FITs are essential, critical tests that
can save many lives.
From point-of-care diagnostic tests to ancestral DNA home-testing, this company’s spit tubes are used by more medical laboratories than any other brand
Most clinical laboratory specialists know that OraSure Technologies of Bethlehem, Pa., was the first company to develop a rapid point-of-care DNA diagnostic test for HIV back in the 1990s. This was a big deal. It meant physicians could test patients during office visits and receive the results while the patients were still in the office. Since many patients fail to follow through on doctors’ test orders, this also meant physicians were diagnosing more patients with HIV than ever before.
Today, OraSure is the dominant company in the spit tube
industry. OraSure claims its tubes contain patented chemical preservatives that
can maintain the specimen’s integrity for up to two years at room temperature.
That’s a long time. And this one feature has made OraSure popular with
direct-to-consumer (DTC) genetic home-test developers.
OraSure provides nearly all of the specimen receptacles used
by individuals searching for their ancestral roots. It’s estimated that about
90% of the DTC genetic-testing market uses the company’s spit tubes. This is
partly because OraSure makes the only tubes approved by the US Food and Drug
Administration (FDA) for home DNA-testing purposes.
“The FDA approval gives customers confidence,” Mark Massaro, Managing Director, Senior Equity Analyst at investment bank Canaccord Genuity Group, told Bloomberg. “That, and they can preserve saliva for a long time.”
The OraSure spit tube above contains a patented mix of chemicals that can maintain saliva’s integrity for up to two years at room temperature. This is critical for ensuring specimens arrive at medical laboratories in usable condition to produce accurate test results. (Photo copyright: Zhongjia Sun/Bloomberg Businessweek.)
Spit, Close, Recap, Send
To use the saliva-testing DNA kits, an individual first
spits into the tube and then snaps the cap on the tube shut. This action
perforates a membrane which contains a patented, chemical mix of preservatives.
These chemicals help preserve the sample and minimize contamination from
non-human DNA that may be present.
“You’ve got to make it as easy as possible for a person to
spit in the tube, close the tube, recap the tube, and send it to you without
any variation,” Stephen
Tang, PhD, President and Chief Executive Officer at OraSure, told Bloomberg.
Saliva samples are very susceptible to environmental factors
like temperature and are extremely time sensitive. They need to be properly
handled and stored to prevent any degradation and ensure the most accurate test
results. Once in the spit tube, a saliva sample can last more than two years at
room temperature, according to the company.
“That’s the secret,” Tang stated. “Saliva is not pure. It’s
got a lot of bacteria and other stuff swimming in it.”
OraSure reported the company made $182 million in revenue in
2018, with about $20 million of that amount being profit. DNA Genotek, Inc., a subsidiary of OraSure
designed the T-shaped spit tubes being used for consumer-DNA testing kits.
Other Clinical Laboratory Uses for Specimen-Collection Devices
In addition to the consumer-DNA industry, OraSure’s tube technology is used in clinical and academic laboratory situations as well as in veterinary DNA testing. The company is focused on expanding the uses for their specimen-collection technology. They have recently begun using their technology to collect urine specimens for diagnosing sexually transmitted diseases and other conditions. OraSure also has added devices for feces collection, to better compete in the developing field of microbiome for gut bacteria analysis.
“We are all about the integrity of the sample collection,”
Tang says. “It’s a wide-open field.”
Ancestry Sued by OraSure
In 2017, Ancestry.com agreed to pay OraSure $12.5 million to
settle a lawsuit which alleged the company had copied OraSure’s patented DNA
testing technology to produce their own saliva-based DNA test.
According to the lawsuit, Ancestry.com purchased saliva test
kits from DNA Genotek in 2012 and 2013 for the purpose of collecting saliva
samples from their customers. In 2013, Ancestry.com filed for a patent of their
own for an improved variation of the kits reportedly without DNA Genotek’s
consent.
OraSure also has devices for substance abuse testing,
cryosurgical kits for the testing of skin lesions, and kits for forensic
toxicology.
Maintaining specimen integrity is critical to ensure lab
test results are accurate and reproducible. OraSure’s spit tube technology
solves the problem of preserving specimens while they are transported to
clinical laboratories and other pathology facilities.
Clinical laboratories could offer services that complement SDH programs and help physicians find chronic disease patients who are undiagnosed
Insurance companies and healthcare providers increasingly consider social determinants of health (SDH) when devising strategies to improve the health of their customers and affect positive outcomes to medical encounters. Housing, transportation, access to food, and social support are quickly becoming part of the SDH approach to value-based care and population health.
For clinical laboratory managers and pathologists this rapidly-developing trend is worth watching. They can expect to see more providers and insurers in their communities begin to offer these types of services to individuals and patients who might stay healthier and out of the hospital as a result of SDH programs. Clinical laboratories should consider strategies that help them provide medical lab testing services that complement SDH programs.
Medical laboratories, for example, could participate by offering
free transportation to patient
service centers for homebound chronic disease patients who need regular
blood tests. Such community outreach also could help physicians identify people
with chronic diseases who might otherwise go undiagnosed.
Anthem Offers Social
Determinants of Health Package
In fact, health benefits giant Anthem, Inc. (NYSE:ANTM) partly attributes its 2019 first quarter 14% increase of Medicare Advantage members to a new “social determinants of health benefits package” comprised of healthy meals, transportation, adult day care, and homecare, according to Forbes.
“Our focus on caring for the whole person is designed to deliver
better care and outcomes, reduce costs, and ultimately accelerate growth,” Gail Boudreaux,
Anthem President and CEO, stated in a call to analysts, Forbes reports.
An Anthem news release states that SDH priorities for payers, providers, and other stakeholders should focus on enhancing individuals’ access to food, transportation, and social support.
In the Anthem news release, which announced the publication of a white paper that “outlines key differences in how individuals and the public perceive social determinants of health,” Jennifer Kowalski (above), Vice President of the Anthem Public Policy Institute stated, “By better understanding how individuals view and talk about social determinants, payers and providers alike can identify new and improved ways to engage with them to more effectively improve their health and wellbeing and the delivery of healthcare.” (Photo copyright: LinkedIn.)
CMS Expands Medicare
Advantage Plans to Include Social Determinants of Health
The Centers for Medicare and Medicaid Services announced that, effective in 2019, Medicare Advantage plans can offer members benefits that address social determinants of health. Medicare Advantage members may be covered for services such as adult day care, meal delivery, transportation, and home environmental services that relate to chronic illnesses.
Humana’s ‘Bold Goal’
Humana, Inc. (NYSE:HUM) calls its SDH focus the BoldGoal. The program aims to improve health in communities it serves by 20% by 2020.
“The social barriers and health challenges that our Medicare Advantage members and others face are deeply personal. This requires us to become their trusted advocate that can partner with them to understand, navigate, and address these barriers and challenges,” said William Shrank, MD, Humana’s Chief Medical Officer, in a news release.
UnitedHealthcare
Investing More than $400 Million in Housing
Meanwhile, since 2011, UnitedHealthcare (NYSE:UNH) also has invested in affordable housing and social determinants of health, Health Payer Intelligence reported.
In a news release, UnitedHealthcare, the nation’s largest health insurer, described how it is investing more than $400 million in 80 affordable US housing communities, including:
$12 million, PATH Metro Villas, Los Angeles;
$11.7 million, Capital Studios, Austin;
$14.5 million allocated to Minneapolis military
veterans housing;
$7.9 million, New Parkridge (in Ypsilanti, Mich.)
affordable housing complex;
$21 million earmarked to Phoenix low- and moderate-income
families needing housing and supportive services;
$7.8 million, Gouverneur Place Apartments, Bronx,
New York; and
$7.7 million, The Vinings, Clarksville, Tenn.
“Access to safe and affordable housing is one of the
greatest obstacles to better health, making it a social determinant that
affects people’s well-being and quality of life. UnitedHealthcare partners with
other socially minded organizations in helping make a positive impact in our
communities,” said Steve Nelson,
UnitedHealthcare’s CEO, in the news
release.
According to the American Hospital Association (AHA) and the Health Research and Educational Trust (HRET), housing, or lack of it, impacts health. In “Housing and the Role of Hospitals,” the second guide in the organizations’ “Social Determinants of Health Series,” AHA and HRET state that 1.48 million people are homeless each year, and that unstable living conditions are associated with less preventative care, as well as the propensity to acquire diabetes, cardiovascular disease, chronic obstructive pulmonary disorder, and other healthcare conditions.
Social determinants of health programs are gaining in
popularity. And as they become more robust, proactive clinical laboratory
leaders may find opportunities to work with insurers and healthcare providers
toward SDH goals to help healthcare consumers stay healthy, as well as reducing
unnecessary hospital admissions and healthcare costs.
Consumer demand and federal requirements for price transparency affect how clinical laboratories and anatomic pathology groups meet patients’ expectations while navigating complex payer agreements
Regardless of a clinical laboratory’s payer mix and revenue cycle management (RCM) system, the demand for greater price transparency impacts laboratory services just as it does other healthcare services. Addressing new federal policies that support price transparency may require medical laboratory managers to alter how they approach RCM and patient communications.
Patient access management (PAM) is what some early-adopter medical labs and pathology groups are using to respond to these new federal policies and changing patient expectations. PAM can be an effective tool to fulfill complex payer requirements and implement consumer-friendly healthcare services. Not only does this comply with federal guidelines, it helps independent laboratories increase revenue by lowering denial rates.
How
and When Clinical Laboratories Should Implement Patient Access Management
Revenue
cycle experts say clinical laboratories are in a position to take an active
role in the pricing transparency debate.
“If labs don’t control the pricing narrative, someone else will,” stated Walt Williams, Director of Revenue Cycle Optimization and Strategy for Quadax, a firm that has studied revenue trends in healthcare for more than 40 years, in an exclusive interview with Dark Daily.
He
says, given these new demands on clinical laboratories and pathology groups,
implementing patient access management practices ensures a satisfactory patient
and physician experience and reduces the financial risk related to trends in
uncollected revenue.
“In this
age of increasing consumerism—along with the complex challenges of navigating
the payer landscape and pre-empting administrative denials—it’s no wonder
independent labs are turning to new patient access technology solutions to
avoid leaving money on the table,” Williams said.
Patient
access management solutions allow clinical laboratories to:
obtain
accurate patient demographic information,
verify
insurance coverage and eligibility, and
gain
clarity on payer rules regarding prior authorization and medical necessity.
These
capabilities enable medical laboratories to secure appropriate reimbursement
closer to the date of service. PAM also can provide the ordering-physician with
financial counseling and guidelines on a patient’s financial obligation. This
would be shared with the patient to help prevent surprise billing.
New
Fact of Life for Labs: Patients Are the New Payers
Medical laboratory patient-access representatives must employ proper patient-liability collection techniques before, during, and after each date of service. This has become increasingly challenging as more patients join high-deductible health plans (HDHPs) and take on more financial responsibility. The problem for labs is that meeting the expectations of consumers requires a different toolset than meeting the needs of complex payer requirements.
Additionally, evolving policies in prior authorization, medical necessity, and coding (see, “Labs Get High Denial Rates Under New NCCI Rules,” The Dark Report) are resulting in potential payment traps for patients and known revenue traps for providers and suppliers.
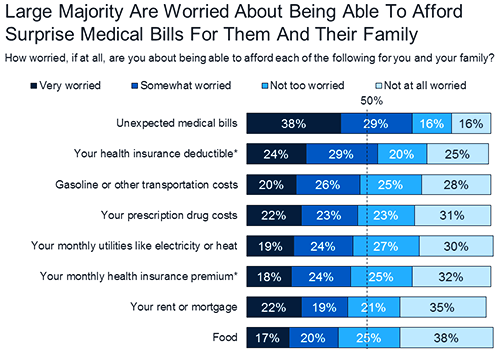
The graphic above, taken from a KFF Health Tracking Poll conducted in 2018, lists “unexpected medical bills” as the top financial fear among Americans. “Four in 10 (39%) insured adults ages 18-64 say there has been a time in the past 12 months when they received care from a doctor, hospital, or lab that they thought was covered and their health plan either didn’t cover the bill at all or covered less than they expected,” the KFF poll notes. This illustrates the critical importance for clinical laboratories to implement patient access management protocols. (Graphic copyright: Kaiser Family Foundation.)
While
the current high cost of healthcare will likely continue for some time,
publishing information about the lab’s policies can help consumers view choices
when it comes to selecting laboratory tests and anticipating potential payment
obligations.
Henry Ford Health System, for example, posted information about prior authorization as it relates to its pathology and laboratory services.
Consumer-Facing
Price Transparency and CMS Requirements
Rooted
in price transparency regulations issued in July 2018, the federal Centers for
Medicare and Medicaid Services (CMS) encouraged “all providers and suppliers of
healthcare services to undertake efforts to engage in consumer-friendly
communication of their charges to help patients understand what their potential
financial liability might be for services they obtain, and to enable patients
to compare charges for similar services. We encourage providers and suppliers
to update this information at least annually, or more often as appropriate, to
reflect current charges.”
How
should we define “standard charges” in provider and supplier settings? Is the
best measure of a provider’s or supplier’s standard charges its chargemaster,
price list, or charge list?
What
types of information would be most beneficial to patients … enable patients to
use charge and cost information in their decision-making?
How
can information on out-of-pocket costs be provided to better support patient
choice and decision-making? What can be done to better inform patients of their
financial obligations?
What
changes would need to be made by providers and suppliers to provide patients
with information on what Medicare pays for a particular service performed by
that provider or supplier?
These
considerations and more can help the development of patient access management
and consumer-friendly communication initiatives that are tailored to clinical laboratory
services.
Patient
Access Management for Clinical Laboratories
Patient
access management facilitates critical components of the revenue cycle.
However, it must be fine-tuned to fit each healthcare provider’s unique revenue
cycle process. This includes clinical laboratory and anatomic pathology
services.
“Having
business rules and workflows based on best practices to verify patient
demographics, support insurance discovery, and navigate prior authorizations
are now a minimum requirement for any healthcare provider to maintain financial
viability,” Williams notes.
To help clinical laboratories fulfill CMS’ patient access guidelines—including best practices for reversing the trend of uncollected revenue—a free white paper titled, “Patient Access Antidote: Retaining More Revenue with Front-End Solutions,” has been published by Dark Daily in partnership with Quadax.
The
white paper will provide useful insights regarding front-end patient access
management. And it will equip clinical laboratories and pathology groups with
the expert tools and solutions they need to optimize their cash flow and
successfully meet key revenue cycle objectives.