By automating clinical chemistry and immunoassay testing, clinical laboratory leaders can improve throughput while reducing the stress on staff, laboratory expert says
The American Society for Clinical Pathology regularly conducts a vacancy survey of medical laboratories throughout the US. While the problem of lab department vacancy rates has been ongoing, the last survey reported showed increased rates for laboratory positions across all departments surveyed. Last year, burnout among healthcare workers reached a crisis level, reported Clinical Laboratory News.
As a result, staffing the clinical laboratory with qualified lab professionals resounds as a top concern—and at a time when expectations are perhaps the highest they have ever been for performance in healthcare operations, from general hospitals to the most complex integrated delivery networks.
Even in the midst of the clinical laboratory workforce shortage and chronic strain, laboratory leaders must still improve their labs’ processes and workflows; increase productivity; and expand routine and specialty testing to better serve patient populations.
Faced with unrelenting pressures to do more with less, lab directors are turning to automating certain departments of the laboratory as a way to:
Relieve the problems caused by an ongoing workforce shortage;
Improve workflows and processes through standardization;
Keep lab staff working on the most important tasks; and
Enhance the laboratory’s reach and grow the lab business in necessary ways.
How UMC Southern Nevada Prioritized STAT Runs, Consolidated Operations
One case in point highlights the University Medical Center (UMC) of Southern Nevada’s clinical laboratory. Located in Las Vegas, UMC is among the largest public hospitals in the United States. It is part of a recent master-planned Las Vegas Medical District (LVMD), and it is the only Level I trauma center in Nevada.
The laboratory needed to improve turnaround time and expand the test menu, among other goals, explained Scott Keigley, one of two General Laboratory Services Managers at UMC. While limited laboratory automation had already been applied broadly, the lab took its automation initiative one step further by connecting three high-volume automated clinical chemistry and immunoassay analyzers (CC/IA), an automated hematology line, and a coagulation analyzer.
The University Medical Center of Southern Nevada improved efficiency andstreamlined workflow by integrating a consolidated automated clinical chemistry and immunoassay analyzer (above) into the laboratory’s workflow. (Photo copyright: Siemens Healthineers)
An immediate benefit that UMC realized was consolidation of clinical lab operations. “Up until implementing our automated platform, we had a dedicated laboratory in our emergency room specifically to triage our emergency room tests,” Keigley explained. “You’re talking about not only a duplication of consumables, resources, and supplies, but also personnel.
“A big part of automating was showing our administration we were going to be able to eliminate that emergency room lab and still turn our results around as quickly and as efficiently without it,” Keigley added.
One of the ways that using an automated platform enabled consolidation of lab operations was by decreasing the turnaround times of STAT samples. “Our STAT turnaround times are way below many of the national thresholds or standards,” Keigley explained. “I’ll use troponin as an example. National threshold is 60 minutes from received to result, but we average about 30 minutes.
“Throughput definitely increased,” Keigley added, emphasizing that this increased throughput was actually accompanied by a reduced workload. “We’ve seen a reduction in the amount of hands-on time required to do the daily maintenance and quality controls. Once the daily maintenance and controls are completed, the chemistry department can usually be run by one person.”
Choosing a Consolidated Automated Chemistry and Immunoassay Platform
Described as flexible for adding components, modular, and scalable, a consolidated clinical chemistry and immunoassay analyzer (CC/IA) can run from 1 million to 3 million tests per year. Designed with innovative technological internal controls and sample handling—and other capabilities that include automated instrument calibration, maintenance, and quality control (QC) functions—the CC/IA platform also works as a standalone and is a first step toward implementing laboratory automation.
At UMC, multiple factors influenced the decision to add the platform, explained Keigley. “One reason was the increased productivity that it (the Atellica Solution) from Siemens Healthineers offers. This technology frees up our techs to do what we went to school to do. I can show anyone how to load samples on these analyzers in five minutes, but that’s not what it’s about.
“We were able to expand our test menu and our services. The platform allowed us to grow.” Keigley estimates that UMC’s test menu grew up to 20% after the change, both expanding the types of testing that could be offered and decreasing the number of send-outs. He estimates that the chemistry lab now processes about 2.6 million reportable results per year.
There were several (QC) features that Keigley believes UMC’s laboratory benefits from. The key QC features Keigley identified include onboard temperature-controlled storage, programmable run times, and barcode-labelled tube options from the control manufacturer that eliminate manual programming.
Operational Evaluation—Nexus Global Solutions, Inc. (Nexus), Plano, TX
While the primary driving factor in UMC’s decision to use the Atellica Solution platform was based on its individual laboratory’s needs, a recent study commissioned by Siemens Healthineers illustrated the benefits of this system.
An operational comparison report by Nexus found that there are multiple advantages associated with this integrated automation platform—as a standalone component—when compared to a similar offering.
Specifically, the Nexus report found:
Start-up and maintenance time was almost an hour and a half less;
Manual start-up time requirements were 28 minutes, compared to 46 minutes;
From 65% to 69% of samples had a faster turnaround time; and
A system footprint that used 20square feet less space and four fewer analyzers.
Clinical laboratory leaders can review the methodology and results of the Nexus Global report by clicking on this link: www.siemens-healthineers.com/operational.
This article was produced in partnership with Siemens Healthineers.
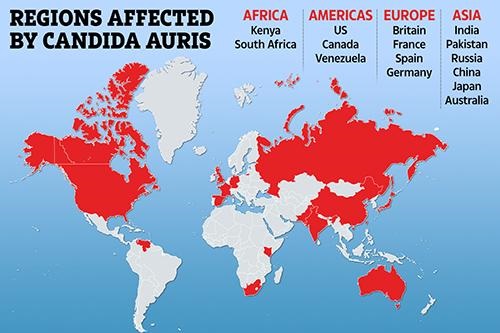
CDC advises clinical laboratories and microbiologists encountering C. auris to follow their own protocols before adopting federal agency guidelines
In July, the Centers for Disease Control and Prevention (CDC) warned healthcare facilities and clinical laboratories to be on the alert for Candida auris (C. auris) infections in their patients. An outbreak of the drug resistant and potentially deadly fungus had appeared in two Dallas hospitals and a Washington D.C. nursing home.
Since those outbreaks, researchers have studied with urgency the “superbug’s” emergence in various types of healthcare facilities around the nation, not just hospitals. Their goal was to discover how it was successfully identified and contained.
“Seeing what was happening in New York, New Jersey, and Illinois [was] pretty alarming for a lot of the health officials in California [who] know that LTACHs are high-risk facilities because they take care of [very] sick people. Some of those people are there for a very long time,” the study’s lead author Ellora Karmarkar, MD, MSc, told Medscape. Karmarkar is an infectious disease fellow with the University of Washington and formerly an epidemic intelligence service officer with the CDC.
“One of the challenges was that people were so focused on COVID that they forgot about the MDROs (multi-drug resistant organisms] … Some of the things that we recommend to help control Candida auris are also excellent practices for every other organism including COVID care,” she added.
According to Medscape, “The OCHD researchers screened LTACH and vSNF patients with composite cultures from the axilla-groin or nasal swabs. Screening was undertaken because 5%–10% of colonized patients later develop invasive infections, and 30%–60% die.
Medscape also reported that the first bloodstream infection was detected in May 2019, and that, according to the Annals of Internal Medicine study, as of January 1, 2020, of 182 patients:
22 (12%) died within 30 days of C. auris identification,
“This is really the first time we’ve seen clustering of resistance in which patients seemed to be getting the infections from each other,” Meghan Lyman, MD, Medical Officer in the Mycotic Diseases Branch of the CDC, told Fox News.
The graphic above illustrates how Candida auris is “spanning the globe,” The New York Times reported. Clinical laboratories that encounter this potentially deadly fungus are advised to contact the CDC immediately for guidance and to take proactive steps to prepare for the “superbug’s” arrival. (Graphic copyright: The Scottish Sun.)
Be More Proactive than Reactive in Identifying C. Auris, CDC Says
C. auris is a type of yeast infection that can enter the bloodstream, spread throughout the body, and cause serious complications. People who appear to have the highest risk of contracting the infection are those:
Who have had a lengthy stay in a healthcare facility,
Individuals connected to a central venous catheter or other medical tubes, such as breathing or feeding tubes, or
Have previously received antibiotics or antifungal medications.
It tends to be resistant to the antifungal drugs that are commonly used to treat Candida infections.
It can be difficult to identify via standard laboratory testing and is easily misidentified in labs without specific technology.
It can quickly lead to outbreaks in healthcare settings.
“With all this spread that we’ve been seeing across the country we’re really encouraging health departments and facilities to be more proactive instead of reactive to identifying Candida auris in general,” Lyman told STAT. “Because we’ve found that controlling the situation and containing spread is really easiest when it’s identified early before there’s widespread transmission.”
There continues to be concerns over this highly drug-resistant infection among hospital physicians and medical laboratories. “Acute care hospitals really ought to be moving toward doing species identification of Candida from nonsterile sites if they really want to have a better chance of detecting this early,” Dan Diekema, MD (above), an epidemiologist and clinical microbiologist at the University of Iowa, told Medscape. (Photo copyright: University of Iowa.)
Candia Auris versus Other Candida Infections
C. auris can cause dangerous infections in the bloodstream and spread to the central nervous system, kidneys, liver, spleen, bones, muscles, and joints. It spreads mostly in long-term healthcare facilities among patients with other medical conditions.
The symptoms of having a Candida auris infection include:
Fever
Chills
Pain
Redness and swelling
Fluid drainage (if an incision or wound is present)
General feeling of tiredness and malaise
C. auris infections are typically diagnosed via cultures of blood or other bodily fluids, but they are difficult to distinguish from more common types of Candida infections, and special clinical laboratory tests are needed to definitively diagnose C. auris.
Whole-genome Sequencing of C. Auris and Drug Resistance
The CDC conducted whole-genome sequencing of C. auris specimens gathered in Asia, Africa, and South America and discovered four different strains of the potentially life-threatening Candida species. All four detected strains have been found in the United States.
There are only three classes of antifungal drugs used to treat Candida auris infections:
However, 85% of the infections in the US have proven to be resistant to azoles and 38% are resistant to polyenes. Patients respond well to echinocandins, but more effective therapies are needed especially as some isolates may become resistant while a patient is on drug therapy, STAT reported.
“Even while it might be susceptible upfront, after a week or two of therapy, we may find that the patient has an infection now caused by an isolate of the same Candida auris that has become resistant to the echinocandins and we are really left with nothing else,” Jeffrey Rybak, PhD, PharmD, Instructor, Department of Pharmaceutical Sciences, St. Jude Children’s Research Hospital, told Infection Control Today.
Although relatively rare, C. auris infections are on the rise. The good news is that there may be further pharmaceutical help available soon. New antifungal agents, such as Ibrexafungerp (Brexafemme) show promise in fighting C. auris infections, but more research is needed to prove their efficacy.
What Should Clinical Laboratories Do?
The CDC stresses that clinical laboratories and microbiologists working with known or suspected cases of Candida auris should first adhere to their own safety procedures. The CDC issued guidelines, but they are not meant to supersede the policies of individual labs.
The CDC also recommends that healthcare facilities and clinical laboratories that suspect they have a patient with a Candida auris infection immediately contact the CDC and state or local public health authorities for guidance.
VA Office of Inspector General recommends changes in management processes after doctor is sentenced to long federal prison term
In a compelling report, the US Department of Veterans Affairs (VA) Office of Inspector General (OIG) found that a host of management failures and “deficiencies in the facility’s quality management processes” at an Arkansas VA hospital contributed to “thousands of diagnostic errors” throughout the tenure of the facility’s Chief of Pathology and Laboratory Medical Services Robert Morris Levy, MD.
“Any one of these breakdowns could cause harmful results,” the report states. “Occurring together and over an extended period of time, the consequences were devastating, tragic, and deadly.”
The OIG report’s findings on how hospital and laboratory administrators dealt with Levy over the years of his employment at the Fayetteville VA Medical Center demonstrate why clinical and pathology lab leaders need to be constantly vigilant in how various quality and compliance procedures are administered in their laboratories. When people and processes are not meeting acceptable standards, it is patients who are at risk of being harmed.
In January, the federal court in Arkansas sentenced Levy to “240 months in federal prison, followed by three years of supervised release and ordered [him] to pay $497,745.70 in restitution for one count each of mail fraud and involuntary manslaughter,” according to court documents.
In its coverage of the federal case against Robert Morris Levy, MD (above in a jailhouse photo), former Chief of Pathology and Laboratory Medical Services at the Fayetteville VA Medical Center, The Washington Post wrote, “Levy’s supervisors failed to heed early warnings that he was endangering patients and then were slow to act, according to internal VA documents, court filings, and interviews with 20 congressional officials, veterans and current and former VA employees.” Clinical laboratory managers and hospital pathologists would be well advised to study the VA’s conclusions in its recent report. (Photo copyright: The Washington Post.)
VA Pathologist ReceivedMultiple Suspensions, then Termination
Following his removal in April 2018, the OIG assembled a team of pathologists to review nearly 34,000 cases interpreted by Levy since he began working at the VA hospital. They identified more than 3,000 errors, of which 589 were classified as “major diagnostic discrepancies” potentially having a negative impact on patient care.
Of the 589, 34 were deemed serious enough to require institutional disclosures, defined as a discussion with the patient or the patient’s representative revealing “that an adverse event has occurred during the patient’s care that resulted in or is reasonably expected to result in death or serious injury.”
The OIG report cited at least two deaths likely resulting from misdiagnoses.
Levy’s hospital privileges were initially suspended in March 2016 following a blood alcohol test indicating he was legally intoxicated while at work. He was reinstated about six months later after completing a treatment program and agreeing to submit to random drug testing.
His privileges were suspended again in October 2017 after he showed signs of impairment during a hospital committee meeting. He was terminated in April 2018 after he was arrested for allegedly driving while intoxicated (DWI) during work hours.
Federal Court Indicts Levy on Multiple Counts
Shortly after the OIG team began reviewing Levy’s cases, a separate OIG group launched a criminal investigation. Levy admitted to investigators that he had been an alcoholic for 30 years, the report stated, and that he had “purchased a substance, 2-methyl-2-butanol (2M2B), online that could be ingested, was similar to alcohol but more potent, and was not detectable using routine drug and alcohol testing methods.”
Citing the federal indictment, the OIG report noted that Levy passed 42 drug and alcohol tests following his reinstatement at the hospital in 2016.
In August 2019, federal authorities charged Levy with three counts of involuntary manslaughter along with multiple counts of wire fraud, mail fraud, and making false statements. The wire and mail fraud charges were related to his 2M2B purchases.
Levy pleaded guilty in June 2020 and was sentenced on January 22, 2021. In addition to the 20-year prison term, he was ordered to pay approximately $498,000 in restitution to VA. The OIG report noted that Levy has appealed the sentence.
And in “Arkansas Pathologist Faces Three Manslaughter Charges,” Dark Daily’s sister publication, The Dark Report, noted that “The outcome of [the Levy] case could be a precedent that gives other prosecutors the confidence that they can file criminal charges in cases where evidence shows that a pathologist’s actions contributed to diagnostic errors that directly contributed to the death of one or more patients.”
“This sentence should send a strong message that those who abuse their positions of trust in caring for veterans will be held accountable,” said VA Inspector General Michael J. Missal in a federal Department of Justice (DOJ) press release. “Our thoughts are with all those harmed by Dr. Levy’s actions, and we hope they find some small measure of comfort from what happened here today.” (Photo copyright: Military Times.)
OIG Finds Numerous ‘Deficiencies in Quality Management’
In its report, OIG found deficiencies in quality management going back to Levy’s original appointment as Pathology and Laboratory Medical Services Chief.
He was initially hired in September 2005 as a locum tenens (temporary) provider and appointed as full-time service chief a month later. This was despite a DWI conviction from 1996 and a stay of only eight months with his previous employer.
Neither would have barred the doctor as a potential candidate; however, the OIG report states, “the OIG is concerned that a rigorous process was not in place to better evaluate his clinical competency at the time he was hired.”
And that was just the beginning.
In his role as service chief, Levy was responsible for the Path and Lab quality management program with assistance from a subordinate staff pathologist, “which made the process susceptible to subversion,” the report states.
The VHA requires a second pathologist to review certain findings, such as diagnosis of a new cancer malignancy. But in some cases, “it was determined that Dr. Levy was entering concurrence statements into some patients’ electronic health records (EHR) when a second pathologist had not agreed with the interpretation or diagnosis,” the OIG report states.
In addition, second reads sometimes “were communicated by sticky notes, which provided Dr. Levy the opportunity to alter or ignore the results,” the OIG reported.
Inherent Conflict of Interest, Fear of Reprisals, and OIG Recommendations
The periodic privileging process, which grants ongoing hospital privileges, was based in part on a “10% peer review” conducted by the staff pathologist. “The involvement of a subordinate in the peer review process of a supervisor creates an inherent conflict of interest,” the OIG report stated. And in some cases, appraisals of the doctor’s competence came from non-pathologists.
The OIG report suggested that the Veteran’s Health Administration (VHA) re-examine its guidance on the peer review, which requires cases to be randomly selected. Instead, the report suggests that targeting specific kinds of cases, such as those with higher risk of interpretation error, could be more effective in analyzing a pathologist’s performance.
The OIG report also noted failures in dealing with the doctor’s impairment and fostering a “culture of accountability.” Hospital staff, apparently, reported signs of impairment as early as 2014, including incidents when the doctor smelled of alcohol and displayed hand tremors. But hospital leadership failed to “vigorously address allegations of impairment,” the OIG report states. And in interviews with the OIG, some staffers expressed fear of reprisal if they reported what they saw.
The OIG report offers 10 recommendations to the VA, including practices related to hiring processes, the 10% peer review, and alcohol and drug testing. It makes two additional recommendations to the director of the Ozarks VA health system: one related to the credentialing processes and the other aimed at ensuring staff and patients can report concerns without fear of reprisal.
Clinical laboratory managers and hospital pathologists may want to review these recommendations and consider the value of applying them in their own practices.
Though clinical laboratory RT-PCR tests remain the ‘gold standard’ when diagnosing COVID-19, at-home antigen tests offer convenience and quick test results. But are they accurate?
Clinical laboratory and pathologists generally acknowledge that RT-Polymerase Chain Reaction (RT-PCR) tests remain the preferred method for detecting COVID-19 disease. However, according to Popular Science, rapid at-home antigen tests that accurately identify people carrying larger loads of the virus are becoming important tools in the fight against spread of the coronavirus.
DxTerity SARS-CoV-2: This saliva-based collection kit is available on Amazon and at Walmart for $110. Specimens must be sent via FedEx on the same day as collection. Results are available within 24 to 72 hours of the sample being received by the PCR testing lab.
Lucira Check It COVID-19 Test Kit: Billed as offering “PCR quality molecular accuracy,” this nasal swab test costs $55 and provides results in 30 minutes or less.
Abbott BinaxNOW Antigen Self-Test. Results within 15 minutes and available for $23.99 at major pharmacies. Each box includes two nasal swab tests, with the second test taken within 36 hours of the first.
Pixel COVID-19 At-Home Collection Kit: This nasal-swab-based mail-in collection kit is available online for $119. Results delivered within 24 to 48 hours of the sample being received by Labcorp.
Many of the newest at-home tests not only have users collect their own swab or saliva samples, but some also provide results in less than an hour, which can be sent to the user’s smartphone. Conversely, home-based collection kits that are returned to clinical laboratories for testing can take 48 hours or longer for shipping and processing.
The FDA’s emergency use authorization announcement (EUA) for Ellume’s $38.99 COVID-19 At Home Test (above) states the test “is a rapid, lateral flow antigen test, a type of test that runs a liquid sample along a surface with reactive molecules. The test detects fragments of proteins of the SARS-CoV-2 virus from a nasal swab sample from any individual two years of age or older.” Ellume’s self-collection test was the first such test to receive an FDA EUA for use without a physician’s order. (Photo copyright: Ellume).
Among the issues cited were the potential for inadequate samples and improper handling to cause inaccurate results, as well as uncertainty whether at-home antigen tests will pick up on COVID-19 variants.
At-home tests also are less likely to be covered by insurance, MedPage Today reported.
During the CAP virtual media briefing, pathologist Kalisha Hill, MD (above), Chief Medical Officer and Chair, Department of Pathology and Medical Director, Laboratory Services, at AMITA Health St. Mary’s Kankakee (Ill.), said, “The gold standard is still a laboratory-performed real-time PCR test and that is the most sensitive and most accurate that we do that is very specific for COVID-19.” Hill called at-home tests a “good screening tool,” but she noted, “You’re testing that moment, that day, and as soon as you leave your home or come in contact with someone else, you could potentially be COVID positive. It’s also important to recognize that when you’re collecting a sample yourself, you may not be able to obtain enough sample for an accurate result … It’s very important how it is collected and also the sensitivity and specificity of the test,” she added. (Photo copyright: AMITA Health/LinkedIn.)
How Do the Tests’ Accuracy Compare?
The Quest Direct and LabCorp Pixel tests—both of which are sent to company labs for PCR testing—scored highest on the two main statistical measures of performance sensitivity (positive percent agreement) and specificity (negative percent agreement). According to Popular Science, each of these tests’ sensitivities and specificities are close to 100%.
According to the websites of the other tests reviewed by Popular Science:
DxTerity test, which uses a saliva sample—97.2% sensitivity and a 92.5% specificity.
BinaxNOW test—84.6% sensitivity and 98.5% specificity.
Cue COVID-19 test—98.7% sensitivity and 97.6% specificity.
Lucira Check Its test—98% accuracy.
Ellume test—95% sensitivity and 97% specificity.
Rapid Antigen Tests Accurate and Easy to Use, says Popular Science
Popular Science found the tests generally easy to use and concluded they are a beneficial—if imperfect—tool in the fight against COVID-19.
“If you’re unvaccinated and symptomatic, they’re a great way to confirm a COVID-19 infection without risking a trip out of the house,” Popular Science stated in its article. “If you’re unvaccinated and have no symptoms, and just want to know whether you can safely attend a family dinner or soccer game, an at-home test remains an imperfect way of self-screening. Remember: If the test comes back negative, there’s still the chance the result is false, and you could accidentally expose others by being within six feet of them without a mask on.”
As the popularity of at-home COVID-19 tests increases, clinical laboratories that perform RT-PCR tests may want to keep a watchful eye on the demand for at-home rapid antigen testing, especially now that some tests are available without prescription.
New USPSTF guidelines suggest reducing the volume of Vitamin D deficiency testing in the general population, which could reduce revenue for clinical laboratories
From 2005 to 2011, the volume of clinical laboratory tests for Vitamin D soared nationally as more doctors tested more patients for Vitamin D deficiency. This became a major source of revenue growth for many clinical laboratories performing those tests. But at least a portion of lab revenue associated with Vitamin D testing may be in jeopardy.
In a recommendation statement published in JAMA Network, titled, “Screening for Vitamin D Deficiency in Adults,” the United States Preventive Services Task Force (USPSTF)—following up on its 2014 recommendations—stated “that the current evidence is insufficient to assess the balance of benefits and harms of screening for Vitamin D deficiency in asymptomatic adults.”
The USPSTF’s new recommendations concerning Vitamin D testing came after the federal task force performed an extensive review of the benefits and potential harm of screening for Vitamin D deficiencies in non-pregnant adults who displayed no symptoms of a deficiency. Symptoms of a Vitamin D deficiency include fatigue and tiredness, bone and back pain, depression, impaired would healing, bone loss, hair loss, and muscle pain.
After completing its research, the USPSTF concluded “the overall evidence on the benefits of screening for Vitamin D deficiency is lacking. Therefore, the balance of benefits and harms of screening for Vitamin D deficiency in asymptomatic adults cannot be determined.”
Are USPSTF Conclusions Contrary to Current Deficiency Testing Practices?
“Among asymptomatic, community-dwelling populations with low Vitamin D levels, the evidence suggests that treatment with Vitamin D has no effect on mortality or the incidence of fractures, falls, depression, diabetes, cardiovascular disease, cancer, or adverse events,” the JAMA Network article states.
Other studies have linked low Vitamin D levels with some health conditions and risks, however, the USPSTF review found no studies that directly evaluated any perks associated with Vitamin D screening in otherwise healthy individuals.
Everyday Health listed 10 illnesses linked to low Vitamin D deficiency. They include:
“We see a lot of associations between Vitamin D deficiency and poor health outcomes,” Mary Byrn, PhD, RN, an associate professor at Loyola University in Chicago who studies Vitamin D, told Everyday Health. “Although these are relationships and we are unable to conclude cause and effect, taking Vitamin D supplements or exposing yourself to the sun in a safe manner to increase Vitamin D naturally are easy ways to improve your health and try to reduce your risk of multiple diseases,” she said. (Photo copyright: Midwest Nursing Research Society.)
Can Vitamin D Supplementation Be Harmful?
The USPSTF study also stated that Vitamin D supplementation appears to be safe and that toxicity from too much Vitamin D would be rare. One of the USPSTF’s key concerns of screening for Vitamin D in asymptomatic individuals was the potential for misclassification and inaccurate diagnoses.
The study also revealed that more research is needed to determine what serum levels are optimal when diagnosing a Vitamin D deficiency, and whether those levels vary by subgroups, such as race, ethnicity, or gender.
The JAMA Network article states that “the evidence is inconclusive about the effect of treatment on physical functioning and infection.”
The amount of Vitamin D individuals need each day depends upon their age. The National Institutes of Health (NIH) recommends that adults between the ages of 19 and 70 get 15 micrograms or 600 International Units (IU) of Vitamin D daily.
According to an NIH fact sheet, people can receive Vitamin D through sun exposure, supplements, and some food, such as fatty fish, mushrooms, beef liver, cheese, and egg yolks, plus foods that are fortified with Vitamin D, such as some milk products and breakfast cereals.
Vitamin D and COVID-19
It has been widely reported that approximately 42% of Americans are Vitamin D deficient. And Vitamin D deficiency has been linked to an increased risk of contracting the SARS-CoV-2 coronavirus and how well patients recover after COVID-19 treatment.
A study published in the Journal of Clinical Endocrinology and Metabolism that examined 216 COVID-19 hospitalized patients in Spain found that over 80% of those individuals were deficient in Vitamin D. The study also found that COVID-19 patients who had lower Vitamin D levels also had a higher number of inflammatory markers that have been associated with poorer COVID-19 outcomes. The results of this study were in March.
For several decades, experts have recommended avoiding sun exposure and using sunscreen to avoid skin cancers. This may have caused people to get less Vitamin D from sun exposure. It may also have contributed to an increase in the number of Vitamin D deficiencies and increased COVID-19 infections.
Pathologists and clinical laboratory managers should keep in mind that the USPSTF recommended less testing for Vitamin D deficiencies in asymptomatic individuals. This proposal may affect test volume in clinical laboratories, as Vitamin D testing has been a common and lucrative assay for many years.
Cozy relationships between hospital chief executives and healthcare companies they do business with may raise ethical questions
If hospital employees, including pathologists, wonder why their hospital uses a certain company’s products and services it may be because their Chief Executive Officer (CEO) sits on the Board of Directors of the same companies from which the hospital buys products and services. That’s the suggestion in a recent Boston Globe investigative report.
In “Boston’s Hospital Chiefs Moonlight on Corporate Boards at Rates Far Beyond the National Level,” The Boston Globe reported that, in Boston, hospital CEOs at the city’s academic medical centers frequently sit on the boards of healthcare companies with which their hospitals do business. However, because the investigative reporters did not list the healthcare companies which had Boston hospital CEOs as board members, clinical laboratory managers and pathologists cannot determine from the article if their medical laboratories are using products from those same companies.
According to The Globe, five of seven CEOs and Presidents of Boston’s major teaching hospitals also receive compensation for serving as directors of publicly traded companies. And in their roles as corporate board members, hospital CEOs often receive stock in these companies, making the value of their remuneration potentially worth millions of dollars, The Globe reported.
Not Illegal, But Is It Ethical?
The Boston Globe’s investigation noted that such moonlighting, while not unheard of elsewhere in the country, is commonplace in Boston, raising ethical concerns despite conflict-of-interest policies aimed at limiting outside relationships.
“Hospitals in Boston and elsewhere that allow this outside corporate work do so under the terms of conflict-of-interest policies,” The Globe reported. “A Globe review of more than a dozen hospital conflict-of-interest policies across the country found more similarities than differences. Almost all require hospital trustees to approve a hospital chief’s outside board work and consider certain factors, such as the amount of business a company does with the hospital and time required.
“But the policies offer limited evidence about actual practices,” The Globe added. “Trustees typically retain significant discretion over what is permitted or barred, and their deliberations are generally hidden from the public. It is hard to tell if the relative rarity of hospital chiefs in other cities holding outside directorships is because of a lack of interest or opportunity, or is the result of trustees saying no.”
One of the hospital chief executives The Globe’s investigation highlighted was former-Boston Children’s Hospital CEO Sandra Fenwick. While there, The Globe noted, she also held a seat on the board of for-profit telehealth company Teledoc Health, and during her tenure as Children’s CEO, she lobbied Massachusetts legislators for telehealth funding at the start of the COVID-19 pandemic.
Though no laws were broken, some questioned the ethics of such actions. Nevertheless, The Boston Globe wrote that “Debra O’Malley, a spokesperson for Secretary of State William Galvin’s office, said Fenwick’s actions did not appear to violate the law: She is required to disclose in writing to the state that she is a lobbyist for the hospital and the bills she lobbied on, which she did, O’Malley said. That information is publicly available.”
And though The Globe reported that Boston Children’s Hospital had “declined to answer detailed questions about [Fenwick’s] lobbying efforts,” the paper wrote that a hospital spokesperson said, “[Fenwick’s] directorships are publicly disclosed in filings with the Securities and Exchange Commission.”
Fenwick retired from Boston Children’s Hospital in March 2021. The Globe noted that at that time her Teledoc Health stock, which was compensation for her board work, was worth $8.8 million. Additionally, she had been paid $2.7 million annually as CEO of Boston Children’s Hospital.
“It does seem like buying influence and it’s hard to imagine what else it would be,” Carl Elliott, MD, PhD (above), Professor in the Center for Bioethics and the Department of Pediatrics at the University of Minnesota told BioPharma Dive. “If you’re actually trying to buy scientific knowledge, then you wouldn’t really be going after CEOs. What they have is power.” (Photo copyright: Boston University.)
Avoiding Conflicts of Interest
Bad optics created by a Boston hospital CEO receiving seven-figure compensation for serving on the board of directors of a publicly traded company is not new. In July 2020, former Brigham and Women’s Hospital President Elizabeth Nabel, MD, resigned from the board of biotech company Moderna (NASDAQ:MRNA) “to alleviate any potential concern about the conduct or the outcome of the COVID-19 vaccine trial when Brigham and Women’s Hospital was identified by NIH as one of the clinical sites for the Phase 3 trial,” a Moderna press release states.
On March 1, 2021, Nabel also stepped down as Brigham and Women’s Hospital president. She then rejoined the Moderna board of directors on March 10, 2021, the press release noted.
In a STAT editorial, titled, “Hospital CEOs, Med School Leaders Shouldn’t Sit on For-Profit Health Care Company Boards,” endocrinologist and former Dean of Harvard Medical School Jeffrey Flier, MD, wrote, “As dean, I vigorously supported the value of robust interactions between faculty and industry to advance innovation and human health, and still do. In my current status as a professor of medicine at Harvard, I serve on several for-profit and not-for-profit boards. I learn from this work, and I believe I am making useful contributions as a board member. But I also believe that the considerations governing such relationships should be judged differently for institutional leaders.”
Flier maintains there are multiple reasons why hospital and medical school leaders should not sit on for-profit boards despite the expertise they bring to the table, including:
The time commitment required,
The “extraordinary compensation packages” they receive in their full-time jobs,
The potential for complicated “business intersections,” and
The risks to an “institution’s reputation for integrity.”
“I recommend that hospital CEOs and academic leaders at the level of Deans and Presidents devote their full attention to their well-compensated day jobs and defer positions on the boards of for-profit companies—and the unavoidable conflicts they raise—to the post-leadership phase of their careers,” Flier wrote.
While cozy relationships between hospital and academic medical center leaders and for-profit healthcare companies may not directly impact hospital pathologists and staff, it is worth staying aware of potential conflicts of interest.