Mobile, wearable, mHealth monitoring devices are a key element of many employer fitness programs and clinical laboratories can play an important role in their success
For years Dark Daily has encouraged clinical laboratories to get involved in corporate wellness programs as a way to support their local communities and increase revenues. Now, leveraging the popularity of mobile health (mHealth) wearable devices, UnitedHealthcare (UHC) has found a new way to incentivize employees participating in the insurer’s Motion walking program. UHC is offering free Apple Watches to employees willing to meet or exceed certain fitness goals.
This is the latest wrinkle in a well-established trend of incentivizing
beneficiaries to meet healthcare goals, such as stopping smoking, losing
weight, reducing cholesterol, and lowering blood pressure.
It’s an intriguing gamble by UHC and presents another opportunity for medical laboratories that are equipped to monitor and validate participants’ progress and physical conditions.
How to Get a Free Apple
Watch and FIT at the Same Time
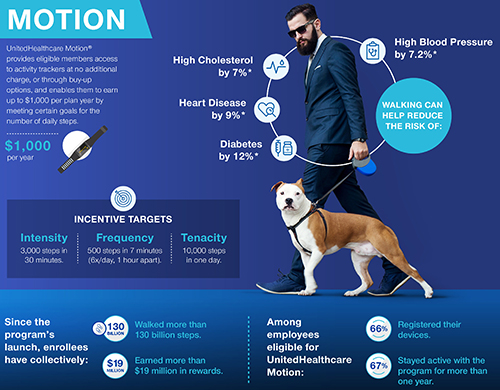
CNBC reported that UHC’s Motion program participants number in the hundreds of thousands. And, according to a UHC news release, they can earn cash rewards up to $1,000 per year. The idea is that participants pay off the cost of their “free” Apple Watch one day at a time by achieving activity goals set in UHC’s FIT tracking method. Those goals include:
Frequency:
500 steps in seven minutes; six times a day, at least one hour apart;
Intensity:
3,000 steps in 30 minutes; and,
Tenacity:
10,000 steps in one day.
“UnitedHealthcare Motion is part of our consumer-focused strategy that is driving toward a simple, integrated, mobile-centric ecosystem that delivers value to consumers,” said Steve Nelson, CEO of UnitedHealthcare, in a news release. “Smartwatches and activity trackers stand alongside transparency in physician selection and medical costs, easy virtual visits with healthcare professionals, and digital coaching and online wellness programs, all of which are designed to support consumers in enhancing their health and improving how they navigate the healthcare system.” Clinical laboratories play a key role in this healthcare strategy. (Graphic copyright: UnitedHealthcare.)
Though hundreds of thousands of beneficiaries are eligible to participate in UHC’s Motion program through their employers, only 45% of those eligible have enrolled in Motion, Fox Business reported.
UHC hopes the offer of a free Apple Watch (which has
applications to track minutes of exercise, a heart rate monitor, and more) will
encourage people to sign up and then progress toward the Motion program’s FIT
goals.
As people meet these goals, they earn $4/day toward the cost
of the Apple Watch. Participants, who do not take enough steps in a six-month period
could be required to repay a percentage of the cost of the smartwatch.
Motion participants who already own an Apple Watch can still
earn up to $1,000 per year in cash rewards for achieving the FIT goals.
“UnitedHealthcare Motion’s success affirms that wearables can play an important role in helping people enhance their well-being and supporting and motivating them to stay engaged in their health,” said Rebecca Madsen, Chief Consumer Officer of UnitedHealthcare, in the UHC news release. (Photo copyright: University of Pennsylvania.)
Impact of mHealth
Programs/Technology Not Clear
Chronic diseases, including diabetes and heart disease, annually cost the US healthcare system $190 billion and employers $126 billion in lost productivity, according to the Centers for Disease Control and Prevention (CDC).
However, some researchers say it’s too early for mHealth
wearables, medication apps, physician virtual engagement, and other digital tools
(many launched within the past five to seven years) to effect key indicators,
such as obesity, life expectancy, and smoking cessation.
“Some of the benefits of these new tools won’t be realized for a long time. It’s really hard to tease out the impact of digital health. Maybe we’re helping people, but we’re not detecting it,” James Murphy, MD, Associate Professor, University of California San Diego Health and radiation oncologist, told CNBC.
Nevertheless, it behooves medical laboratories to develop
procedures for analyzing and reporting data that could impact people who use
wearable mHealth devices to participate in employer wellness programs.
For example, labs could contact insurance companies with
information about biomarkers that provide views into an individual’s progress
toward personal health goals.
Data-driven recommendations from medical laboratories about
tests for chronic conditions such as heart disease and diabetes will likely be
welcomed by payers.
Medicare officials are including most hospital laboratories in this PAMA data reporting cycle, but hospitals face $10,000/day federal penalties for not filing, filing late, or filing incomplete or inaccurate data
Clinical laboratories operated by hospitals and health systems could prove to be a game changer for the lab industry in this upcoming PAMA private payer lab test price reporting cycle. But that upside comes with risk.
For this reporting period, the federal Centers for Medicare and Medicaid Services (CMS) has defined any hospital laboratory that uses the CMS 1450 14X to bill for Medicare Part B clinical laboratory tests as an “applicable laboratory” under the Protecting Access to Medicare Act of 2014 (PAMA). That means a majority of hospital labs in the United States are required to report the prices they were paid by private health insurers to CMS.
This makes the current PAMA reporting period a high-stakes
endeavor, because unprepared clinical laboratories could face federal fines of
$10,000/day. The reporting eligibility requirements are broad and may leave unprepared
clinical laboratories at significant risk.
“Receive more than 50% of their Medicare revenues from laboratory and physician services during a data collection period.
“Laboratories will collect private [payer] data from January
1, 2019, through June 30, 2019, and report it to CMS by March 31, 2020.”
In addition to shrinking margins, increased competition,
reduced reimbursement rates, and ever-changing regulations, clinical
laboratories now face new fines that could prove financially catastrophic for
even the largest, most efficient labs.
New Rules and
Reporting Requirements Threaten Unprepared Labs
Healthcare reform continues to reshape how healthcare is both delivered and billed across the country. GenomeWeb reported in 2017 that CMS expects PAMA to save the government $3.93 billion by 2028.
While medical laboratories continue to grapple with the
impact of reduced reimbursement rates under PAMA’s revised CLFS final rule, the
new rules for what constitutes an “applicable lab” and the new reporting
requirements that started January 1, 2019, add yet another level of complexity
to reporting and compliance concerns.
Rodney Forsman, Assistant Professor Emeritus of Lab Medicine and Pathology at the Mayo Clinic College of Medicine, in Rochester, MN, told Dark Daily that “Laboratories must work to identify reporting concerns, billing and IT limitations, and identify current statutes and limitations to present to compliance officers and stakeholders. Failure to do so could leave labs liable for fines of up to $10,000 per day.”
Compliance Will Be a
Team Effort
He further emphasizes that compliance with reporting
requirements will involve a range of stakeholders within the hospital and its
laboratory. Information technology (IT) teams, compliance officers, laboratory C-suite
executives, and billing departments all will play a role in implementing the
changes needed and reporting the data required.
Therefore, understanding exactly what regulations require—and
what is at stake—is crucial to not only implement critical changes, but to ensure
that the lab understands and is on-board with said changes.
Considerations include:
Understanding the new collection and reporting
periods;
Assessing billing and IT limitations in relation
to reporting requirements; and,
Implementing proper data capture and validation
systems ahead of data submission.
Rodney Forsman (left), Assistant Professor Emeritus of Lab Medicine and Pathology at the Mayo Clinic College of Medicine, and Brian Kemp (right), Vice President of Change Healthcare, stress that a current understanding of PAMA’s impact is crucial and that clinical laboratories are at considerable risk if they are not compliant with the latest PAMA requirements. (Photo copyright: Dark Daily.)
This important webinar will include:
A brief overview of PAMA;
The latest updates to PAMA reporting
requirements; and,
Actionable information for applicable labs
required to meet them.
The speakers will also cover concerns for hospital outreach programs and specific CMS 1450 14X Type of Bill (TOB) billing changes to help hospital COOs, CFOs, CIOs, contract officers, and compliance officers understand the latest implications of ongoing PAMA requirements.
Laboratory directors, managers, administrators, and IT and
billing staff will want to attend this critical webinar to learn essential PAMA
reporting considerations and pitfalls to avoid.
(To register for this
critical Feb. 20th webinar, click here. Or, copy and paste this URL into your browser: https://www.darkdaily.com/webinar/pama-in-2019-what-labs-need-to-know-to-collect-data-report-on-time-and-avoid-10000-per-day-penalties/.)
With a now-estimated price tag of $16.1 billion, federal regulators and government representatives question the VA’s replacement for their VistA medical records system
Originally estimated to cost $10 billion, a contract to
replace the federal Department of Veterans
Affairs (VA) electronic
health record (EHR) system will now cost $16.1 billion, according to new
estimates, and this has drawn increased scrutiny from regulators and the media.
ProPublica reports that the initial
deal signed in May 2018 between the VA and Cerner,
one of the nation’s largest vendors of laboratory
information systems (LIS) and anatomic pathology information systems,
included a $10-billion ‘no-bid’ contract to replace the VA’s aging VistA medical records system
over 10 years. Since then, that estimate has ballooned to $16 billion, and with
this latest increase, is now at $16.1 billion.
One ongoing challenge facing clinical
laboratories and anatomic
pathology groups is maintaining interfaces to the plethora of disparate EHR
systems implemented in healthcare networks across the country. It’s a costly
undertaking that has nearly bankrupted many healthcare providers.
Thus, these developments could impact how medical
laboratories and pathology groups work and communicate with the VA in the
future and are worth paying attention to.
In response, John Windom,
Executive Director of the federal government’s Office of Electronic Health Record Modernization (OEHRM), told the House Committee that the VA’s
original estimate failed to include roughly $35 million/year for VA government employee
costs over the decade-long Cerner contract.
“We have to have highly qualified subject matter experts to
grade the implementation efforts of Cerner. Those people in the industry cost
money,” noted Windom, Health Data Management reported.
This review hearing came just after ProPublica reported on a progress report where Cerner had assigned
an alert rating of “yellow trending toward red” to the VA’s EHR implementation efforts.
“It scares the hell out of me,” Ken Kizer, MD, MPH, CEO of health information technology (HIT) developer Medsphere Systems, and former Under Secretary for Health at the VA, told ProPublica. “I don’t think the VA, given other issues, has the luxury to have something that doesn’t work.” (Photo copyright: UC Davis Health.)
Deploying a new EHR in a system as large as the VA is a
highly complex operation. Adding in government oversight—and coordinating
development and deployment between all the parties involved—further complicates
the VA and Cerner’s efforts.
One complication not receiving much coverage is the fact
that EHR systems designed primarily for insurance billing purposes may be
incompatible with the needs of the VA and other federal agencies that do not
bill insurance companies.
“VA is different. The focus of the VA’s electronic medical
record is never about clinical documentation to support billing. It’s about
giving the information to the provider at the right time to inform the best
care. There are true risks to patients if they don’t do this right,” Heather
Woodward-Hagg, PhD, former National Program Director (Acting), Veterans
Engineering Resource Centers (VERC) and Founding Director, Veterans Affairs
Center for Applied System Engineering (VA-CASE), told ProPublica.
Nevertheless, according to coverage of the Review Committee
hearing by MeriTalk, Windom remains hopeful
that the project’s financials will improve. “There are going to be efficiencies
gained we can’t forecast at this point,” he told the Committee members.
According to MeriTalk, the original deal between
the DoD, Cerner, and Leidos in 2015 was estimated
at $4.3 billion. However, in July 2018, the DoD increased the project budget by
$1.2 billion—bringing the total estimate to $5.5 billion.
Still, this falls far short of the VA estimate of $16.1
billion leaving regulators and media outlets questioning the health and
oversight of the Cerner/VA project.
The VA estimate also is well above the cost of other notable
EHR implementations—such as the development and deployment of Kaiser
Permanente’s HealthConnect EHR.
Speaking with InfoWorld in 2013, Philip Fasano, then CIO
of Kaiser Permanente, noted
that it cost roughly $4 billion to build a system alongside Epic to serve their
9-million members. When asked what it would take to implement a similar system
nationally, he estimated costs in the “tens of billions.”
The Hidden Costs of
EHR Implementation
Speaking with Becker’s Hospital Review in 2016, Eric Helsher, Vice
President of Client Success at Epic, highlighted
how difficult it is to budget for such upgrades. “It’s misleading to say, ‘A
hospital is undergoing a $X million Epic
implementation,’ because the install includes far more than simply the Epic
software,” he said. “An EHR from any vendor requires technology like servers
and storage to house the software—be it on-premise
or in the Cloud—and laptops and mobile devices to access it. That would be like
if you go buy a fully loaded laptop and attribute that full cost to Microsoft
Word. You needed the computer to get Word.”
Whether the VA and Cerner can determine ways to bring the
contract in line with budgets remains to be seen. However, while healthcare
reform highlights EHR implementation and interoperability as major concerns in
the modern US healthcare landscape, the VA’s latest attempts at replacing their
VistA medical records system serves as a reminder of the complexity and hidden
costs facing healthcare providers working to meet healthcare reform
requirements and offer a more personalized care experience.
This, of course, applies equally well to clinical
laboratories.
Most of the hospital closures occurred in states that did not expand their Medicaid programs following the Affordable Care Act of 2014
Sustained financial pressure is not limited to clinical
laboratories. Rural hospitals are under grave financial pressure as well.
These hospitals are particularly vulnerable, and many have closed their doors,
leaving local physicians and independent pathologists in those communities with
an unclear path going forward.
And Medicaid
expansion, or more accurately the lack thereof, may have played a major
role in these closures.
Medicaid Expansion
‘Coverage Gap’ Involved in Rural Hospital Closures
Medicaid expansion seems to be one factor affecting hospital
closings. According to Becker’s Hospital Review (Becker’s) more hospitals have closed in
states where Medicaid was not expanded following the passage of the Affordable
Care Act in 2014.
This is likely related to the increasing number of uninsured
people in those states. Incomes tend to be lower in rural areas and the number
of uninsured people is higher there than in urban settings.
In a report on this coverage gap, the Kaiser
Family Foundation (KFF) explains, “In states that do not expand Medicaid,
many adults fall into a ‘coverage gap’ of having incomes above Medicaid
eligibility limits, but below the lower limit for Marketplace premium tax
credits.”
The graphic above is taken from the North Carolina Rural Health Research Program study. It shows the location of 95 hospitals that closed between 2010 and 2018. The researchers defined rural hospital closures as “… any short-term, general acute, non-federal hospital that is A) not located in a metropolitan county, or B) is located in a RUCA [Rural Urban Commuting Area] type 4 or higher, or C) is a Critical Access Hospital. For the purposes of this project, we have defined a hospital closure as the cessation in the provision of in-patient services.” (Photo copyright: University of North Carolina.)
Most Hospital
Closures in Rural Southern United States
Approximately 2.2 million people are affected by the
coverage gap, and there are similarities between where those people live and
where hospitals are closing. For example, 89% of those caught in the coverage
gap live in the south—where the majority of hospitals have closed, KFF noted.
According to Becker’s:
Texas has seen the most closures with 15;
Tennessee is second with nine closures since
2010;
Next is Georgia at seven; and,
Alabama, Mississippi, North Carolina, and
Missouri are tied each with five hospitals closed in the last few years.
About a third of the hospitals (21) that closed between 2013
and 2017 were 20-35 miles away from the next nearest hospital, according to a
report given to Congress by the Medicare
Payment Advisory Commission in June of last year.
A printable list of the 95 closed rural hospitals can be
downloaded by clicking on this
link.
GAO Reports For-Profit
Hospitals Most Vulnerable
The combination of lower incomes and fewer insured people
makes it difficult for hospitals to cover their fixed costs, leading to
bankruptcy. According to a report released by the Government Accountability
Office (GAO), for-profit hospitals have been disproportionately affected by
bankruptcy.
Only about 11% of the hospitals in rural areas
were for-profit organizations in 2013;
However, 40% of those hospitals that closed due
to bankruptcy between 2013 and 2017 were for-profit.
“While Medicaid expansion has improved all hospitals’
operating margins and total margins, the effect was particularly pronounced in
rural areas,” noted a report from the Center
on Budget and Policy Priorities. That’s because uncompensated care is
provided more often in for-profit, rural hospitals located in states where Medicaid
expansion did not occur.
Healthcare is undergoing massive changes and the reasons for
the rising number of health system and hospital bankruptcies are complex and
layered. The role of pathology labs isn’t always clear and many clinical
laboratories are caught in shifting sands without a clear path forward. In
rural areas, where hospitals are closing at an alarming rate, that is
particularly true.
Thus, clinical laboratory managers and stakeholders should
focus on improving outreach and solidifying revenues to navigate the uncertain
waters that lay ahead. Especially in poorer states where high numbers of people
cannot qualify for Medicaid coverage.
Pharmaceutical developers are combining genetic sequencing and precision medicine to create new drug therapies and cancer treatments designed for specific patients
Most anatomic pathologists are aware of the rapid advances in the field of cancer immunotherapy—sometimes also called immune-oncology. This is an area of healthcare where precision medicine and personal genetics become crucial elements in developing more effective drug regimens.
Scientists are combining those two areas of research to develop vaccines designed for specific individuals based on the genetic characteristics of their DNA. This is why there are great hopes that cancer immunotherapy can be used to artificially stimulate the immune system to treat cancer and improve the system’s natural ability to fight cancer.
San Francisco-based Genentech, a subsidiary of Swiss pharmaceutical giant Roche (OTCMKTS:RHHBY), is working with German company BioNTech to develop such personalized vaccines for cancer patients. Each vaccine would be based on the unique deoxyribonucleic acid (DNA) of a patient’s tumor.
Unlike typical vaccines, Genentech’s drug would not be taken
as a preventative measure. Instead, patients receive it after being diagnosed
with cancer.
Though
still being tested, this new line of research indicates that development of personalized
cancer treatments is progressing, as scientists strive to customizetreatments tumor by tumor.
Creating One-Off Vaccines
To create each vaccine, a patient first undergoes a tumor biopsy. The sample tissue is then sent to a genetics laboratory for full genome sequencing. Sophisticated algorithms analyze the genetic data and locate targets within the tumor that have the most potential for training the patient’s immune system to attack the existing cancer. A customized vaccine is then created for and administered to the patient.
“What’s truly revolutionary about this approach is that each vaccine uses a common molecular backbone—mRNA—that is uniquely tailored to an individual patient,” said Todd Renshaw, former Global Head of Clinical Contract Manufacturing at Genentech, in an article posted on the company’s website. “It’s the next step in personalized medicine.”
Vaccines are typically used to train the body’s immune
system to attack specific diseases that infiltrate the body from the outside. However,
cancer tumors are formed within the body’s own tissues, making it difficult for
the immune system to detect them. Thus, vaccines haven’t shown much promise for
treating cancer.
“Vaccines work by exposing the immune system to ‘non-self’ proteins known as antigens, priming it to recognize and eliminate the invaders. But in the case of cancer cells, most proteins are the same as those on healthy cells,” said Lélia Delamarre, Senior Scientist in Cancer Immunology at Genentech, in the online article. “This makes it hard to identify which antigen to use in a vaccine.”
Global
testing on the vaccine has commenced with a focus on ten cancers in upwards of
560 patients.
Barriers to Creating Individual Vaccines
The American Cancer Society estimates there were 1,735,350 new cancer diagnoses in the US in 2018—and 609,640 cancer deaths—making it the second leading cause of death in the US after heart disease.
A
truly customized cancer treatment in the form of a vaccine could be a major
breakthrough in treating this deadly disease. However, there are significant
barriers to developing such a vaccine.
For
starters, the vaccines cannot be manufactured in batches, packaged, warehoused,
or delivered to pharmacies in bulk. The personalized vaccines must be
manufactured in single patient doses, which could be prohibitively costly.
Nevertheless, this research represents an exciting
opportunity for anatomic pathologists and clinical laboratories with genetics
capabilities which would be needed to secure and sequence tumor biopsies for
guiding the creating of the customized vaccines.
Pathologists should track this trend closely and work within
their group practices to ensure they have the analyzers, informatics, and
expertise required to perform this type of testing for patients within their
communities.
While clinical laboratories may not be directly affected by copay accumulators, anything that affects patients’ ability to pay for healthcare will likely impact lab revenues as well
Here’s a new term and strategy that some big employers are
deploying in an attempt to control the choice of health benefits provided to
their employees. The term is “copay accumulator” and it is intended to offset
efforts by pharmaceutical companies to minimize what consumers must pay
out-of-pocket for expensive prescription drugs.
Clinical laboratory managers and pathologists will have a front row seat to watch this next round in the struggle between industry giants for control over how patients pay for drugs and treatment regimes.
Pharmaceutical companies on one side and health insurers and employers on the other side have played brinksmanship over medication copays for years. Now at the center of this struggle are copay accumulators, a relatively new feature of plans from insurers and pharmacy benefit managers (PBMs) on behalf of the large employers they serve.
More than 41-million Americans use copay accumulators, and about nine million use similar though limited copay maximizer programs, Zitter Health Insights, a New Jersey-based pharma and managed care consultancy firm, told Reuters.
Now, big employers are getting in on the game. Walmart
(NYSE:WMT) and Home Depot (NYSE:HD) are among a growing number of companies using
copay accumulators and copay maximizers to keep their healthcare costs down and
encourage employees to seek lower-cost alternatives to expensive brand
prescriptions (generic drugs).
About 25% of employers currently use such programs, and 50% of employers are anticipated to be doing so in just two more years, the National Business Group on Health told Reuters.
What Are Copay
Accumulators and How Do They Work?
In response to popular drug company discount cards,
insurance companies developed the “copay accumulator.” Here’s how it works.
Typically, patients’ insurance plan deductibles can be thousands
of dollars. Thus, even after plan discounts, patients often pay hundreds, even
thousands of dollars each month for prescribed medications. Insurance companies
see a beneficial side to this, stating the cost encourages patients to be aware
of their medications and motivates them to try lower-cost non-branded
alternatives (generic drugs), all of which saves insurance plans money.
However, many patients with high-deductibles balk at paying
the high cost. They opt to not fill prescriptions, which costs pharmaceutical
companies money.
To encourage patients to fill prescriptions, drug companies
provide discount cards to help defray the cost of the drugs. The difference
between the discounted payment and the full price of the drug is paid by the
pharmaceutical company. But these discount cards interfere with insurance
companies’ ability to effectively track their enrollees’ drug usage, which
impacts the payers’ bottom lines.
When a patient uses a drug discount card at the point-of-sale, the sale is noted by the patient’s health insurer and the insurer’s copay accumulator program kicks in. It caps the total accumulated discount an enrollee can take for that medication and prevents any patient payments to apply toward the plan’s deductible. Once the drug company’s discount card threshold is reached, the patient bears the full cost of the drug, a ZS Associates Active Ingredient blog post explained.
Critics of copay accumulators point out that patients could
end up paying full price for extremely expensive prescriptions they previously
accessed with discount cards, while simultaneously making no progress toward
fulfilling their insurance deductibles. Or, they will simply stop taking their
medications altogether.
“A medication which previously cost $7 may suddenly cost hundreds or even thousands of dollars because the maximum amount of copay assistance from the [drug] manufacturer was reached,” noted Ken Majkowski, Pharm.D, Chief Pharmacy Officer at FamilyWize (a company that offers its own prescription savings programs), in a blog post. “Since the health plan will no longer allow the copay amounts to contribute to the patient’s deductible, the cost of the medication remains very high.”
Major Employers Implement
Their Own Copay Accumulator Programs
Enter the next goliath into the fray—the large employer. Executives
at Walmart and Home Depot say discount drug coupons drive up healthcare costs
and give their employees and their family members no incentive to explore lower
cost alternatives, Reuters reported.
Walmart’s pharmacy benefits are managed by Express Scripts, a prescription benefit plan provider that fills millions of prescriptions annually, according to the company’s website. Meanwhile, Home Depot’s pharmacy benefits are operated by CVSHealth, which focuses on therapies for cystic fibrosis, hepatitis C, cancer, HIV, psoriasis, pulmonary arterial hypertension, and hyperlipidemia, Reuters noted.
Insurance Associations
Weigh-In
Health insurance company representatives say the need for copay accumulators begins with the high price of pharmaceuticals. Insurers are not the only ones concerned about these costs. The American Hospital Association (AHA), the Federation of American Hospitals (FAH), and the American Society of Health-System Pharmacists (ASHP) recently released a report showing total drug spending per hospital admission increased by 18% between 2015 and 2017, and some drug categories rose more than 80%.
“The bigger question is why do we need copay coupons at all? It’s very important to recognize the problem starts with the [drug] price. This is the real underlying problem,” Cathryn Donaldson, Director of Communications, America’s Health Insurance Plans (AHIP), told the Los Angeles Times.
In their blog post, ZS Associates advised drug companies to
“push-back” on the copay accumulators. The Evanston, Ill.-based consultancy
firm recommends pharma executives change the way they run the discount cards—such
as paying rebates directly to patients instead of working through pharmacies.
Medical laboratory leaders need to be aware of programs,
such as copay accumulators, and the associated issues that affect patients’
ability to pay for their healthcare. Because large numbers of patients struggle
to pay these high deductibles, it means clinical laboratories will be competing
more frequently with hospitals, physicians, imaging providers, and others to
get patients to pay their lab test bills.