Good behavior in federal prison by the disgraced founder of the now-defunct clinical laboratory company earned her the reduction in her original sentence of 11 years
Elizabeth Holmes, founder of failed clinical laboratory blood analysis company Theranos, continues to serve a lengthy term in prison after being convicted of multiple counts of fraud in 2022. However, now comes news that good behavior at her federal prison has shortened her sentence by nearly two years, according to NBC News.
The latest reduction took Holmes’ release from December 2032 to August 2032 in her “11-plus-year (135 month) prison sentence for wire fraud and conspiracy,” NBC reported, adding that Holmes, though Theranos, “defrauded investors out of hundreds of millions of dollars.”
Holmes entered FPC Bryan, a federal prison camp in Bryan, Texas, to begin serving her term in May 2023.
“Holmes had her sentence computation done within the first 30 days of arriving at Bryan,” Forbes reported. Given Good Conduct Time (GCT), Holmes was given 608 days off calculated from the start of her sentence. “If she were to incur a disciplinary infraction, some of those days can be taken away. Most all prisoners receive 54 days per year of GCT based on the sentence imposed,” Forbes added.
The Federal Bureau of Prisons (BOP) can additionally shave off up to a year through its Residential Drug Abuse Program (RDAP). “To qualify, the prisoner must not have a disqualifying offense, such as terrorism or gun charge, and voluntarily provided information that they had a drug or alcohol problem prior to their arrest. This disclosure has to be done prior to sentencing during the pre-sentence interview and must be also documented in the Presentence Report, a detailed report used by the BOP to determine things like classification and programming for the prisoner,” Forbes noted.
Additionally, the federal First Step Act, which President Trump signed into law in 2018, enables Holmes to “earn up to 365 days off any imposed sentence by participating in prison programming such as a self-improvement classes, a job, or religious activities,” Forbes reported.
Given the opportunities to shave time off her sentence, Holmes may ultimately serve just 66 months of her original 135 month sentence in federal prison.
Elizabeth Holmes (above) taken backstage at TechCrunch Disrupt San Francisco 2014 when Holmes was at the height of her fame and popularity. At this point, Theranos’ Edison blood testing device had not yet been shown to be a fake. But evidence was mounting as clinical laboratory scientists and anatomic pathologists became aware of the technology’s shortcomings. (Photo copyright: Max Morse/Wikimedia Commons.)
Fall of a Silicon Valley Darling
Theranos boasted breakthrough technology and became an almost overnight sensation in Silicon Valley when it burst onto the scene in 2003. Holmes, a then 19-year-old Stanford University dropout, claimed Theranos would “revolutionize the world of blood testing by reducing sample sizes to a single pin prick,” Quartz reported.
The height of the company saw Theranos valued at $9 billion, which came crashing down when the Wall Street Journal reported in 2015 that questionable accuracy and procedures were being followed by the company, CNN reported.
“From the moment Holmes concluded her presentation and stepped off the podium on Monday afternoon, she, her company, and her comments became the number one subject discussed by attendees in the halls between sessions and in the AACC exhibit hall,” Michel wrote, adding, “The executive team and the investors at Theranos have burned through their credibility with the media, the medical laboratory profession, and the public. In the future, the company’s claims will only be accepted if presented with scientific data developed according to accepted standards and reviewed by credible third parties. Much of this data also needs to be published in peer-reviewed medical journals held in highest esteem.”
Ultimately, investors who had jumped in early with financial support for Theranos were defrauded of hundreds of millions of dollars and Holmes was sentenced to 11 years/three months behind bars.
“Theranos had only ever performed roughly a dozen of the hundreds of tests it offered using its proprietary technology, and with questionable accuracy. It also came to light that Theranos was relying on third-party manufactured devices from traditional blood testing companies rather than its own technology,” CNN added.
The company shut down in 2018.
And so, the Elizabeth Holmes saga continues with reductions in her prison sentence for “good behavior.” The irony will likely not be lost on the anatomic pathologists, clinical laboratory scientists, and lab managers who followed the federal trials.
Clinical studies show that new ‘cell-free’ test can predict cardiovascular disease risk better than standard HDL cholesterol test
Researchers from the National Institutes of Health (NIH) have developed a diagnostic assay that measures how well high-density lipoprotein (HDL)—the so-called “good” cholesterol—is working in the body. And their findings could lead to new clinical laboratory tests that supplement standard HDL level testing to better determine a person’s risk for heart disease.
Cholesterol tests are among the most commonly performed assays by clinical laboratories. A new test that reveals how well HDL is working in the body would certainly boost a medical laboratory’s test requisition volume.
“Measuring HDL function is limited to research labs and isn’t conducive to large-scale testing by routine clinical laboratories. To try to solve that problem, researchers from NHLBI’s Lipoprotein Metabolism Laboratory created a new diagnostic test,” noted an NHLBI news release.
“This is going to quicken the pace of basic research,” said Edward B. Neufeld, PhD, who along with guest researcher Masaki Sato, PhD, developed the test. “It increases the number of samples that you can study. It increases the number of experiments you can do.”
Such a new cholesterol test would quickly become one of the most commonly performed clinical lab tests because just about every American who has a physical gets cholesterol tests as part of that process.
“Other people may modify this or come up with better versions, which is fine with us,” Edward Neufeld, PhD (above), NHLBI Staff Scientist, said in a news release. “We just really wanted to tackle this problem of evaluating HDL function.” Clinical laboratories may soon have a new cholesterol test to supplement standard HDL level testing. (Photo copyright: ResearchGate.)
Faster Answers Needed about HDL
According to the NIH, the goal should go beyond measuring level of HDL as part of a person’s annual physical. What is also needed is finding out whether HDL cholesterol is effectively doing certain tasks, such as removing extra cholesterol from arteries and transporting it to the liver.
The NHLBI’s new cell-free test may make it possible to step up large-scale clinical testing of HDL function, according to the news release. As it stands now, HDL function study has been limited to research labs where testing involves “harvesting cells in the lab [which] can take days to process,” according to NIH Record.
“Most studies to date that have assessed CAD (coronary artery disease) risk by HDL functionality still use the CEC (cellular cholesterol efflux capacity) in vitro assay and are based on the use of radioisotopes (3H-cholesterol) and cultured cells, which is very labor intensive and impractical to do in a clinical laboratory,” the researchers wrote in The Journal of Clinical Investigation. They also pointed out that CEC batch-to-batch variability does not fit clinical laboratories’ need for standardization.
Advantages of NHLBI’s Test
To overcome these barriers, the NHLBI researchers created an HDL-specific phospholipid efflux (HDL-SPE) assay that has certain advantages over current HDL function assessments done in research labs.
According to the NIH, the HDP-SPE assay:
Is easy to replicate in clinical labs.
Is more suited to automation and large samples.
Offers up results in about an hour.
Is a better predictor of cardiovascular disease risk than HDL cholesterol testing for CAD risk.
“We developed a cell-free, HDL-specific phospholipid efflux assay for the assessment of CAD risk on the basis of HDL functionality in whole plasma or serum. One of the main advantages of the HDL-SPE assay is that it can be readily automated, unlike the various CEC assays currently in use,” the authors noted in their paper.
Here is how the test is performed, according to the NIH:
Plasma with HDL is separated from the patient’s blood.
“Plasma is added to donor particles coated with a lipid mixture resembling plaque and a fluorescent-tagged phospholipid” that only HDL can remove.
The fluorescent signal by HDL is then measured.
A bright signal suggests optimal HDL lipid removal function, while a dim light means reduced function.
The test builds on the scientists’ previous findings and data. In creating the new assay they drew on data from:
A study of 50 severe CAD and 50 non-CAD people.
A Japanese study of 70 CAD and 154 non-CAD participants.
Examined association of HDL-SPE with cardiovascular disease in a study of 340 patients and 340 controls.
“We have established the HDL-SPE assay for assessment of the functional ability of HDL to efflux phospholipids. Our combined data consistently show that our relatively simple HDL-SPE assay captures a pathophysiologically relevant parameter of HDL function that is at least equivalent to the CEC assay in its association with prevalent and incident CAD,” the researchers concluded in The Journal of Clinical Investigation.
Test May Be Subject to New FDA Rule
While HDL cardiovascular-related research is moving forward, studies aimed at the therapeutic side need to pick up, NIH noted.
“Someday we may have a drug that modulates HDL and turns out to be beneficial, but right now we don’t have that,” said Alan Remaley MD, PhD, NHLBI Senior Investigator and Head of the Lipoprotein Metabolism Laboratory, in the news release.
It may be years before the HDL-SPE test is used in medical settings, the researchers acknowledged, adding that more studies are needed with inclusion of different ethnicities.
Additionally, in light of the recently released US Food and Drug Administration (FDA) final rule on regulation of laboratory developed tests (LDT), the company licensed to bring the test to market may need to submit the HDL-SPE assay to the FDA for premarket review and clearance. That could lengthen the time required for the developers to comply with the FDA before the test is used by doctors and clinical laboratories in patient care.
Clinical laboratory managers should prepare for an increase in demand for measles testing, especially for children
Clinical laboratory managers should be on the alert for new cases of measles. The US Centers for Disease Control and Prevention (CDC) has reported a surge in the highly infectious disease. Public health experts pointed to declining vaccination coverage as the primary cause. Officials in other countries have also reported outbreaks.
In 2000, the US declared that measles had been eliminated, meaning it “is no longer constantly present in this country,” the CDC stated on its website. However, the agency noted travelers can still bring the disease into the country and that there have been sporadic outbreaks since then.
In a new study, published April 11, 2024, in the CDC’s Morbidity and Mortality Weekly Report (MMWR), the agency reported that it was notified of 97 confirmed cases in the first quarter of 2024. That compares to an average of five cases during the first quarters of 2020 through 2023, the agency stated. In total, 338 cases were reported to the CDC between Jan. 1, 2020, and March 28, 2024, so the latest outbreaks amount to 29%—nearly a third—of the total.
“While the risk for measles for the majority of the US population still remains low, it’s crucial that we take the necessary steps now to prevent the continued spread of measles and maintain elimination in the US,” Adria D. Mathis, MSPH, lead author of the CDC report, told Healthline. Mathis is affiliated with the CDC’s Division of Viral Diseases at the National Center for Immunization and Respiratory Diseases (NCIRD).
“We have seen, in the region, not only a 30-fold increase in measles cases, but also nearly 21,000 hospitalizations and five measles-related deaths. This is concerning,” Hans Henri P. Kluge, MD (above), WHO Regional Director for Europe, told BBC News. “Vaccination is the only way to protect children from this potentially dangerous disease.” Clinical laboratories in the US that identify a case of measles from a positive test must report that result to public health labs. Thus, wise lab managers will track the rise in measles cases and prepare for increased demand for measles testing. (Photo copyright: World Health Organization.)
Renewed Threat to the US, Other Countries
The recent cases “represent a renewed threat to the US elimination status,” and “underscore the need for additional efforts to increase measles, mumps, and rubella (MMR) vaccination coverage, especially among close-knit and under-vaccinated communities,” Mathis told Healthline.
The MMWR report notes that most of the new cases were in persons under age 20, and that almost all were “in persons who were unvaccinated or whose vaccination status was unknown.” Most of the importations, the report states, were “among persons traveling to and from countries in the Eastern Mediterranean and African WHO [World Health Organization] regions; these regions experienced the highest reported measles incidence among all WHO regions during 2021–2022.”
In the US, vaccination coverage has been below 95% for three consecutive years. That is the “estimated population-level immunity necessary to prevent sustained measles transmission,” according to the federal agency. In 12 states and the District of Columbia, the coverage rate is below 90%. In total, “approximately 250,000 kindergarten children [are] susceptible to measles each year,” the CDC report states.
Measles vaccination coverage has declined globally, “from 86% in 2019 to 83% in 2022.” This left nearly 22 million children under the age of one susceptible to the disease, the report notes.
Earlier Measles Outbreaks in the US
The CDC performed its latest analysis following two larger measles outbreaks in 2019 among under-vaccinated populations in New York state.
The Associated Press (AP) reported that the 2019 epidemic, which totaled 1,274 cases nationwide, “was the worst in almost three decades and threatened the United States’ status as a country that has eliminated measles by stopping the continual spread of the measles virus.”
A vaccine for the disease first became available in 1963. Prior to its availability, “there were some three million to four million cases per year,” AP reported. Most people recover, but “in the decade before the vaccine was available, 48,000 people were hospitalized per year. … About 1,000 people developed dangerous brain inflammation from measles each year, and 400 to 500 died,” AP noted, citing CDC data.
US Not Alone in Fight against Measles
Other countries also are reporting spikes in measles cases. In a recently published rapid risk assessment, the Canadian government reported a total of 29 cases as of March 15, 2024, of which 21 were reported since Feb. 28.
“That’s already the largest annual total since 2019 and more than double the number of cases reported last year, as medical experts fear the number will rise while more Canadians travel in and out of the country this month for March break,” CBC News reported.
“New projections from a team at Simon Fraser University (SFU) in British Columbia show the grim possibilities,” CBC News reported. “The modelling suggests that vaccine coverage of less than 85% can lead to dozens of cases within small communities—or even hundreds if immunization rates are lower.”
Numbers are far worse in parts of Europe. In a February 2024 news release, the World Health Organization reported that in 2023, more than 58,000 people in its European region were infected by the disease, “resulting in thousands of hospitalizations and 10 measles-related deaths.”
According to WHO epidemiological data, countries in Central Asia, which is part of WHO’s European region, reported some of the highest numbers:
15,111 in Kazakhstan,
13,735 in Azerbaijan, and
7,044 in Kyrgyzstan.
The Russian Federation reported 12,723 cases and Turkey reported 4,559.
A WHO European Region Measles and Rubella Monthly Update notes that more than half of the regionwide cases—31,428—were reported in the last three months of 2023. More than 15,000 cases were reported in December. That compares to just 163 cases reported in 2021 and 942 in 2022. Nearly half of the cases were among children under the age of five.
Lack of Vaccinations among Children Blamed for Outbreaks
One factor that has led to the increase in measles cases was the disruption to immunization services caused by the COVID-19 pandemic. “This has resulted in a significant accumulation of susceptible children who have missed their routine vaccinations against measles and other vaccine-preventable diseases,” the WHO reported.
Among the region’s 53 member states, 33 had eliminated measles, WHO reported, but “this achievement remains fragile. To retain this status, a country must ensure that transmission of the virus following any importation is stopped within 12 months from the first reported case.”
In the UK, which reported 231 cases last year, the National Health Service has launched a campaign to improve vaccination rates, the BBC reported, noting that “more than 3.4 million children aged under 16 are unprotected and at risk of becoming ill.”
However, a public health campaign built on vaccination is successful only if a high rate of individuals get vaccinated. The Baby Boomer and Gen X generations had high rates of vaccination for smallpox, polio, etc. because the parents saw individuals in their family and neighborhood who became infected and suffered lifechanging consequences. They recognized that vaccination was a simple thing to provide protection from a potentially deadly infection.
Clinical laboratory managers and pathologists will want to follow the CDC’s ongoing reports of the number of cases of measles in this country. Today, the absolute number of new measles cases is relatively small. At the same time, in communities experiencing an outbreak of even a few measles cases, physicians may want to increase the volume of measles tests they order for their patients.
Drone company Zipline delivers medical supplies and clinical laboratory specimens on four continents and is used in the US by several major healthcare networks and retail organizations
Unmanned aerial vehicles (UAVs), commonly referred to as drones, continue to demonstrate their value in the medical industry. In February, WellSpan Health announced it will soon begin using drones to deliver prescriptions to patients and to transport medical supplies and clinical laboratory specimens between its facilities located in Pennsylvania.
WellSpan Health, one of the leading healthcare systems in Southern Pennsylvania and Northern Maryland, is partnering with Zipline, a supplier of drone logistic services, in the endeavor.
“We’re making our [healthcare] system lower cost, faster, and more sustainable by bringing this exceptional technology to South Central Pennsylvania,” said Roxanna Gapstur, PhD, RN, President and CEO, WellSpan Health, in a news release. “We know the easier it is to access care the healthier people can be. With Zipline, we’re connecting healthcare straight to your front door.”
Zipline’s Platform 2 (P2 Zip) drone will be used for the venture. The drone is designed to fly in almost all weather conditions. If true, this would be a boon to the drone delivery service industry.
Previous attempts to implement drone delivery services have been hampered by a typical drone’s low performance in bad weather such as heavy rain and high winds. This seems to be what has held back wide adoption of drone delivery in the US.
“WellSpan continues to reimagine what healthcare can look like for our patients. With Zipline, we’re creating a future for our patients, where getting a prescription filled is as simple as pressing a button,” said Roxanna Gapstur, PhD, RN (above), President and CEO, WellSpan Health, in a news release. WellSpan Health’s drone delivery customers will be able to receive text notifications tracking the progress of their medical supplies and clinical laboratory specimens on their smartphones. (Photo copyright: WellSpan Health.)
Delivery of Medical Supplies Direct to Patients’ Front Door
ABC27 reported that “WellSpan will be the first health service in the state of Pennsylvania that will introduce this type of technology and delivery system.”
According to the drone company’s website, Zipline:
Serves more than 4,000 health centers worldwide and more than 45 million people.
Has completed more than one million deliveries.
Plans to operate more flights annually than almost all the major US airlines by next year.
Delivers 75% of Rwanda’s blood supply outside Kigali, the country’s capital city.
Additionally, Zipline’s all-electric, zero-emission drones reduce carbon emissions by an average of 97% when compared to gas-driven vehicles.
Each P2 Zip drone features Zipline’s autonomous airspace Detect and Avoid (DAA) deconfliction technology and contains fully redundant flight systems.
“This acoustic system is composed of a series of small, lightweight acoustic microphones and onboard processors used to navigate airspace and grant 360-degree awareness with a range of up to 2,000 meters,” DRONELIFE reported. “This innovative onboard system enables the aircraft to autonomously detect and maneuver around other aircraft and obstacles in real-time, making large scale autonomous commercial operations more feasible.”
According to a fact sheet, the P2 Zip drone can carry loads up to eight pounds and has a cruising speed of 70 miles/hour. It’s service range is either a 10-mile radius or a one-way trip of 24 miles. It only requires two feet of open space to execute a delivery and can hover at more than 300 feet above the ground while delivering a package.
“Zipline has been improving access to healthcare for eight years. Together with WellSpan Health we will bring prescriptions and medical products right to patients’ doorsteps with fast, sustainable, and convenient delivery,” stated Keller Rinaudo Cliffton, co-founder and CEO of Zipline, in the news release.
Other Healthcare Drone Delivery Services
Dark Daily has published many ebriefs about drones being used for medical supply and clinical laboratory specimen deliveries.
As drone delivery technology continues to improve, UAVs are more likely to be used in healthcare situations. If the issue of bad weather has been resolved, it’s reasonable to assume that within a short period of time clinical laboratories may begin receiving many more samples to test via drones.
Lack of regular clinical laboratory screenings in this age group at least partially to blame, researchers say
While cervical cancer rates have seen a 50-year decline overall, that trend is shifting among 30- to 40 year-olds who have experienced a near 2% increase from 2012-2019. This finding comes from a 2024 American Cancer Society (ACS) report that is eyeing the timeline of the human papillomavirus (HPV) vaccines and the lack of clinical laboratory cancer screenings as possible contributors to this new trend.
Though a 2% increase is significant, the study, which was published in CA: ACancer Journal for Clinicians, titled “Cancer Statistics, 2024,” noted that these cancers were “mostly early, curable tumors,” epidemiologist Ahmedin Jemal DVM, PhD, Senior Vice President Surveillance and Health Equity Science at ACS, and senior author of the new report, told NBC News.
To understand how the increase in cancer rates impacts this age group, consider the numbers: “About 13,800 American women are diagnosed with cervical cancer each year and 4,360 die from the disease,” NBC reported.
US vaccination programs for youths have lagged behind nations that have embraced HPV vaccination to positive results.
Australia, for example, has vaccinated a high proportion of its youth since the vaccine was first released in 2006. In 2023, the nation created its National Strategy for the Elimination of Cervical Cancer in Australia program and expects cervical cancer to be fully eliminated there by 2035.
For lab professionals, this demonstrates how new technologies like the HPV test and vaccine can alter how individuals are screened for diseases, and how vaccines can reduce and even eliminate diseases that were once common.
“We need to make sure we are not forgetting about that generation that was a little too old for HPV vaccination,” Jennifer Spencer, PhD (above), Assistant Professor, Department of Population Health and Department Internal Medicine, Dell Medical School, University of Texas at Austin, told NBC News. “The onus is on the healthcare system to think about who is slipping through the cracks,” she added. Lack of clinical laboratory screenings among the 30-40 age group may be contributing to the increase in cervical cancer rates. (Photo copyright: Dell Medical School.)
Lack of Clinical Laboratory Screenings
Research points to a lag in cervical cancer screenings as a possible cause for the recent rise in cases. Timely screening allows doctors to both identify and remove any worrisome lesions before they become cancerous, Jennifer Spencer, PhD, Assistant Professor of the Department of Population Health, Dell Medical School, University of Texas at Austin, told NBC News.
Screenings for women ages 21-65 have fallen 15% since 2000, according to data from the National Cancer Institute. Also, more than half of women with cervical cancer have “either never been screened or haven’t been screened in the past five years, according to the Centers for Disease Control and Prevention,” NBC reported.
The US Preventative Services Task Force recommends that women 21-29 years of age should receive Pap smears every three years. Women 30-65 years of age should do the same, or every five years with an HPV test or combo test.
Despite a decrease in cervical cancer, 29% of women in their 20s are overdue to get screening, NBC noted. This was the age group most likely to be lagging on getting screened. Spencer says that this delay in screening could explain the resulting increase in cervical cancer among the 30-40 age group.
Causes for Lack in Screenings
Regardless of age group, women who were uninsured, in a rural area, non-white, or identifying as lesbian, bisexual, or gay were also more likely to be overdue on screenings, according to Spencer’s study.
In addition, women who just moved to the United States may have missed their screenings, thus increasing risk, epidemiologist Nicholas Wentzensen, MD, PhD, Deputy Director, Senior Investigator, and Head of the Clinical Epidemiology Unit at the National Cancer Institute, told NBCNews.
Additionally, Spencer found in her research that confusion exists by both patients and doctors on when cervical screening should take place. Some participants in her study did not have screening recommended by their doctors, while others simply did not recognize it was necessary.
“When women in one of Spencer’s studies were asked why they hadn’t been screened recently, they commonly said that they didn’t know they needed to be screened or that a health provider hadn’t recommended it. Only 1% [of] women ages 21 to 29 said they had skipped screening because they had received the HPV shot,” NBC News reported.
A 2022 Journal of American Medicine (JAMA) report also looked at screenings as a possible cause. Those researchers found that “only 73% of women with abnormal screening results received follow-up care,” NBC reported.
“If the increase (in cases) is real, it could be a result of missed screening opportunities at earlier ages, as suggested by the increase in squamous cell carcinoma and localized disease. It may also stem from a decrease in screening at younger ages,” the JAMA study authors wrote.
HPV Vaccine and Cervical Cancer Prevention
The HPV vaccine is another important area of research to be considered. Approved in 2006, HPV vaccines were beneficial because HPV “causes six types of cancer, including cervical cancer,” NBC reported.
Women in their early 20s at that time were the first generation to benefit from HPV vaccines, NBC noted. It may be that they continue to benefit in a decrease in cervical cancer among their cohort.
Countries that have emphasized HPV vaccines and stringent screenings in their cancer prevention efforts are reaping the benefits of that policy.
Though cancer screening and the HPV vaccine are important first steps women should take to prevent cervical cancer, follow-through clinical laboratory testing and diagnosis is crucial, Spencer added. This would include additional testing and treatment for any abnormal results of the cancer screening.
However, according to Spencer, “only 73% of women with abnormal screening results received follow-up care,” NBC reported.
Healthcare policymakers today are emphasizing the need for providers to identify and close gaps in care as a way to improve patient outcomes and help control the cost of care. Women who are overdue for a cervical cancer screening test—whether an HPV test or Pap smear—have this care gap. This creates an opportunity for clinical labs to add value.
Clinical laboratories could be helpful during this period by looking at patient files to note which patients are overdue for screenings and then alerting their doctors. Medical labs also could work directly with doctors to establish a program to reach out to patients. Labs would thus be adding value as well as benefitting patients.
This may be a new ‘sign of the times’ as hospitals, clinical laboratories, and other healthcare providers working with AI find they also need to hire their own prompt engineers
AI “prompting,” according to Florida State University, “refers to the process of interacting with an AI system by providing specific instructions or queries to achieve a desired outcome.”
According to workable.com, prompt engineers specialize “in developing, refining, and optimizing AI-generated text prompts to ensure they are accurate, engaging, and relevant for various applications. They also collaborate with different teams to improve the prompt generation process and overall AI system performance.”
Healthcare institutions are getting more serious about using AI to improve daily workflows and clinical care, including in the clinical laboratory and pathology departments. But adopting the new technology can be disruptive. To ensure the implementation goes smoothly, hospitals are now seeking prompt engineers to guide the organization’s strategy for using AI.
When Boston Children’s Hospital leaders set out to find such a person, they looked for an individual who had “a clinical background [and] who knows how to use these tools. Someone who had experience coding for large language models and natural language processing, but who could also understand clinical language,” according to MedPage Today.
“We got many, many applications, some really impressive people, but we were looking for a specific set of skills and background,” John Brownstein, PhD, Chief Innovation Officer at Boston Children’s Hospital and Professor of Biomedical Informatics at Harvard Medical School, told MedPage Today.
“It was not easy to find [someone]—a bit of a unicorn-type candidate,” noted Brownstein, who is also a medical contributor to ABC News.
After a four-month search, the hospital hired Dinesh Rai, MD, emergency room physician and AI engineer, for the position. According to Brownstein, Rai had “actually practiced medicine, lived in a clinical environment,” and had “successfully launched many [AI] applications on top of large language models,” MedPage Today reported.
“Some of the nuances I bring to the table in terms of being a physician and having worked clinically and understanding really deeply the clinical workflows and how we can implement the [AI] technology—where its limits are, where it can excel, and the quickest way to get things [done],” Dinesh Rai, MD (above), told MedPage Today. “I’m happy to be able to help with all of that.” Hospital clinical laboratory and pathology managers may soon by engaging with prompt engineers to ensure the smooth use of AI in their departments. (Photo copyright: LinkedIn.)
Prompt Engineers are like F1 Drivers
“It’s kind of like driving a car, where basically anyone can drive an automatic car, and anyone can go onto ChatGPT, write some text, and get a pretty solid response,” said Rai, describing the act of AI prompting to MedPage today.
Then, there are “people who know how to drive manual, and there are people who will know different prompting techniques, like chain-of-thought or zero-shot prompting,” he added. “Then you have those F1 drivers who are very intimate with the mechanics of their car, and how to use it most optimally.”
The American Hospital Association (AHA) believes that AI “holds great promise in helping healthcare providers gain insights and improve health outcomes.” In an article titled, “How AI Is Improving Diagnostics, Decision-Making and Care,” the AHA noted that, “Although many questions remain regarding its safety, regulation, and impact, the use of AI in clinical care is no longer in its infancy and is expected to experience exponential growth in the coming years.
“AI is improving data processing, identifying patterns, and generating insights that otherwise might elude discovery from a physician’s manual effort. The next five years will be critical for hospitals and health systems to build the infrastructure needed to support AI technology, according to the recently released Futurescan 2023,” the AHA wrote.
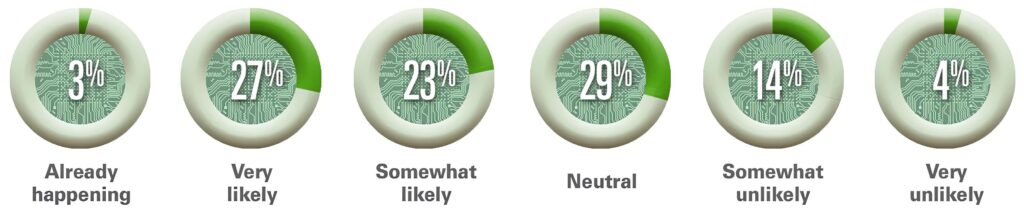
The graphic above is taken from the American Hospital Association’s article about Futurescan’s 2023 survey results on AI in healthcare. “Healthcare executives from across the nation were asked how likely it is that by 2028 a federal regulatory body will determine that Al for clinical care delivery augmentation (e.g., assisted diagnosis and prescription, personalized medication and care) is safe for use by our hospital or health systems,” AHA stated. This would include the use of AI in clinical laboratories and pathology group practices. (Graphic copyright: American Hospital Association.)
The AHA listed the top three opportunities for AI in clinical care as:
Clinical Decision Tools: “AI algorithms analyze a vast amount of patient data to assist medical professionals in making more informed decisions about care.”
Diagnostic and Imaging: The use of AI “allows healthcare professionals to structure, index, and leverage diagnostic and imaging data for more accurate diagnoses.”
Patient Safety: The use of AI improves decision making and optimizes health outcomes by evaluating patient data. “Systems that incorporate AI can improve error detection, stratify patients, and manage drug delivery.”
The hiring of a prompt engineer by Boston Children’s Hospital is another example of how AI is gaining traction in clinical healthcare. According to the Futurescan 2023 survey, nearly half of hospital CEOs and strategy leaders believe that health systems will have the infrastructure in place by 2028 to successfully utilize AI in clinical decision making.
“I’m lucky to [be] in an organization that has recognized the importance of AI as part of the future practice of medicine,” Rai told MedPage Today.
Pathologists and managers of clinical laboratories and genetic testing companies will want to track further advancements in artificial intelligence. At some point, the capabilities of future generations of AI solutions may encourage labs to hire their own prompt engineers.