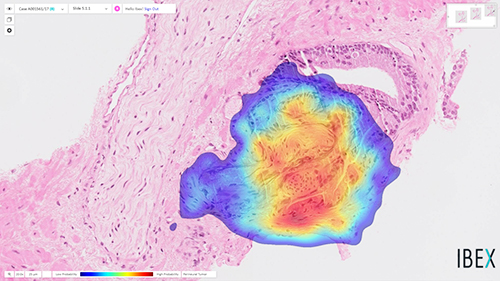
Working from tissue slides similar to those used by surgical pathologists, the algorithm accurately detects prostate cancer with an impressive 98% sensitivity
It could be that a new milestone has been reached on the road to using artificial intelligence (AI) to help anatomic pathologists diagnose cancer and other diseases. A research collaboration between a major American university and an Israeli company recently published a study about the ability of an AI algorithm to correctly diagnose prostate cancer.
The scientists trained the Galen Prostate AI to recognize prostate cancer by having it examine images from over a million parts of stained tissue slides taken from patient biopsies. Expert pathologists labeled each image to teach the algorithm how to distinguish between healthy and abnormal tissue. The AI was then tested on 1,600 different tissue slide images that had been collected from 100 patients seen at UPMC who were suspected of having prostate cancer.
“Humans are good at recognizing anomalies, but they have their own biases or past experience,” said Rajiv Dhir, MD, Chief Pathologist and Vice Chair of Pathology at UPMC Shadyside Hospital, Professor of Biomedical Informatics at University of Pittsburgh, and senior author of the study, in a UPMC news release. “Machines are detached from the whole story. There’s definitely an element of standardizing care.”
The image above is “of prostate cancer (represented by the heatmap) detected by the Ibex Galen Prostate [AI] solution on a biopsy that was previously diagnosed as benign by the pathologist,” stated an Ibex news release announcing the UPMC study. (Photo copyright: Ibex.)
UPMC Algorithm Goes Beyond Cancer Detection, Exceeds Human Pathologists
The researchers also noted that this is the first algorithm to extend beyond cancer detection. It reported high performance for tumor grading, sizing, and invasion of surrounding nerves—clinically important features of pathology reports.
“Algorithms like this are especially useful in lesions that are atypical,” Dhir said. “A nonspecialized person may not be able to make the correct assessment. That’s a major advantage of this kind of system.”
The algorithm also flagged six slides as potentially containing abnormal tissue that were not flagged by human pathologists. However, the researchers pointed out that this difference does not mean the AI is better than humans at detecting prostate cancer. It is probable, for example, that the pathologists simply saw enough evidence of malignancy elsewhere in the patients’ samples to recommend treatment.
Other Studies Where AI Detected Prostate Cancer
The UPMC researchers are not the first to use AI to detect prostate cancer. In February, The Lancet Oncology published a study from researchers at Radboud University Medical Center (RUMC) in the Netherlands who developed a deep learning AI system that could determine the aggressiveness of prostate cancer in certain patients.
For that research, the RUMC scientists collected 6,000 biopsies from more than 1,200 men. They then showed the biopsy images along with the original pathology reports to their AI system. Using deep learning, the AI was able to detect and grade prostate cancer according to the Gleason Grading System (aka, Gleason Score), which is used to rate prostate cancer and choose appropriate treatment options. The Gleason Score ranges from one to five and most cancers obtain a score of three or higher.
“Systems such as ours can be used in different ways. First, it can be used to screen biopsies and to filter out the easy (benign) cases. This could reduce the workload for pathologists,” said Wouter Bulten, a PhD candidate at Radboud who worked on the study, in an interview with HemOnc Today. “Second, the system can be used as a second opinion after the pathologist’s initial read. The system can flag a case if its opinion differs from that of the pathologist. It also can give feedback during the first read, showing the pathologist where to look. In this case, the pathologist needs only to confirm the opinion of the AI system.”
Can Today’s AI Outperform Human Pathologists?
In their research, the Radboud team discovered that their AI system was able to achieve pathologist-level performance and, in some cases, even performed better than human pathologists. However, they do not foresee AI replacing the need for pathologists, but rather emerging as another method to use in cancer detection and treatment.
“We see our system as an additional tool that the pathologist can use. Although our system performs very well, it still makes mistakes,” stated Bulten. “These mistakes are often different from those a human would make. We believe that when you merge the expertise of the pathologist with the second opinion of an AI system, you get the best of both worlds.”
According to the American Cancer Society, prostate cancer is the second most common cancer among men in the US, after skin cancer. The organization estimates there will be approximately 191,930 new cases of prostate cancer diagnosed and about 33,330 deaths from the disease in the US in 2020.
Though the UPMC study focused only on prostate cancer, the scientists believe their algorithm can be trained to detect other types of cancer as well. AI in clinical diagnostics is clearly progressing, however more studies will be required. Nevertheless, if AI can truly become a useful tool for anatomic pathologists to detect cancer earlier, we may see a welcomed reduction in cancer deaths.
Pooled testing could become a critical tool for clinical laboratories to spot the SARS-CoV-2 coronavirus among asymptomatic and pre-symptomatic individuals
COVID-19 testing for individuals has expanded in the US, but the number of people actually tested remains a small proportion of the country’s total population and clinical laboratory testing supply shortages continue to hamper progress. A technique known as pooled testing may help. Federal experts hope it will substantially increase the number of individuals who are tested for the SARS-CoV-2 coronavirus before it makes a possible resurgence in the fall.
One-by-one, some of the nation’s largest clinical laboratory organizations are developing the capability to do pooled testing. For example, on July 18, the Food and Drug Administration (FDA) announced it had issued Quest Diagnostics (NYSE:DGX) an Emergency Use Authorization (EUA) for its SARS-CoV-2 rRT-PCR test, and that it is valid for up to four individual samples as a pooled test.
Quest’s rRT-PCR test was the first COVID-19 diagnostic test to be authorized for use with pooled samples, the FDA noted in a new release.
In the FDA’s statement announcing Quest’s EUA for its rRT-PCR test, Stephen M. Hahn, MD (above), FDA Commissioner, said, “This EUA for sample pooling is an important step forward in getting more COVID-19 tests to more Americans more quickly while preserving testing supplies.” He added, “Sample pooling becomes especially important as infection rates decline and we begin testing larger portions of the population.” (Photo copyright: CBS News.)
Following the announcement of Quest’s EUA, on July 24 the FDA announced LabCorp’s (NYSE:LH) EUA for its COVID-19 real-time reverse transcription polymerase chain reaction (rRT-PCR) test. The test, the EUA states, is intended for the “qualitative detection of nucleic acid from SARS-CoV-2 in upper and lower respiratory specimens” in individuals suspected of COVID-19, using “a matrix pooling strategy (i.e., group pooling strategy), containing up to five individual upper respiratory swab specimens (nasopharyngeal, mid-turbinate, anterior nares or oropharyngeal swabs) per pool and 25 specimens per matrix.”
Exponentially Increasing Testing
In pooled testing, instead of performing a coronavirus test on every specimen received by a clinical laboratory, samples from each individual specimen are taken and then combined with samples from other specimens. A single test is then performed on the entire collection of specimen samples.
If the results of the pooled samples are negative for coronavirus, it is safe to assume that all the specimens in the batch are negative for the virus. If the pooled sample comes back positive, then it will be necessary to go back to the original specimens in that pooled sample and test each specimen individually.
In an exclusive interview with Dark Daily’s sister print publication The Dark Report, Steven H. Hinrichs, MD, Chair of the Department of Pathology and Microbiology at the University of Nebraska Medical Center (UNMC), noted that one pitfall of pooled testing is that it works best in areas of low virus prevalence.
“For pooled testing, the ideal level of low prevalence would be an infection rate below 10%,” he said, adding, “For COVID-19 test manufacturers, pooled testing has the potential to reduce the number of standard tests labs run by roughly 40% to 60%, depending on the population being tested.
“Cutting the number of COVID-19 tests would be a disadvantage for test manufacturers, because pooled tests would identify large numbers of uninfected individuals who would not require standard testing with EUA tests.
“On the other hand, this policy would be a significant advantage for US labs because pooled testing would cut the number of standard tests,” he continued. “Clinical labs would save money on tests, reagents, and other supplies. It would also ease the burden on the lab’s technical staff,” Hinrichs concluded.
“In our study, we show that it’s reasonable to pool five samples, although we realized that some people may want to pool 10 samples at once,” noted Hinrichs. “But even if one sample is positive in a pool of five, then testing five samples at once saves 80% of our costs if all of those samples are negative. But, if one sample is positive, each of those five samples needs to be retested using the standard test,” Hinrichs explained.
During an American Society for Microbiology (ASM) virtual conference, Deborah Birx, MD, White House Coronavirus Response Coordinator, said, “Pooling would give us the capacity to go from a half a million tests per day to potentially five million individuals tested per day,” STAT reported.
Advantages of using pooled testing for the coronavirus include:
Expanding the number of individuals tested,
Stretching laboratory supplies, and
Reducing the costs associated with testing.
Health officials believe that individuals who have COVID-19 and are asymptomatic are largely responsible for the rising number of coronavirus cases in the US, STAT reported.
“It allows you to test more frequently in a population that may have a low prevalence of disease,” Benjamin Pinsky, MD, PhD, Associate Professor, Departments of Pathology and Medicine at Stanford University School of Medicine, told STAT. “That would allow you to test a lot of negatives, but also identify individuals who are then infected, before they develop symptoms.”
Pooled testing also could be advantageous for communities where COVID-19 is not prevalent, in neighborhoods that need to be tested during an outbreak, and for schools, universities, organizations, and businesses that want to remain safely open while periodically monitoring individuals for the virus, CNN reported.
“The goal is to increase the capacity of testing in a relatively straightforward fashion,” Pinsky told STAT. “The caveat is that by pooling the sample, you’re going to reduce the sensitivity of the test.”
According to Pinsky, “pooling only makes sense in places with low rates of COVID-19, where you expect the large majority of tests to be negative. Otherwise, too many of the pools would come back positive for it to work as a useful surveillance tool,” STAT reported.
As Clinical Lab Testing Increases, Pooled Testing for COVID-19 Could Be Critical
Pooled testing has been used in other countries, including China, to test larger amounts of people for COVID-19.
“If you look around the globe, the way people are doing a million tests or 10 million tests is they’re doing pooling,” Birx said during the ASM virtual conference, CNN reported.
In a press release, the American Clinical Laboratory Association (ACLA) stated that about 300,000 tests for COVID-19 were performed per day in labs across the US in late June. That number was up from approximately 100,000 tests being performed daily in early April.
“All across the country, clinical laboratories are increasing the number of labs processing tests, purchasing additional testing platforms, and expanding the number of suppliers to provide critical testing materials,” said Julie Khani, ACLA President in the press release. “However, the reality of this ongoing global pandemic is that testing supplies are limited. Every country across the globe is in need of essential testing supplies, like pipettes and reagents, and that demand is likely to increase in the coming months.”
Clinical laboratory managers will want to keep an eye on these developments. As the need for COVID-19 testing increases, pooled testing may provide an efficient, cost-effective way to spot the coronavirus, especially among those who are asymptomatic or pre-symptomatic and who display no symptoms.
Pooled testing could become a critical tool in the diagnosis of COVID-19 and potentially decrease the overall number of deaths.
Understanding how superspreading occurs can help clinical lab leaders slow and even prevent the spread of SARS-CoV-2 within their communities and health systems
Clinical laboratories understand the critical importance of preventing the spread of infection. However, according to the Boston Globe, researchers worldwide are learning that roughly 80% of new COVID-19 cases are caused by just 10% of infected people. Those people are called superspreaders.
It’s critical that medical laboratory managers are aware of the role superspreaders play in transmitting SARS-CoV-2, the coronavirus that causes the COVID-19 illness.
Clinical lab leaders who understand how superspreading occurs can take steps to protect staff, patients, and anyone who visits the facility. Because lab personnel such as couriers and phlebotomists, among others, come into contact with large numbers of people daily, understanding how to identify superspreaders could limit transmissions of the coronavirus within the laboratory, as well as within hospital networks.
Superspreading versus Plodding
Influenza and other viruses tend to spread in a way that epidemiologists call “plodding.” One person infects another, and the virus slowly spreads throughout the population. However, scientists around the globe are finding that SARS-CoV-2 transmission does not fit that pattern. Instead, a few infected people appear to be transmitting the virus to dozens of other people in superspreading events, Boston Globe reported.
“You can think about throwing a match at kindling. You throw one match, it might not light the kindling. You throw another match, it may not light the kindling. But then one match hits the right spot and all of a sudden the fire goes up,” Ben Althouse, PhD, principal scientist and co-chair of epidemiology at the Institute for Disease Modeling in Bellevue, Wash., told the Boston Globe.
But because roughly 90% of infected people aren’t spreading the virus, identifying who the superspreaders are can be a challenge. Nevertheless, limiting situations in which superspreading is likely to occur could greatly reduce the spread of infection.
Samuel Scarpino, PhD (above), Assistant Professor in the Network Science Institute at Northeastern University, says that “preventing superspreader events could go a long way toward stopping COVID-19,” Scientific American reported. “All of the data I’m seeing so far suggest that if you tamp down the superspreader events, the growth rate of the infections stops very, very quickly,” Scarpino said. (Photo copyright: University of Vermont.)
Examples of Superspreading Events
One of the first big outbreaks in the United States was an example of a superspreading event. The Biogen (NASDAQ:BIIB) leadership conference in late February in Boston resulted in at least 99 cases of COVID-19 just in Massachusetts, reported the Boston Globe.
Several superspreading events have occurred in houses of worship. One well-documented example prompted a CDC Morbidity and Mortality Weekly Report, titled, “High SARS-CoV-2 Attack Rate Following Exposure at a Choir Practice—Skagit County, Washington.” The 122-member choir met for practice twice in March. On March 3 no one had symptoms, but one person had cold-like symptoms at the March 10 practice. Eventually, 53 members tested positive for SARS-CoV-2.
On May 30, a Texas family held a birthday party, Medical Xpress reported. Twenty-five people attended the party, which only lasted a few hours. The family followed the state’s guidelines for gatherings, however one of the hosts was infected with the SARS-CoV-2 coronavirus and wasn’t aware of it. Seven attendees contracted it, and those seven spread the virus to an additional 10 family members. A total of 18 members of a single family were infected.
There are commonalities among the documented superspreading events. Most occur indoors, often in poorly ventilated areas. Some activities cause more respiratory droplets to be expelled than others, such as singing. Some respiratory droplets are released simply by breathing, and many more are expelled when a person talks. Talking louder expels even more droplets into the air.
Are Some People More Likely to Spread the Coronavirus than Others?
The fact that so few people are responsible for the majority of transmissions of the virus raises questions. Do some people simply have more virus particles to shed? Is biology a factor?
One factor may be how long the SARS-CoV-2 coronavirus is in the body before symptoms of the COVID-19 illness manifest.
“If people got sick right away after they were infected, they might stay at home in bed, giving them few opportunities to transmit the virus,” noted Scientific American in “How ‘Superspreading’ Events Drive Most COVID-19 Spread.” However, CDC states on its website that “The incubation period for COVID-19 is thought to extend to 14 days, with a median time of 4-5 days from exposure to symptoms onset. One study reported that 97.5% of persons with COVID-19 who develop symptoms will do so within 11.5 days of SARS-CoV-2 infection.”
During that time, infected individuals may transmit the virus to dozens of other people. The CDC estimates that about 40% of transmission occurs in pre-symptomatic people, Scientific American reported.
But it’s not all bad news. The fact that circumstances may be more important than biology might be good news for clinical laboratories. “Knowing that COVID-19 is a superspreading pandemic could be a good thing. It bodes well for control,” Nelson told the Boston Globe.
Clinical laboratory managers are encouraged to follow CDC recommended safety protocols, titled, “Guidance for General Laboratory Safety Practices during the COVID-19 Pandemic.” They include social distancing, setting up one-way paths through lab areas, sanitizing shared surfaces such as counters and benchtops, and implementing flexible leave policies so that sick employees can stay home.
Following these guidelines, and being aware of superspreaders, can help medical laboratories and anatomic pathology groups keep staff and customers free of infection.
Though the test initially drew ‘raves’ from Trump administration, the FDA now suggests negative results should be confirmed with an additional ‘high-sensitivity authorized SARS-CoV-2 molecular test’
This spring, as the United States attempted to jump-start a national response to the SARS-CoV-2 coronavirus pandemic, the Trump administration heralded Abbott Laboratories’ five-minute test for COVID-19 as a major breakthrough. But even as the federal Food and Drug Administration (FDA) issued dozens of Emergency Use Authorizations (EUAs) to quickly get COVID-19 diagnostic tests into clinical use, the accuracy of some of those tests came into question—including Abbott’s ID NOW COVID-19 rapid molecular test.
The continuing controversy over Abbott’s ID NOW COVID-19 test shows how the national spotlight can be a double-edged sword, bringing both widespread favorable attention to a breakthrough technology, followed by heightened public scrutiny if deficiencies emerge. At the same time, from the first news stories about the Abbott ID NOW COVID-19 test, pathologists and clinical laboratory managers understood that this test always had certain performance parameters, as is true of every diagnostic test.
“Everybody was raving about it,” a former administration official, speaking on the condition of anonymity to discuss internal deliberations, said of ID NOW in an interview with Kaiser Health News (KHN). “It’s an amazing test, but it has limitations which are now being better understood.”
In a White House ceremony on March 29, 2020, President Trump praised his administration’s role in speeding up development “on both testing and treatment that will help us win our war against the coronavirus.” Among the moves highlighted was the FDA’s approval two days earlier of Abbott’s ID-NOW COVID-19 rapid molecular test (above), which the President stated, “delivers lightning-fast results in as little as five minutes,” adding, “Normally, this approval process from the FDA would take 10 months, and even longer, but we did it in four weeks.” (Photo copyright: Washington Post.)
FDA Warns Public about Inaccurate Test Results
On May 14, the FDA issued a public warning about the point-of-care test’s accuracy after receiving 15 “adverse event reports” indicating some patients were receiving “false negative results.”
“Regardless of method of collection and sample type, Abbott ID NOW COVID-19 had negative results in a third of the samples that tested positive by Cepheid Xpert Xpress when using nasopharyngeal swabs in viral transport media and 45% when using dry nasal swabs,” the NYU study authors stated.
Abbott Rebuts Criticism
In a statement following the FDA’s warning, Abbott said, “We’re seeing studies being conducted to understand the role of ID NOW in ways that it was not designed to be used. In particular, the NYU study results are not consistent with other studies. While we’ve seen a few studies with sensitivity performance percentages in the 80s, we’ve also seen other studies with sensitivity at or above 90%, and one as high as 94%.
“While we understand no test is perfect, test outcomes depend on a number of factors including patient selection, specimen type, collection, handling, storage, transport and conformity to the way the test was designed to be run. ID NOW is intended to be used near the patient with a direct swab test method,” Abbott’s statement added, noting the company would be “further clarifying our product information to provide better guidance” and “reinforcing proper sample collection and handling instructions.”
Then, on May 21, Abbott issued another statement highlighting an interim analysis of an ongoing multisite clinical study demonstrating ID NOW COVID-19 test performance is ≥94.7% in positive agreement (sensitivity) and ≥98.6% negative agreement (specificity) when compared to two different lab-based molecular PCR reference methods.
“We’re pleased ID NOW is delivering on what it was designed to do—quickly detect the virus in people who need to know now if they’re infected,” said Philip Ginsburg, MD, SAIM, Senior Medical Director, Infectious Disease, Rapid Diagnostics at Abbott, in the statement. “This is great news for people who are experiencing symptoms and want to take action before they infect others, reducing the spread of infection in society.”
Nonetheless, KHN reported on June 22 that the FDA had “received a total of 106 reports of adverse events for the Abbott test, a staggering increase. The agency has not received a single adverse event report for any other point-of-care tests meant to diagnose COVID-19.”
Second Comparison Study Results for Abbott’s ID NOW
The Abbott ID NOW test correctly identified 74% of positive samples. In comparison, Cepheid’s Xpert Xpress SARS CoV-2 test correctly identified 99% of positives. Negative agreement was 100% and 92.0% for ID NOW and Xpert, respectively.
The FDA’s testing policy for clinical laboratories and commercial manufacturers recommends diagnostic tests correctly identify at least 95% of positive samples. However, KHN pointed out, a senior FDA official in late May said coronavirus tests that were administered outside lab settings would be considered useful in fighting the pandemic even if they miss 20% of positive cases.
“There’s no way I would be comfortable missing two out of 10 patients,” Whittier told KHN.
Abbott ID-NOW’s Role in the Global Fight to Stop COVID-19
Abbott’s ID NOW COVID-19 test is promoted as delivering positive test results in five minutes and negative results in about 13 minutes. On its website and in news releases, Abbott maintains its test “performs best in patients tested earlier post symptom onset.”
In a July 17 statement, Abbott said, “ We have shipped 5.3 million of our rapid ID NOW tests to all 50 states, Washington DC, Puerto Rico and the Pacific Islands. The majority of these tests have been sent to outbreak hotspots and we’ve asked that customers prioritize frontline healthcare workers and first responders.”
It is common for a new diagnostic instrument and a new clinical laboratory test to be continually improved after initial launch. Thus, the performance of such devices at the time they are given clearance from the FDA to be used in clinical care can be much improved several months or years later.
Given the importance of a reliable point-of-care SARS-CoV-2 test during the pandemic, it can be assumed that Abbott Laboratories is working closely with its medical laboratory customers specifically to improve the accuracy, reliability, and reproducibility of both the instrument and the test kit.
Researchers found evidence indicating that the virus has—under selection pressure—made itself more stable, giving it a “significant boost in infectivity”
While the COVID-19 pandemic continues to spread across the United States and throughout the world, new research suggests that a coming genetic mutation within the SARS-CoV-2 coronavirus may make it much more dangerous than it already is. This finding has significant implications for clinical laboratories that perform COVID-19 testing and the in vitro diagnostics (IVD) companies that develop and manufacture tests for COVID-19.
The mutation, called D614G, will provide the coronavirus with sturdier spikes that will increase its ability to latch onto and infect cells. That’s according to a study conducted at The Scripps Research Institute (Scripps) in Jupiter, Fla., which found that a mutated coronavirus may be up to 10 times more infectious than the original strain.
“Viruses with this mutation were much more infectious than those without the mutation in the cell culture system we used,” said Hyeryun Choe, PhD, Professor, Department of Immunology and Microbiology, Scripps Research, and senior author of the study, in a Scripps news release.
A More Flexible and Potent Coronavirus May Be Coming
The researchers found that coronavirus particles containing the mutation tend to have four to five times more functional spikes than particles without the mutation. The spikes enable the virus to bind to cells more easily. The research suggests that the greater the number of functional spikes on the viral surface the greater the flexibility and potency of the coronavirus.
In the Scripps news release, Farzan said, “more flexible spikes allow newly made viral particles to navigate the journey from producer cell to target cell fully intact, with less tendency to fall apart prematurely.
“Over time, it has figured out how to hold on better and not fall apart until it needs to,” he added. “The virus has, under selection pressure, made itself more stable.”
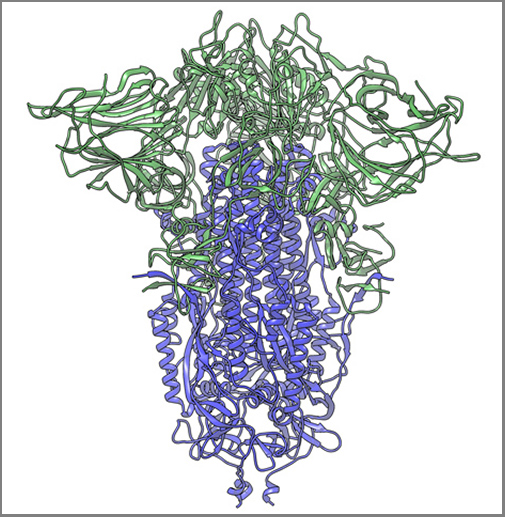
The image above, taken from the Scripps Research news release, shows “a cryogenic electron microscope image of a SARS-CoV-2 spike protein side view, the S1 section of the spike is shown in green and the S2 portion is shown in purple. This unique two-piece system has shown itself to be relatively unstable. A new mutation has appeared in the viral variant most common in New York and Italy that makes this spike both more stable and better able to infect cells.” (Graphic and caption copyright: Andrew Ward lab, Scripps Research.)
Mutation Makes SARS-CoV-2 Coronavirus ‘Much More Stable’
The two Scripps scientists have studied coronaviruses for nearly 20 years and performed extensive research on the Severe Acute Respiratory Syndrome (SARS) outbreak that occurred in 2003. They noted that there is a difference between spike proteins of SARS, an earlier strain of coronavirus, and the new SARS-CoV-2 strain.
The protein spikes of both strains were originally tripod shaped. However, the spikes of the SARS-CoV-2 coronavirus are divided into two different segments: S1 and S2. According to the published study: “The S1domain mediates receptor binding, and the S2 mediates downstream membrane fusion.”
This feature originally produced unstable spikes, but with the D614G mutation, the tripod breaks less frequently, which makes more of the spikes fully functional and the virus more infectious.
“Our data are very clear, the virus becomes much more stable with the mutation,” Choe said in the news release.
Is COVID-19 Spread Due to ‘Founder Effect’
The scientists also examined whether the spread of COVID-19 could have been the result of the “Founder Effect,” which is seen when a small number of variants fan out into a wide population by chance. Could the founder effect explain why COVID-19 outbreaks in some areas of the world were more severe than others? The researchers believe their data definitively answered that question.
“There have been at least a dozen scientific papers talking about the predominance of this mutation,” Farzan said. “Are we just seeing a founder effect? Our data nails it. It is not the founder effect.”
Hyeryun Choe, PhD (left), and Michael Farzan, PhD (right), scientists at Scripps Research explained that their research was performed using engineered viruses and that their observations of the virus and its mutation may not translate to increased transmissibility when a virus attaches to a host outside the lab. COVID-19 and its mutation appear to be relatively stable and are mutating at a rate slower than that of the seasonal flu, which may be critical factors in the development of a vaccine. (Photos copyright: Scripps Research.)
Findings Raise ‘Interesting’ Questions about the COVID-19 Coronavirus
Nevertheless, the two scientists are curious about some of their findings. “Our data raise interesting questions about the natural history of SARS-CoV-2 as it moved presumably from horseshoe bats to humans. At some point in this process, the virus acquired a furin-cleavage site, allowing its S1/S2 boundary to be cleaved in virus-producing cells. In contrast, the S1/S2 boundary of SARS-CoV-1, and indeed all SARS-like viruses isolated from bats, lack this polybasic site and are cleaved by TMPRSS2 or endosomalcathepsins in the target cells.
“In summary, we show that an S protein mutation that results in more transmissible SARS-CoV-2 also limits shedding of the S1 domain and increases S-protein incorporation into the virion. Further studies will be necessary to determine the impact of this change on the nature and severity of COVID-19,” the Scripps researchers concluded.
However, not all Scripps researchers agreed with the conclusions of Choe and Farzan’s research.
The Times of Israel reported that Kristian Andersen, PhD, a professor in the Department of Immunology and Microbiology, Scripps California Campus, told the New York Times that “other analyses of virus variants in labs had not found significant differences in infection rates.”
“That’s the main reason that I’m so hesitant at the moment,” Andersen said. “Because if one really was able to spread significantly better than the other, then we would expect to see a difference here, and we don’t.”
Times of Israel also reported that “In late May researchers in University College London said their studies of the genomes of more than 15,000 samples had not shown one strain being more infectious than others.”
So, the jury’s out. Nonetheless, clinical laboratory leaders will want to remain vigilant. A sudden increase in COVID-19 infection rates will put severe strain on already strained laboratory supply chains.
As digital healthcare continues to gain acceptance and regulatory support, clinical laboratories will need to help patients provide biological samples for virtual doctor visits
Patterns are emerging in healthcare that will likely impact clinical laboratories now and into the future. Trends in telehealth and mobile health (mHealth) that were just beginning to develop before the COVID-19 pandemic have accelerated with the outbreak, and many are predicted to remain once the pandemic is over, reported Healthcare Business and Technology.
Now comes virtual waiting rooms to go along with virtual doctor’s visits. One example is Banner Health of Phoenix, Arizona. The non-profit has more than 50,000 employees in Ariz. and is the state’s largest employer. It operates 28 hospitals and multiple specialty clinics in six states, making it one of the largest health systems in the US as well.
Banner Health is working with LifeLink to deploy virtual waiting rooms in all of its 300 clinics.
What is a Virtual Waiting Room?
The Banner Health System includes 1,500 physicians who work in 300 clinics. More than one million patients in Arizona, California, Colorado, Nebraska, Nevada, and Wyoming are part of the system.
In the not too distant past, when patients visited Banner Health providers and received doctor’s orders for diagnostic tests, they then went to clinical laboratories or the lab’s patient service centers to provide a biological specimen for testing.
Now, because of COVID-19, patients at Banner Health clinics access virtual waiting rooms through a mobile device or computer. They check in virtually for video visits and may not visit a doctor’s office or medical facility at all. Instead, they engage their healthcare provider through a telehealth connection.
The introduction of the virtual waiting rooms is Banner Health’s response to the need for social distancing during the COVID-19 pandemic.
The virtual waiting rooms employ LifeLink chatbots, which interact with patients in a conversational way, and are available for both telehealth and in-person appointments. The chatbots can:
provide appointment reminders,
guide patients through completing necessary paperwork,
provide instructions on using telehealth technology,
check patients in for appointments, and
direct patients to an exam room for in-person doctor visits.
Banner Health used similar technology for patients visiting their emergency departments.
“The traditional patient experience of walking into an office, filling out paper forms, reading instructions and then waiting for an exam room had to change. LifeLink chatbots have already helped hundreds of thousands of Banner patients navigate emergency room visits, so the concept of digitizing regular doctor appointment visits with a mobile, virtual waiting room chatbot assistant was a natural extension of the technology,” said Jeff Johnson, JD, Vice President of Innovation and Digital Business at Banner Health, in a press release. (Photo copyright: Healthcare IT News.)
Both Patients and Healthcare Providers Need to Adapt
“The COVID-19 pandemic requires an entirely different level of thinking when it comes to providing routine patient services,” said Greg Johnsen, CEO at LifeLink, in the Banner Health press release. “Like the changes we are seeing in retail, healthcare providers need to adapt, and the waiting room experience is one area that will need to change. We take great pride in knowing that LifeLink chatbots are providing peace of mind and convenience for patients that need to see their doctors.”
A significant innovation is that patients can easily engage with the chatbots through a “one-click authentication process and then interact through a standard web browser,” rather than requiring them to download and install a mobile device app, Healthcare IT News reported.
“One of the key benefits of this chatbot technology is the ease of use,” said Banner Health’s Jeff Johnson in the press release. “Interactions that use natural language eliminate the need for user training, and there are no apps or passwords required so it’s simple for patients to interact with us securely, on any device. We have seen high engagement rates as a result.”
One thing seems certain, as COVID-19 causes increased anxiety over social distancing, it is likely that virtual healthcare, telehealth, and digital pathology will continue to be developed in the medical industry.
This has implications for clinical laboratories, because if patients are being scheduled virtually, it is just a small additional step to have the doctor see them virtually via telehealth. In such circumstances, medical laboratories will need to have a way for the patient to provide a specimen for lab testing.