The resulting genomic dataset may provide useful diagnostic insights that can be used by clinical laboratory and pathology professionals to learn how and why some people age with good health
Why do some seniors age in good health and other seniors
suffer with multiple chronic conditions? A new genetic database is using whole-genomic
sequencing (WGS) to answer that question in ways that may benefit medical
laboratories.
Because of the rapid aging of populations in the United
States and other developed nations throughout the world, there is keen interest
in how to keep seniors healthy. In fact, developing effective lab testing
services in support of improved senior health is one of the big opportunities
for both clinical laboratories and anatomic
pathology groups.
Until recent years, most clinical
pathologists dealt primarily with lab tests that used specimens such as blood
and urine. However, genetics researchers are using WGS to discover new causes
for many chronic illnesses. And the tools these researchers are developing offer
pathologists and clinical
laboratories powerful new ways to help doctors diagnose disease.
Through the use of WGS, the MGRB now features a huge
database of thousands of healthy elderly people. The data it contains may enable
pathology scientists to learn, from a genetic standpoint, why some people age
healthfully while others do not.
The researchers published their work titled, “The Medical
Genome Reference Bank: A Whole-Genome Data Resource of 4,000 Healthy Elderly
Individuals. Rationale and Cohort Design,” in the European Journal of
Human Genetics.
Finding New Applications for Genetic Data
According to the UNSW published study, “The MGRB is comprised
of individuals consented through the biobank programs of two contributing
studies … Each sample is from an individual who has lived to [greater than or
equal to] 70 years with no reported history or current diagnosis of
cardiovascular disease, dementia, or cancer, as confirmed by the participating
studies at recent follow-up study visits.”
The researchers noted in their paper, “Aged and healthy
populations are more likely to be selectively depleted of pathogenic alleles, and therefore
particularly suitable as a reference population for the major diseases of
clinical and public health importance.”
The MGRB plans to make its database openly accessible to the
international research community through its website once all 4,000 samples
have been sequenced. Currently, about 3,000 of the samples have been analyzed,
as noted on the Garvan website,
which is tracking the MGRB’s progress.
“The Medical Genome Reference Bank can tell us much about what it means to grow old but remain well, and is a powerful tool to help us deconstruct the genetics of common diseases,” said David Thomas, PhD (above), an NHMRC Principal Research Fellow, Director of The Kinghorn Cancer Center, and Head of the Cancer Division of the Garvan Institute in New South Wales, AU, in a statement reported by GenomeWeb. (Photo copyright: South West Sydney Research.)
Personal Genetic Data in Precision Medicine
“The integration of genomic knowledge and technologies into
healthcare is revolutionizing the way we approach clinical and public health
practice,” Caron
M. Molster, et al, noted in, “The Evolution of Public Health
Genomics: Exploring Its Past, Present, and Future,” published in Frontiers
in Public Health. Molster is Manager at the Health Department Western
Australia in Perth, and lead author of the paper.
“Public health genomics has evolved to responsibly integrate
advancements in genomics into the fields of personalized
medicine and public health,” the researchers wrote.
The 100,000
Genomes Project in the United Kingdom is sequencing the genomes of people
who have rare diseases and their families. Researchers all over the world are collecting
genomic data with plans to use it in different ways, and on various chronic
disease populations, in pursuit of precision medicine
goals.
Molster and her co-authors noted the comparable development
of genetic sequencing and precision medicine in their paper.
“Parallel to the developments in precision medicine has been
the advancement of technologies that enable the production, aggregation,
analysis, and dissemination of extremely large volumes of individual- and
population-level data on genes, environment, behavior, and other social and
economic determinants of health. These data have proven useful in finding new
correlations, patterns and trends, particularly those involving complex
interactions, in relation to diseases, pathogens, exposures, behaviors,
susceptibility (risk), and health outcomes in populations,” they wrote.
According to Paul Lacaze, PhD,
Head of the Public Health Genomics Program at Monash University, one of the
challenges in interpreting whole-genome data in order to diagnose disease is
“discriminating rare candidate disease-causing variants from the large numbers
of benign variants unique to each individual. Reference populations are
powerful filters,” he noted in the MGRB paper.
The MGRB database provides just such a powerful reference
population, giving researchers who are studying specific diseases a tool for
comparison.
Other Studies into Heathy Aging
Other initiatives to create datasets of genome information
for specific populations also are underway. The Scripps
Translational Science Institute (STSI) in La Jolla, Calif., has been
studying healthy aging since 2007. That’s when STSI launched the Wellderly Study,
according to a news
release. As of 2016, they had sequenced the genomes of 600 study
participants, as well as 511 samples for comparison from a study being conducted
separately by the Inova Translational Medicine Institute, a paper in Nature noted.
Another effort being conducted in China involves a database
called PGG.Population.
These researchers seek to “create a comprehensive depository of geographic and
ethnic variation of human genome, as well as a platform bringing influence on
future practitioners of medicine and clinical investigators,” according to
their 2018 paper published in Nucleic Acids
Research.
In this case, rather than identifying common genomic
variants among a specific population, such as the healthy elderly, the
researchers are working to understand how genetic variations are distributed
among specific populations. “The PGG.Population database documents 7,122
genomes representing 356 global populations from 107 countries and provides
essential information for researchers to understand human genomic diversity and
genetic ancestry,” wrote the researchers.
Each of these disparate datasets represents paths of
investigation that could lead to a better understanding of personal and public health.
As technologies continue to develop that enable scientists to sift through the
massive amount of WGS data being generated, a clearer picture of what healthy
aging at the genetic level looks like will likely emerge.
Precision medicine is leading to precision public health,
and clinical pathology laboratories are important parts of the public health
puzzle.
Clinical laboratories that service both settings could be impacted as new CMS proposed rule attempts to align Medicare’s payment policies for outpatient and in-patient settings
Hospital outpatient revenue is catching up to inpatient
revenue, according to data released from the American
Hospital Association (AHA). This increase is part of a growing trend to
reduce healthcare costs by treating patients outside of hospital settings. It’s
a trend that is supported by the White House and Medicare and continues to
impact clinical
laboratories, which serve both hospital inpatient and outpatient customers.
The AHA published this study data in its annual Hospital Statistics, 2019Edition. The data comes from a 2017 survey of 5,262
US hospitals. The report includes data about utilization, revenue, expenses,
and other indicators for 2017, as well as historical data.
The AHA statistics on outpatient revenue suggest providers
nationwide are working to keep people out of more expensive hospital settings. Hospitals,
like medical
laboratories, appear to be succeeding at developing outpatient and outreach
services that generate needed operating revenue.
This aligns with Medicare’s push to make healthcare more accessible through outpatient settings, such as urgent care clinics and physician’s offices. A growing trend Dark Daily has covered extensively.
Outpatient Revenue
Climbs
In its coverage of
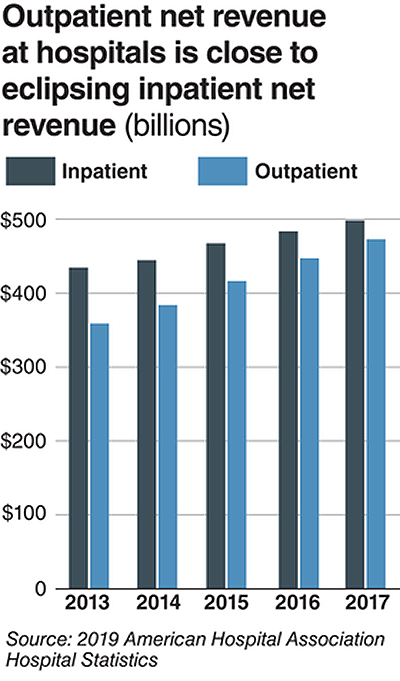
the AHA’s study, Modern Healthcare reported that 2017
hospital net inpatient revenue was $498 billion and net outpatient revenue was
$472 billion.
The Becker’s Hospital CFO Report notes that
gross inpatient revenue in 2017 was $92.7 billion higher than gross outpatient
revenue. But in 2016, gross inpatient revenue was much further ahead—$129.5
billion more than gross outpatient revenue. The “divide” between inpatient and
outpatient revenue is narrowing, Becker’s reports.
The graphic above illustrates the shrinking gap between hospital inpatient and outpatient revenues. “Outpatient revenue will ultimately eclipse inpatient revenue,” Chuck Alsdurf, Director of Healthcare Finance Policy and Operational Initiatives at the Healthcare Financial Management Association (HFMA), told Modern Healthcare. (Graphic copyright: Modern Healthcare/AHA.)
The Becker’s
report also stated:
Admissions increased by less than 1% to 34.3
million in 2017, up from 34 million in 2016;
Inpatient days were flat at 186.2 million;
Outpatient visits rose by 1.2% to 766 million in
2017; and,
Outpatient revenue increased 5.7% between 2016
and 2017.
Similar Study Offers Additional
Insight into 2018 Outpatient Revenue
A benchmarking report by Crowe,
a public accounting, consulting, and technology firm, which analyzed data from
622 hospitals for the period January through September of 2017 and 2018, showed
the following, as reported by RevCycleIntelligence:
Inpatient volume was up 0.6% in 2018 and gross
revenue per case grew by 5.3%;
Outpatient services rose 2.4% in 2018 and gross
revenue per case was up 7.1%.
Physicians’ Offices
Have Lower Prices for Some Hospital Outpatient Services
Everything, however, is relative. When certain healthcare
services traditionally rendered in physician’s offices are rendered, instead,
in hospital outpatient settings, the numbers tell a different story.
In fact, according to the Health
Care Cost Institute (HCCI), the price for services was “always higher” when
performed in an outpatient setting, as compared to doctor’s offices.
HCCI analyzed services at outpatient facilities as well as
those appropriate to freestanding physician offices. They found the following
differences in 2017 prices:
Diagnostic and screening ultrasound: $241 in
physician’s office—$650 in hospital outpatient setting;
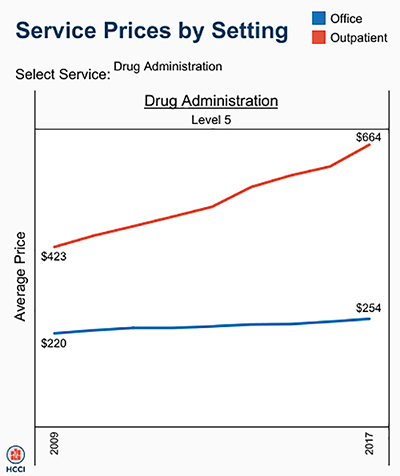
Level 5 drug administration: $254 in office—$664
in hospital outpatient setting;
Upper airway endoscopy: $527 in office—$2,679 in
hospital outpatient setting.
One example where hospital outpatient settings provide similar services at increased costs is in drug administration, as the graphic above illustrates. “The difference was higher than I expected. With some services, the price is two or three times higher when rendered in the outpatient setting,” Julie Reiff, HCCI researcher and report author, told Fierce Healthcare. (Graphic copyright: HCCI.)
Medicare Proposed
Rule Would Change How Hospital Outpatient Clinics Get Paid
Meanwhile, the Centers for
Medicare and Medicaid Services (CMS) has released its final rule (CMS-1695-FC),
which make changes to Medicare’s hospital outpatient prospective payment and
ambulatory surgical center payment systems and quality reporting programs.
In a news
release, CMS stated that it “is moving toward site neutral payments for
clinic visits (which are essentially check-ups with a clinician). Clinic visits
are the most common service billed under the OPPS [Medicare’s Hospital
Outpatient Prospective Payment System). Currently, CMS often pays more for
the same type of clinic visit in the hospital outpatient setting than in the
physician office setting.”
“CMS is also proposing to close a potential loophole through
which providers are billing patients more for visits in hospital outpatient
departments when they create new service lines,” the news release states.
Hospitals are fighting the policy change through a lawsuit, Fierce Healthcare reported.
In summary, clinical laboratories based in hospitals and
health systems are in the outpatient as well as inpatient business. Medical laboratory
tests contribute to growth in outpatient revenue, and physician offices compete
with clinical laboratories for some outpatient tests and procedures. Thus, a new
site-neutral CMS payment policy could affect the payments hospitals receive for
clinic visits by Medicare patients.
This research could lead to a useful liquid biopsy test that would be a powerful new tool for clinical laboratories and anatomic pathologists
Cancer researchers have long sought the Holy Grail of
diagnostics—a single biomarker that can quickly detect cancer from blood or
biopsied tissue. Now, researchers in Australia may have found that treasure. And
the preliminary diagnostic test they have developed reportedly can return
results in just 10 minutes with 90% accuracy.
In a news release, University of Queensland researchers discussed identifying a “simple signature” that was common to all forms of cancer, but which would stand out among healthy cells. This development will be of interest to both surgical pathologists and clinical laboratory managers. Many researchers looking for cancer markers in blood are using the term “liquid biopsies” to describe assays they hope to develop which would be less invasive than a tissue biopsy.
“This unique nano-scaled DNA signature appeared in every type of breast cancer we examined, and in other forms of cancer including prostate, colorectal, and lymphoma,” said Abu Sina, PhD, Postdoctoral Research Fellow at the Australian Institute for Bioengineering and Nanotechnology (AIBN), University of Queensland (UQ), in the news release.
“We designed a simple test using gold nanoparticles that
instantly change color to determine if the three-dimensional nanostructures of cancer
DNA are present,’ said Matt
Trau, PhD, Professor of Chemistry at the University of Queensland, and
Deputy Director and Co-Founder of UQ’s AIBN, in the news release.
The team’s test is preliminary, and more research is needed before
it will be ready for Australia’s histopathology laboratories (anatomic
pathology labs in the US). Still, UQ’s research is the latest example of how
increased knowledge of DNA is making it possible for researchers to identify
new biomarkers for cancer and other diseases.
“We certainly don’t know yet whether it’s the holy grail for
all cancer diagnostics, but it looks really interesting as an incredibly simple
universal marker of cancer, and as an accessible and inexpensive technology
that doesn’t require complicated lab-based equipment like DNA sequencing,” Trau
added.
The UQ researchers published their study in the journal Nature Communications. In it, they noted that “Epigenetic reprogramming in cancer genomes creates a distinct methylation landscape encompassing clustered methylation at regulatory regions separated by large intergenic tracks of hypomethylated regions. This methylation landscape that we referred to as ‘Methylscape’ is displayed by most cancer types, thus may serve as a universal cancer biomarker.”
While methyl patterning is not new, the UQ researchers say they were the first to note the effects of methyl pattern in a particular solution—water. With the aid of transmission electron microscopy, the scientists saw DNA fragments in three-dimensional structures in the water. But they did not observe the signature in normal tissues in water.
“To date, most research has focused on the biological consequences of DNA Methylscape changes, whereas its impact on DNA physicochemical properties remains unexplored,” UQ scientists Matt Trau, PhD (left), Abu Sina, PhD (center), and Laura Carrascosa (right), wrote in their study. “We exploit these Methylscape differences to develop simple, highly sensitive, and selective electrochemical or colorimetric one-step assays for the detection of cancer.” (Photo copyright: University of Queensland.)
Their test averaged 90% accuracy during the testing of 200
human cancer samples. Furthermore, the researchers found the DNA structure to
be the same in breast, prostate, and bowel cancers, as well as lymphomas, noted
The Conversation.
“We find that DNA polymeric
behavior is strongly affected by differential patterning of methylcytosine
leading to fundamental differences in DNA solvation and DNA-gold affinity
between cancerous and normal genomes,” the researchers wrote in NatureCommunications.“We exploit
these methylscape differences to develop simple, highly sensitive, and
selective electrochemical or one-step assays for detection of cancer.”
Next Steps for the
“Gold Test”
“This approach represents an exciting step forward in
detecting tumor DNA in blood samples and opens up the possibility of a generalized
blood-based test to detect cancer, Ged Brady, PhD, Cancer Research UK
Manchester Institute, told The
Oxford Scientist. “Further clinical studies are required to evaluate
the full clinic potential of the method.”
Researchers said the next step is a larger clinical study to
explore just how fast cancer can be detected. They expressed interest in
finding different cancers in body fluids and at various stages. Another opportunity
they envision is to use the cancer assay with a mobile device.
DiCarlo told USA Today
that such a mobile test could be helpful to clinicians needing fast answers for
people in rural areas. However, he’s also concerned about false positives. “You
don’t expect all tumors to have the same methylation pattern because there’s so
many different ways that cancer can develop,” he told USA Today. “There
are some pieces that don’t exactly align logically.”
The UQ researchers have produced an intriguing study that differs
from other liquid biopsy papers covered by Dark Daily. While their test may need to be used in combination with other
diagnostic tests—MRI, mammography, etc.—it has the potential to one day be used
by clinical laboratories to quickly reveal diverse types of cancers.
Expanded ‘Cancer Gene Census’ is expected to accelerate development of new therapeutics and biomarker-based personalized medicine diagnostic tests for disease; could be useful for anatomic pathologists
Oncology is one of the fastest-developing fields in precision medicine and use of DNA-based diagnostics. Surgical pathologists are helping many cancer patients benefit from the use of a companion genetic test that shows their tumors are likely to respond to a specific drug or therapy. Consistent with that work, researchers in the United Kingdom (UK) have now produced the first comprehensive summary of all genes known to be strongly associated with cancer in humans.
The expansion of the “Cancer Gene Census” is noteworthy for anatomic pathologists who should expect to see the information increase the understanding of cancer causes and accelerate the development of new therapeutics and biomarker-based molecular diagnostics.
In this latest Cancer Gene Census, researchers from the Wellcome Sanger Institute (WSI) used CRISPR gene editing systems to produce an expanded catalog of 719 cancer-driving genes in humans.
According to a review article on the project published in Nature Reviews Cancer, “The recent expansion includes functional and mechanistic descriptions of how each gene contributes to disease generation in terms of the key cancer hallmarks and the impact of mutations on gene and protein function.”
The 2018 Cancer Gene Census from the Wellcome Sanger Institute in the United Kingdom summarizes 719 genes suspected of causing cancer in humans and describes how they function across all forms of the disease. (Photo copyright: Wellcome Sanger Institute.)
The Catalogue of Somatic Mutations in Cancer (COSMIC) provided the foundation for the WSI’s research. It involved manually condensing almost 2,000 research papers to develop evidence for a gene’s role in cancer.
While the COSMIC database characterizes more than 1,500
forms of human cancer and types of mutations, the U.K.’s Cancer Gene Census
goes further and “describes which genes are fundamentally involved and
describes how these genes cause disease,” a Wellcome Sanger Institute news
release states.
“For the first time ever, functional changes to these genes
are summarized in terms of the 10 cancer hallmarks—biological processes that
drive cancer,” the statement explains. “Mutations in some genes lead to errors
in repairing DNA, whereas mutations in other genes can suppress the immune
system or promote tumor invasion or spreading. Across the 700 genes in the
Cancer Gene Census, many have two or more different ways of causing cancer.”
Zbyslaw Sondka,
PhD, lead author on the WSI project, believes their study has provided
scientists with much needed new insights. “Scientific literature is very compartmentalized.
With the Cancer Gene Census, we’re breaking down all those compartments and
putting everything together to reveal the full complexity of cancer genetics,” he
noted in a WSI
article.
“This is the broadest and most detailed review of human
cancer genes and their functions ever created and will be continually updated
and expanded to keep it at the forefront of cancer genetics research,” Sondka
added.
Making Precision
Medicine More Precise
An understanding of the roles played by different genes in
various cancers is key to enabling researchers to develop drugs that will be
effective against individual cancers.
“The combination of the Cancer Gene Census with COSMIC will
enable researchers to investigate individual mutations and try to find good
targets for anti-cancer drugs based on the actual processes involved,” Simon Forbes, PhD,
Senior Author of the Cancer Gene Census paper and Director of COSMIC at the
Wellcome Sanger Institute, stated in the WSI news release.
Simon Forbes, PhD (above), Director of COSMIC at the Wellcome Sanger Institute and Senior Author of the Cancer Gene Census paper, believes the institute’s latest Cancer Gene Census, which catalogs 719 cancer-causing genes, will “help make precision medicine even more precise” by allowing “biologists and pharmaceutical scientists to see patterns and target particular pathways with anti-cancer drugs, not solely single genes.” (Photo copyright: Wellcome Sanger Institute.)
The path to precision medicine cancer treatments was further boosted this month when Wellcome Sanger Institute researchers, in partnership with the Open Targets Platform, announced a new system to prioritize and rank 600 drug targets that show the most promise for development into cancer treatments, noted a WSI statement.
The WSI/Open Targets team published its research in the international science journal Nature.
CRISPR-Cas9 and
Personalized Medicine
This latest research springboards off one of the largest CRISPR (Clustered Regularly Interspaced Short Palindromic Repeats)-Cas9 screens of cancer genes to date. Researchers used CRISPR gene-editing systems to disrupt every gene within 30 different types of cancers and locate several thousand key genes essential for cancer’s survival. They then identified 600 genes that potentially could be used in personalized medicine treatments.
“The results bring researchers one step closer to producing
the Cancer
Dependency Map, a detailed rulebook of precision cancer treatments to help
more patients receive effective therapies,” the Wellcome Sanger Institute statement
notes.
Anatomic pathologists and clinical laboratories should note
the speed at which development of useful biomarkers for diagnosing cancer is
progressing. All labs will want to be prepared to capitalize on those
advancements through the lab testing services they offer in their medical laboratories.
As a
result of the drive toward consumer-driven healthcare, and because of rising
health insurance deductibles,patients are increasingly becoming
the new payers. Efficient patient access management is now viewed as critical
to reversing the resulting trend of uncompensated care, and to meeting the
lab’s revenue cycle objectives.
As patients take on more risk and assume more
of their own healthcare costs, and as registration errors, authorization, and
medical necessity continue to contribute to a large percentage of claim
denials—laboratory leaders need to examine new patient access technologies and
modernize their collection practices. In order to
continue to profitably provide quality care and to meet revenue cycle
objectives, it is crucial for labs to get a handle on plummeting accounts
receivable.
DarkDaily.com is
pleased to offer a recently published free White Paper that covers common trends having an impact on
revenue cycle management and best patient access practices, as well as recommended
strategies that labs and pathology groups can employ to take a proactive
approach to their collection practices—and why it’s so important for the
process to begin upfront.
“Patient
Access Antidote: Retaining More Revenue with Front-End Solutions” shares useful insights regarding front-end patient access
management, and equips clinical laboratories and pathology groups with the expert tools and solutions they need to optimize their cash flow and
successfully meet key revenue cycle objectives.
Just a few examples of the best practices covered in this complimentary White Paper: determining patient responsibility and factoring in prior-authorization and medical necessity, identifying patients’ financial clearance or propensity to pay, and providing consumers a clear explanation of their financial policies—along with a detailed, reliable estimate of their out-of-pocket expenses—as early in the revenue cycle as possible.
At DarkDaily.com, readers can access free resources on a variety of topics tailored specifically to the needs of laboratory administrators, lab managers, pathologists, and lab industry consultants.
US hospitals typically spend $2,424/day to provide inpatient care, according to the KFF report
How much does the average hospital spend/day to provide inpatient care? The numbers vary widely, but the latest statistics from Kaiser Family Foundation (KFF) State Health Facts show West Coast states incur the highest daily operating and non-operating inpatient costs.
This disparity in spending is unlikely to surprise medical laboratory executives working in hospital settings. They know firsthand that operating costs can vary from state-to-state and by hospital ownership type.
Oregon, California, and Washington are the most expensive
three states overall for inpatient hospital care. However, the leaderboard
changes when looking specifically at inpatient care at for-profit hospitals.
In the for-profit hospital category:
North Dakota, South Dakota, and Alaska rack up
the highest expenses/day.
Idaho, California, and Oregon top the non-profit
hospital segment.
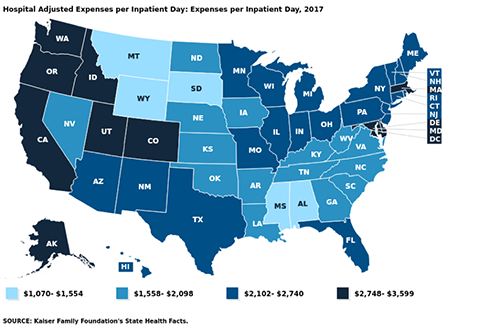
Overall in the US, the average hospital incurs expenses of
$2,424/inpatient day, the KFF reports.
While the average US hospital spends $2,424/day to deliver inpatient care, West Coast states have the highest hospital adjusted operating and non-operating expenses/inpatient day, according to a recent report from the Kaiser Family Foundation. Oregon hospitals top the spending list at $3,599/day. (Graphic copyright: Kaiser Family Foundation.)
AMA Annual Survey
Rankings
Rankings are based on information from the 1999-2017 American Hospital
Association Annual Survey, which includes all operating and non-operating
expenses for registered US community hospitals. The figures are an estimate of
the expenses incurred by a hospital to provide a day of inpatient care. They
have been adjusted higher to reflect an estimate of the volume of outpatient
services, according to the KFF. The numbers do not reflect actual charges or
reimbursement for the care provided.
Most expensive average expenses/inpatient day:
Oregon, $3,599
California, $3,441
Washington, $3,429
Idaho, $3,119
District of Columbia, $3,053
Least expensive average expenses/inpatient day:
Montana, $1,070
Mississippi, $1,349
South Dakota, $1,505
Wyoming, $1,520
Alabama, $1,554
Most expensive non-profit hospitals/inpatient day:
Idaho, $4,208
California, $3,800
Oregon, $3,546
Washington, $3,500
Colorado, $3,319
Least expensive non-profit hospitals/inpatient day:
Mississippi, $1,365
South Dakota, $1,519
Iowa, $1,564
Montana, $1,627
Alabama, $1,723
Most expensive for-profit hospitals/inpatient day:
North Dakota, $4,701
South Dakota, $3,956
Alaska, $3,280
Nebraska, $3,031
Wisconsin, $2,830
Least expensive for-profit hospitals/inpatient day:
Maine, $1,055
Maryland, $1,207
West Virginia, $1,362
Iowa, $1,558
Arkansas, $1,619
Most expensive state/local government hospitals/inpatient
day:
Oregon, $4,062
Connecticut, $3,979
Washington, $3,312
California, $3,217
Utah, $3,038
Least expensive state/local government hospitals/inpatient
day:
Montana, $52
South Dakota, $442
Pennsylvania, $787
Nebraska, $906
Georgia, $917
Some Regions Pay Much
More for Healthcare
The KFF report did not look at whether patients in states
where hospitals incur the highest daily operating and non-operating expenses
also pay the most for hospital services. Hospital charges vary widely, with
many treatments costing far more in some regions than others.
In addition, health bills can vary at different hospitals in
the same city or region. According to Healthcare.gov,
the average total cost of a three-day hospital stay is about $30,000.
Adding to the confusion is the fact that hospital costs,
billed charges, and the amounts paid by patients for services can be distinctly
different amounts. Health insurance companies, for example, negotiate lower
rates with hospitals and health systems for their plan enrollees. While patients
without insurance are billed full price for services based on the hospital’s chargemaster.
Zack Cooper, PhD, Associate Professor of Health Policy and Economics at Yale University, told National Public Radio (NPR) that hospital consolidation is partly to blame for the wide variation in the price of hospital services within states and across the country. He says consolidation has eliminated competition in many markets. “Where one large hospital dominates the markets, that hospital is able to get higher prices,” Cooper maintains. “Hospitals have gotten increasingly powerful over time.” (Photo copyright: Yale University.)
CMS Final Rule
Requires Pricing Transparency
As of Jan. 1, 2019, a new Centers for Medicare and Medicaid Services (CMS) rule went into effect aimed at making hospital pricing more transparent. The CMS is now requiring hospitals to publish chargemaster price lists online, rather than release those numbers to patients upon request.
However, healthcare advocates have questioned the rule’s
impact on transparency. Posted hospital pricing information is often hard to
access and difficult to comprehend. In addition, chargemaster prices typically
do not represent the actual costs passed on to consumers.
“[The chargemaster] is the list price. When you go to buy a car, you have a manufacturer’s suggested retail price. This is basically what [the chargemaster] is,” Medical Contributor Natalie Azar, MD, told NBC News.
“Prevention comes first,” Nechrebecki suggests. “Utilize the
ambulatory care clinics. Go see your doctors and do what they recommend to keep
yourself healthy. Eat well and exercise often. You will prevent many surgeries
and hospitalizations.”
Sound advice. Nevertheless, clinical laboratories and anatomic pathology groups should take note of the federal government’s ongoing push for price transparency and prepare accordingly.