Acceptance of digital pathology and whole-slide imaging is now almost universal among academic health center pathology departments and the nation’s largest pathology companies
Across the United States, many private practice anatomic pathology groups now recognize that digital pathology is the path forward for the entire profession. During the past decade, most academic pathology departments and large pathology lab companies have incorporated digital pathology (DP) and whole-slide imaging (WSI) into many of their labs’ daily activities.
However, in community hospital-based anatomic pathology groups, there have been barriers to even the partial adoption of digital pathology. The two biggest barriers are well-known and discussed frequently at conferences and in the literature.
Some Pathologists Reluctant to Give Up Light Microscopes
One recognized barrier to wider adoption of DP is the reluctance of many long-serving pathologists to give up their familiar light microscopes and glass slides so they can make the transition to reading pathology images on a computer screen. These pathologists remain loyal to the tools and workflows that have served them well throughout their careers.
They generally oppose their group’s move to digital pathology when the subject is discussed in partner meetings and strategic retreats. Since many pathology groups require 100% of partners or shareholders to approve major business decisions, even one recalcitrant and stubborn pathologist-partner can block the motion to adopt digital pathology that is supported by most partners.
The second barrier is the fully-loaded cost to acquire, validate, implement, and use a digital pathology system with whole-slide imaging. A full-featured scanner can cost $250,000 or more and acquiring all the software, systems, and tools needed by a group to fully incorporate digital pathology into daily workflow can easily total $500,000 to $1,000,000.
This substantial commitment of a pathology group’s capital can trigger the same intense debates as the original question of whether the pathologists in the group should adopt DP and WSI. And, not surprisingly, in most pathology groups the same dynamics come into play when votes are tallied on the motion for the pathology group to commit the funds necessary to acquire a digital pathology system, the scanners, and associated tools.
Just one or two partner holdouts can block the decision to spend the money, despite that most of the pathologist partners are ready to make the commitment.
More Community Pathology Groups Considering Digital Pathology
Yet, the momentum in favor of adopting DP and WSI continues to build. “Those pathology labs that are early adopters report multiple clinical and financial benefits. These can include generating positive financial outcomes—including the ability to attract new clients, increasing case referrals, and generating new sources of revenue to the group. In turn, the increased revenue can allow the group to increase pathologist compensation,” said Robert L. Michel, Editor-in-Chief of Dark Daily and its sister publication The Dark Report.
Every day, more anatomic pathologists in the United States use a digital pathology system with a workstation (like above) to view whole-slide images and manage their daily caseload. Most academic center pathology departments use digital pathology, as do many of the nation’s largest pathology lab companies. (Photo copyright: WizardHealth.)
“We are in a time when health insurers are hammering away at the reimbursement paid to anatomic pathologists,” Michel continued. “Year after year, payers cut reimbursement for technical component and professional component services. They exclude many pathology groups from payer networks. That is why more community pathology groups are recognizing several important benefits with the use of DP and WSI that can increase a pathology group’s revenue and boost its pathologist compensation.
Community Pathology Groups Can Use Digital Pathology to Add Value
Equally important, there are specific ways that digital pathology and whole-slide imaging increase the value of the clinical services pathologists deliver to their client physicians. These dual benefits of DP are often overlooked—or not discussed—when community pathology groups conduct their annual retreats and debate the key points of when to adopt—and how to fund—a digital pathology system for their group. These benefits range from giving physicians a faster diagnostic answer on their cancer cases to helping the group’s subspecialist pathologists get more case referrals from physicians in other states.
“It’s important for all surgical pathologists to recognize several realities in today’s pathology marketplace,” Michel noted. “First, almost every sector in healthcare is digitizing itself. Reinforcing this trend is the federal government’s mandates for interoperability across EHRs, HISs, and LISs. Any private pathology group practice that lags in its adoption of digital capabilities and digital images will find itself falling farther and farther behind as physicians switch their case referrals to other pathology labs that have converted to digital pathology and whole-slide images.
“Second, pathology groups that adopt DP and WSI put themselves in a position to build market share in their service region, while at the same time increasing case referrals for their in-house subspecialist pathologists from throughout the United States,” Michel continued. “Also, when the histology is done locally, the local pathology group can deliver faster diagnostic answers and provide digital images as appropriate to referring physicians and hospitals in that region without the need to transport glass slides by couriers.
“Third—and this is an often-overlooked benefit of digital pathology—the local pathology group with DP and WSI can recruit today’s graduating pathology residents and fellows who have trained on DP and WSI. These new pathologists typically limit their job search to pathology groups that have gone digital,” Michel noted. “Millennial pathologists trained with digital images in their residency program. They are eager to work with the automated image analysis algorithms now coming to market.”
On Thursday, May 27, at 1:00 PM EDT, Keith Kaplan, MD, Chief Medical Officer of Corista (left), Andrew Evans, MD, Medical Director of Laboratory Medicine at Mackenzie Health (center left), William DeSalvo, President of Collaborative Advantage Consulting and Manager of Histology Operations at Sonora Quest Laboratories in Tempe, Ariz. (center right), and Lisa-Jean Clifford, COO and Chief Strategy Officer at Gestalt Diagnostics (right) will present “Adopting Digital Pathology on a Budget: Getting Started, Knowing What’s Feasible, and Funding Your DP from Overlooked Sources.” Anatomic pathologists, clinical laboratory directors, laboratory managers, clinical pathologists, and laboratory technicians will gain a critical understanding of which components a fully integrated digital pathology system requires, the differences between your lab’s existing LIS and a digital pathology system, budget-minded approaches to buying the components of a digital pathology system and implementing them in a stepwise fashion, and much more! (Photo copyright: Dark Daily.)
Recognizing the significant capital investment needed to acquire and deploy digital pathology and WSI, one goal of the webinar’s panel of experts is to identify ways that pathology groups can go digital on a budget. “We will do our best to identify different ways that pathology groups with limited financial resources can get into digital pathology,” said Keith Kaplan, MD, Chief Medical Officer at Corista in Concord, Mass., who will chair the upcoming webinar. “This may be the first public presentation where there is candid information about different financial strategies that your pathology group can utilize to acquire the scanners, the DP systems, and the associated tools needed for a full conversion to daily digital pathology.”
Don’t overlook how your participation in this webinar can be the foundation for helping your pathology group practice develop a timely, cost-effective path forward to introduce digital pathology and whole-slide imaging. Use of DP and WSI can become an important factor in helping your group offset payer prices cuts, develop new clients and sources of revenue, and increase pathologist compensation.
Click HERE to register today (or copy and paste this URL into your browser: https://www.darkdaily.com/webinar/adopting-digital-pathology-on-a-budget/). Make sure to have your pathology practice administrator and your histology manager join you for this important webinar.
In a letter, Congress urged the HHS Secretary to conduct “vigorous oversight and enforces full compliance with the final rule”
Analysis of more than 3,100 hospital websites by The Wall Street Journal (WSJ) has found “hundreds” containing embedded code that prevents search engines from displaying the hospitals’ prices. This is contrary to the Hospital Price Transparency Final Rule (84 FR 65524), passed in November 2019, which requires hospitals to “establish, update, and make public a list of their standard charges for the items and services that they provide,” including clinical laboratory test prices.
“Hundreds of hospitals embed code in their websites that prevented Alphabet Inc.’s Google and other search engines from displaying pages with the price lists,” the WSJ reported. “Among websites where [the WSJ] found the blocking code were those for some of the biggest US healthcare systems and some of the largest hospitals in cities including New York and Philadelphia.”
Additionally, the WSJ found hospitals were finding ways to “hide” the price lists they did display deep within their websites. The prices can be found, but the effort involves “clicking through multiple layers of pages,” on the providers’ websites, the WSJ added.
Lawmakers Put Pressure on CMS
The WSJ report drew the attention of federal lawmakers who weighed in on the current state of hospital price transparency and on the WSJ’s findings in a letter to Xavier Becerra, Secretary of the federal Department Health and Human Services (HHS).
In their letter, members of the Congressional Committee on Energy and Commerce called for HHS “to revisit its enforcement tools, including the amount of civil penalty, and to conduct regular audits of hospitals for compliance.”
Committee members wrote, “The Hospital Price Transparency Final Rule requires hospitals to make public a machine-readable file containing a list of all standard charges for all items and services and to display charges for the hospital’s 300 most ‘shoppable’ services in a consumer-friendly format. We are concerned about troubling reports of some hospitals either acting slowly to comply with the requirements of the final rule or not taking any action to date to comply.”
The letter, which was signed by the committee’s Chairman Frank Pallone (D, New Jersey) and Committee Ranking Member Cathy McMorris Rodgers (R, Washington State), cited the WSJ investigation as well as other analyses of price transparency at US hospitals.
Cynthia Fisher (above), founder of Patient Rights Advocate, told The Wall Street Journal, “In the past there was absolutely no power for the consumer. It was like highway robbery being committed every day by the healthcare system.” Now, Fisher added, “it’s the American consumer who is going to drive down the cost of care.” Clinical laboratories will note that consumer demand for, and federal regulation of, price transparency is not limited to hospitals. All healthcare providers need procedures in place that comply with federal guidelines for transparency. (Photo copyright: Morning Consult.)
Additional Studies Show Major Hospitals “Non-Compliant”
One such study cited by the Congressional committee in its letter to HHS was conducted by Health Affairs, which looked into transparency compliance at 100 hospitals. In a blog post, titled, “Low Compliance from Big Hospitals on CMS’s Hospital Price Transparency Rule,” the study authors wrote “our findings were not encouraging: Of the 100 hospitals in our sample, 65 were unambiguously noncompliant.
“Of these 65,” they added:
“12/65 (18%) did not post any files or provided links to searchable databases that were not downloadable.
“53/65 (82%) either did not include the payer-specific negotiated rates with the name of payer and plan clearly associated with the charges (n = 46) or were in some other way noncompliant (n = 7).
“We are troubled by the finding that 65 of the nation’s 100 largest hospitals are clearly noncompliant with this regulation. These hospitals are industry leaders and may be setting the industrywide standard for (non)compliance; moreover, our assessment strategy was purposefully conservative, and our estimate of 65% noncompliance is almost certainly an underestimate,” Health Affairs concluded.
A previous similar investigation by The Washington Post called compliance by hospitals with the pricing disclosure rules “spotty.”
So, why is complying with the federal price transparency rule so challenging for the nation’s largest hospitals? In its reporting on the Wall Street Journal analysis, Gizmodo wrote, “we’ve seen healthcare providers struggle to implement the new law due, in part, to how damn ambiguous it is. Past reports have pointed out that the vague requirements hoisted onto hospitals as part of these new rules often result in these pricing lists being difficult—if not downright—impossible to find, even if the lists are technically ‘machine-readable’ and ‘on the internet.’”
“Meanwhile,” Gizmodo continued, “as [the WSJ] points out, the order doesn’t specify exactly how much detail these hospitals are even supposed to offer on their pricing sheets—meaning that it’s up to the hospitals whether they want to include rates pertaining to specific health insurance plans, or whether they want to simply include different plan’s rates in aggregate.”
And in their letter to HHS, the Congressional committee wrote, “… some hospitals are providing consumers a price estimator tool instead of providing the full list of charges and payer-negotiated rates in one file, and some are making consumers fill out lengthy forms for estimates. Some hospitals also are providing the data in a non-useable format or failing to provide the codes for items and services.”
Clinical Laboratories Must Comply with Price Transparency Rules
Clearly, transparency in healthcare has a long way to go. Nevertheless, hospital medical laboratory leaders should expect reinforcing guidance from CMS on making price information on commonly used clinical laboratory tests fully accessible, understandable, and downloadable.
As Dark Daily noted in previous coverage, consumer demand for price transparency is only expected to increase. Clinical laboratories need to have a strategy and process for helping consumers and patients see test prices in advance of service.
A New York Times report suggests that frequent testing is still the best approach to controlling spread of the SARS-CoV-2 coronavirus
Many colleges and universities go to great lengths to screen their students for signs of COVID-19 using technologies that include fever scanners, heart-rate monitors, and symptom-checking apps. But a recent report in The New York Times, titled, “Colleges That Require Virus-Screening Tech Struggle to Say Whether It Works,” suggests that academic institutions would be better off adopting frequent clinical laboratory testing for the SARS-CoV-2 coronavirus, even if it is more expensive than symptom screening.
This shouldn’t be a surprise to pathologists and other medical laboratory professionals who have followed news and research about the pandemic. Back in Sept. 2020, the federal Centers for Disease Control and Prevention (CDC) in a media statement noted that “symptom-based screening has limited effectiveness because people with COVID-19 may have no symptoms or fever at the time of screening, or only mild symptoms.”
That same month, Medscape reported that presidential advisor Anthony Fauci, MD, said, “It is now clear that about 40%-45% of infections are asymptomatic.”
But this hasn’t prevented educational institutions from investing in costly screening technologies. One cited by The New York Times (NYT) was the University of Idaho, where 9,000 students live on or near campus. The university has spent $90,000 on fever scanners resembling airport metal detectors, the paper reported, but as of early March, the units had identified fewer than 10 people with high skin temperatures.
“Even then, university administrators could not say whether the technology had been effective because they have not tracked students flagged with fevers to see if they went on to get tested for the virus,” the NYT reported, adding that many other institutions that adopted screening technologies have failed to systematically measure the effectiveness of these approaches.
“The moral of the story is you can’t just invest in this tech without having a validation process behind it,” infectious-disease epidemiologist Saskia Popescu PhD, MPH, of George Mason University told The New York Times.
Rising COVID-19 Infections on College Campuses
These efforts have come amid increasing COVID-19 infection rates on many US campuses. In “Cases Rise, Restrictions Begin,” Inside Higher Ed reported that large universities were doing better than they had in the fall 2020 semester, but that “other campuses—including those that kept cases low in the fall—are seeing numbers rise.” One such campus was Boston College, which cast blame on students who were not following safety protocols.
For its story, The New York Times surveyed more than 1,900 US colleges and universities as part of an effort to track outbreaks on campus. Respondents reported more than 120,000 campus-related COVID-19 cases between Jan. 1 and March 2, 2021, but because institutions measure outbreaks in different ways, the NYT reported that this is likely an undercount. Overall, institutions reported more than 535,000 cases since the pandemic began, according to the survey.
Clinical Laboratory Testing Still Ongoing on College Campuses
School administrators told The New York Times that despite questions about the usefulness of screening tools, this approach is still worthwhile as reminders for students to follow other protocols, such as mask wearing.
And universities have not abandoned testing for COVID-19. For example, The New York Times noted that students at the University of Idaho are tested at least twice each semester, and the school is also testing wastewater to identify outbreaks of SARS-CoV-2.
The Ohio State News, a publication of Ohio State University, reported in late February that it had tested 30,000 people in a single week, accounting for 12% of the COVID-19 tests conducted in Ohio. At the start of the fall semester, the university was sending test samples to a private company in New Jersey, but later it began processing samples at the on-campus Applied Microbiology Services Lab (AMSL).
“By the start of spring semester, the AMSL was processing about 85% of Ohio State’s COVID-19 tests,” the university reported, for a likely savings of $30 million to $40 million. Leaders of the testing program expect that they can realistically conduct 35,000 tests per week.
Chris Marsicano, PhD (above), a professor and researcher at Davidson College, told Inside Higher Ed that many institutions are relying on antigen testing, which is less costly but also less reliable than PCR (polymerase chain reaction) tests. “PCR tests are expensive,” he said. “Just because you’re testing multiple times a week doesn’t mean you’re catching all the cases.” Marsicano leads the institution’s College Crisis Initiative. Clinical laboratory leaders can attest to Marsicano’s statement. (Photo copyright: Twitter.)
Using Technology for COVID-19 Contact Tracing
In addition to symptom screening, some universities have adopted technologies that track student movement on campus for contact-tracing purposes. But again, the benefits are questionable. For example, Bridgewater State University in Bridgewater, Mass. asked students to scan QR codes at various locations, but only one-third were doing so, The New York Times reported. Another system at the university records entry to campus buildings when students swipe their IDs.
“We found what we need is tests and more tests,” clinical psychologist Christopher Frazer, Psy.D., Executive Director of the university’s wellness center, told The New York Times. He said that students on campus are tested once a week. When they have tested positive, contact tracers “often learned much more about infected students’ activities by calling them than by examining their location logs,” the NYT reported.
Colleges and universities are also banking on vaccination to reduce the spread of the virus, Inside Higher Ed reported. Some will require all students to be vaccinated for the fall semester, but such mandates are facing legal and political hurdles. For example, executive orders by Texas Governor Greg Abbott and Florida Governor Ron DeSantis may prohibit institutions in those states from imposing vaccination requirements.
As colleges and universities struggle to deal with the challenges of COVID-19, clinical laboratories have resources for staying up to date on current testing and tracking technologies in use on campuses. For example, the CDC is funding a program to facilitate sharing of best practices and other information. Inside Higher Ed reported that the Higher Education COVID-19 Community of Practice (CoP) will include a discussion board, webinars, and a searchable database of info uploaded by participating institutions.
But information blocking remains a barrier to complete information exchange, creating ongoing issues for clinical laboratories and pathology groups
Interoperability of electronic health records (EHRs) remains one the biggest challenges for clinical laboratories and anatomic pathology groups that must interface with the EHRs of their physician clients to enable electronic transmission of medical laboratory orders and test results.
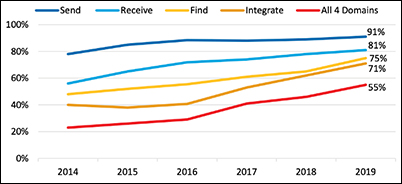
Laboratory professionals will be pleased to know the most recent federal government report on hospital interoperability shows 55% of all hospitals can now send, receive, find, and integrate patient information from outside sources into their EHRs. This is an important milestone on the road to robust data exchange.
About 70% of hospitals reported integrating data into their EHR—a nearly 15% increase from 2018.
A majority of hospitals used a mix of electronic and non-electronic methods to exchange summary of care records. However, use of electronic third-party methods, Health Information Service Providers (HISPs), health information exchange (HIE), and vendor networks increased in 2019.
The proportion of hospitals that used a national network to find (or query) patient health information increased by nearly 40% between 2018 and 2019.
The graphic above taken from the ONC report shows the “percent of US non-federal acute care hospitals that electronically find patient health information and send, receive, and integrate patient summary of care records from sources outside their health system from 2014-2019. About 70% of hospitals reported integrating data into their EHR—a nearly 15% increase from 2018.” This is a positive development for clinical laboratories and anatomic pathology groups, because it makes it easier for them to accept electronic medical laboratory test orders and report test results electronically. (Graphic copyright: Office of the National Coordinator of Health Information Technology.)
David Burda, creator and leader of 4sight Health, a thought leadership and advisory company, has been a forceful advocate for healthcare interoperability, routinely stressing that patients cannot receive the optimum level of care from their providers as long as EHR vendors and health systems engage in information blocking.
In a blog post, Burda commented on the ONC report and outlined how far there still is to go. “Hospitals passed an important interoperability milestone in 2019, but the goal of reaching total hospital interoperability is still ways off.
“To be fair,” he added, “there were some other signs of progress in the new ONC report. The most significant, from a patient’s point of view, was the fact that in 2019, more hospitals were actively seeking patient health information from other providers and sources as part of how they routinely diagnose and treat patients. They’re not passively relying on data in their own EHR systems to make medical decisions.”
For example, Burda wrote:
73% of the hospitals said they struggle with exchanging patient information with other providers who use a different EHR system.
66% of the hospitals said they share patient information with other providers who don’t share patient health information with them.
59% of the hospitals said other providers’ EHR systems don’t have the capability to receive patient health information from them.
“These [issues] are all caused by cultural, financial, and technical barriers that should have fallen years ago,” wrote David Burda (above), news editor and columnist for 4sight Health in his blog post about the ONC interoperability report. “But they didn’t, and all we can do is keep pushing forward to the day patient health data stops being a closely guarded commodity and starts flowing freely throughout the delivery system to drive better care for patients.” Clinical laboratory test results, being the largest portion of data contained in electronic health records, would make up a significant portion of the health data Burda is referring to. (Photo copyright: 4sight Health.)
KLAS and CHIME are Optimistic about EHR Interoperability
Industry progress toward interoperability was also noted in a white paper titled, “Trends in EMR Interoperability,” co-authored by KLAS Research and the College of Healthcare Information Management Executives (CHIME). The authors found reasons for optimism, noting the rate of provider organizations achieving “deep interoperability” had doubled since 2017, with roughly two-thirds of provider organizations often or nearly always having access to needed records.
“The overall rate leaves much to be desired, but signs of progress are visible,” the authors wrote. Evidence of that progress includes improved data sharing with outside EHRs, a growing ability for ambulatory clinics and smaller hospitals to connect with larger organizations, and more widespread use of national networks to achieve information sharing.
“Since KLAS’ prior large-scale interoperability study in 2017, the market has made notable progress; access to outside records has increased, provider organizations are connecting to more critical exchange partners than ever, and the use of APIs offers new ways to facilitate data exchange in service of myriad use cases,” the report concludes. “Even with all this progress, there is still a significant opportunity for EMR (electronic medical record) vendors and provider organizations to partner effectively to help data exchange truly impact patient care. With additional work, the industry appears poised for improvement in this area going forward.”
Seema Verma says Interoperability is Improving
In an article she authored for Health IT News, titled, “How CMS Has Made Progress on Healthcare Interoperability,” Seema Verma, Administrator for the Centers for Medicare and Medicaid Services (CMS) during the Trump presidency, noted that great strides have been made in recent years toward the goal of complete interoperability.
“Technology is ever evolving, and our work will constantly evolve, but our efforts have laid a foundation for future policy that will enable the secure and interoperable exchange of healthcare information, drive value-based care in America, and give patients and doctors the information they need,” she wrote.
For clinical laboratories and anatomic pathology groups, the road to interoperability remains littered with a few potholes, but speed bumps are disappearing, which may signal a time in the not-too-distant future when clinical laboratories and pathology groups will easily interface electronically with physicians, hospitals, and other providers to receive test orders and transmit test results.
COVID-19 has made telehealth an important tool. New technologies may help clinical laboratories collect blood samples ordered by physicians treating patients remotely
Even before COVID-19, telehealth services were gaining in popularity. But the SARS-CoV-2 pandemic fully opened the door to widespread use of mobile healthcare (mHealth) technologies. This has had an on-going impact on clinical laboratories.
Pre-pandemic, if a patient visited a healthcare provider and that provider ordered medical laboratory tests, the patient could simply walk down the hall to the lab’s patient service center and provide a blood sample. But when patients and providers meet through telehealth services, it is not so easy for lab personnel to collect samples for testing.
Several questions face healthcare providers and clinical laboratories as the pandemic subsides:
Will telehealth remain popular?
Does it benefit patient care?
Can physicians fit it into their workflows?
Will it continue to be reimbursed fairly?
COVID-19 Gives Telehealth Adoption a Big Boost
Telemedicine became important very quickly as SARS-CoV-2 coronavirus infections spread in early 2020. And not just in the United States. Clinicians worldwide began to embrace mHealth technology as a method of delivering care in a way that reduced the transmission of the virus.
The number of telemedicine consultations has declined since April 2020 but continues to be significantly higher than before the pandemic. It is also interesting to note that 90% of telemedicine visits were by phone in Australia and Canada, according to an article published in JAMA Network, titled, “Paying for Telemedicine After the Pandemic.”
“At its peak in April 2020, telemedicine was responsible for 38% of all ambulatory visits among Australia’s Medicare program, 42% of all ambulatory visits for individuals insured by a US commercial insurer, and 77% of all ambulatory visits among people in Ontario, Canada,” wrote Ateev Mehrotra, MD, MPH (above), Associate Professor of Health Care Policy, Harvard Medical School, and Associate Professor of Medicine and Hospitalist, Beth Israel Deaconess Medical Center (BIDMC), et al, in the Jama Network article. Clinical laboratory testing was part of all of that and continues to find its way in this new world of mobile healthcare. (Photo copyright: Managed Healthcare Executive.)
Telehealth Popular with Community Health Centers but Disparities Remain
One of the big issues with telehealth, according to the NACHC, is that not all patients have access to the technology necessary for telehealth to be a viable alternative to traditional office visits. And that patients who use NACHC clinics tend to be “low income, minority, and uninsured or publicly insured.”
Thus, the NACHC lists “inadequate broadband” as one of the biggest issues regarding the continued use of telehealth. “Patients without reliable internet or the necessary technology still face difficulties accessing services, which has resulted in forgone or delayed care,” the NACHC noted.
A study, titled, “Who Is (and Is Not) Receiving Telemedicine Care During the COVID-19 Pandemic,” published in the American Journal of Preventative Medicine (AJPM), confirms the findings of the NACHC. “The COVID-19 pandemic has affected telehealth utilization disproportionately based on patient age, and both county-level poverty rate and urbanicity.”
Although in-person visits declined by 50%, the AJPM study’s authors noted that telehealth did not completely bridge the gap, particularly in areas where there were higher levels of poverty.
Physician Practices Are Businesses Too
The pandemic hurt businesses of all types, including independent physician’s offices. Approximately 8% of practices closed due to the pandemic, and 4% expect they will shut down within the next year. Along with the financial burden of shutdowns, physicians are burning out, Fast Company reported.
Organizations now have the technology in place and some patients have learned to utilize the service. However, the situation does raise important questions:
Will telehealth remain a critical component of healthcare in the future?
As physician’s offices close, will telehealth fill the gap?
Telehealth and Payment
Becker’s Hospital Review asked nine hospital CIOs if telehealth would “have staying power.” Every executive mentioned either reimbursement or payers in their response. Therefore, whether telehealth remains a viable method of care delivery may depend more on who will pay for it and less on popularity or patient access.
During the COVID-19 pandemic, CMS revised the rules surrounding telehealth. This allowed practitioners to charge the same for telehealth visits as they would for in-person visits. Many private payers followed suit as well. However, those rules were temporary and it is not certain that they will be extended.
“Payers must continue to reimburse for telehealth visits,” Mark Amey, CIO, Alameda Health System, told Becker’s Hospital Review. “This has been approved with emergency orders, but there are questions on whether this will become permanent. The sooner this is addressed and resolved, the sooner organizations can make sure they are investing in permanent—not temporary—solutions.”
Tests that use nasal swabs and saliva have seen an enormous boom thanks to demand for COVID-19 testing that can be done at home, and COVID-19 antibody tests also are in high demand. Additionally, direct-to-consumer (DTC) tests that use blood samples also are seeing advancements. However, none of those factors—not even reimbursement—help medical laboratory managers who are trying to identify new methods of collecting specimens for testing that support telehealth doctors.
“Innovations in blood sample collection are proving their utility and validity just in time for the home-based medicine push,” noted the AACC. The article goes on to describe Mitra microsampling devices, produced by Neoteryx. These devices collect 20 uL of blood via a finger prick and are already used by organ transplant recipients.
Another method involves the use of dried blood spots.
Though COVID-19 is a factor, it is not the only one driving development of new healthcare technologies that may expand options for medical laboratories looking for ways to collect samples remotely.
As the COVID-19 pandemic progresses, we will continue to bring you news about healthcare technology that can enhance clinical laboratories’ ability to collect patient samples, include advancements in remote sampling techniques and technologies.
Oddly, as upcoding severity levels have risen, reported higher-severity inpatient hospital stays have dropped, OIG reported
Medicare upcoding fraud is a growing problem for the federal Centers for Medicare and Medicaid Services (CMS). Now, a report from the US Department of Health and Human Services (HHS) Office of Inspector General (OIG) suggests that the practice is increasingly occurring for high-severity inpatient hospital stays that account for the most expensive part of US healthcare.
“The [COVID-19] pandemic has placed unprecedented stress on the country’s healthcare system, making it more important than ever to ensure that Medicare dollars are spent appropriately,” the OIG report states.
The OIG website notes, “Medicare pays for many physician services using Evaluation and Management (commonly referred to as “E/M”) codes. New patient visits generally require more time than follow-up visits for established patients, and therefore E/M codes for new patients command higher reimbursement rates than E/M codes for established patients.”
The OIG describes one type of upcoding as “… an instance when [providers] provide a follow-up office visit or follow-up inpatient consultation, but bill using a higher-level E/M code as if [they] had provided a comprehensive new patient office visit or an initial inpatient consultation.
“Another example of upcoding related to E/M codes is misuse of Modifier 25,” the OIG continued. “Modifier 25 allows additional payment for a separate E/M service rendered on the same day as a procedure. Upcoding occurs if a provider uses Modifier 25 to claim payment for an E/M service when the patient care rendered was not significant, was not separately identifiable, and was not above and beyond the care usually associated with the procedure.”
How OIG Conducted the Study of Hospital Coding Practices
To perform its research, the OIG analyzed Medicare Part A claims for hospital stays for the six-year period from fiscal year (FY) 2014 through FY 2019. The OIG identified trends in billing and payments for inpatient hospital stays at the highest severity levels, as determined by the Medicare Severity Diagnosis Related Group (MS-DRG).
The OIG investigation revealed that the number of hospital stays billed at the highest severity level increased almost 20% between 2014 and 2019, while the number of stays billed at other severity levels decreased. These expenditures accounted for nearly half of all Medicare spending on inpatient hospital stays, the OIG reported.
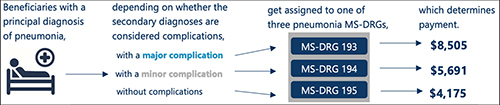
According to the OIG report, “Medicare pays hospitals more for beneficiaries in MS-DRGs with higher severity levels because they are typically more costly to treat.” The graphic above taken from the OIG report illustrates “how the presence of complications can affect Medicare payment for three beneficiaries with the same principal diagnosis.” (Graphic copyright: Federal Office of Inspector General Department of Health and Human Services.)
As Severity Levels Went Up, Inpatient Length of Stays Went Down
Interestingly, the average length of inpatient stays at the highest severity level decreased, and the average length of hospital stays overall remained largely the same, decreasing by just 0.1 days. In addition, the total number of inpatient hospital stays decreased by 5%.
The OIG report noted that “the increase in the number of stays billed at the highest severity level implies that beneficiaries were sicker overall. However, the decrease in the average length of stays at the highest severity level potentially undermines that idea because it is not consistent with sicker beneficiaries. Length of stay generally has a positive relationship to severity of stay; sicker beneficiaries stay in the hospital longer.”
The OIG confirmed that in FY 2019, Medicare spent $109.8 billion for 8.7 million hospital stays. Approximately 3.5 million (or 40%) of those stays were billed at the highest severity level, as determined by the MS-DRG. In addition, nearly half of the $109.8 billion spent, or $54.6 billion, was for stays billed at the highest severity level and Medicare paid an average of $15,500 per stay at that level.
The OIG report states that “stays at the highest severity level are vulnerable to inappropriate billing practices, such as upcoding—the practice of billing at a level that is higher than warranted. Specifically, nearly a third of these stays lasted a particularly short amount of time and over half of the stays billed at the highest severity level had only one diagnosis qualifying them for payment at that level. Further, hospitals varied significantly in their billing of these stays, with some billing much differently than most.”
The OIG study also found that over half of the inpatient stays billed at the highest severity level achieved that level due to only one diagnosis. According to the OIG, the severity of an inpatient stay depends on a patient’s secondary diagnosis and it only takes one secondary diagnosis to propel a patient into the highest severity level. The OIG determined that if the diagnosis was inaccurate or inappropriate, higher payments would not be warranted.
OIG Recommends CMS Conduct Targeted Reviews
The report found that the most frequently billed MS-DRG in FY 2019 was septicemia or severe sepsis and that hospitals billed for 581,000 of these stays, for which Medicare paid $7.4 billion. In addition, kidney and urinary tract infections, pneumonia, and renal failure were among the most common conditions to have a complication that led to a high severity classification.
In its report, the OIG recommended more oversight from CMS to ensure that Medicare dollars are spent appropriately. The OIG also suggests that CMS conduct targeted reviews of MS-DRGs and hospital stays that are vulnerable to upcoding, as well as the hospitals that frequently bill them.
Clinical Laboratories Are Forewarned
Medicare audits continue to be more detailed and rigorous and all healthcare providers—including clinical laboratories and anatomic pathology groups—should be prepared to present all necessary documentation to support claims if and when they are audited.
Improvements in software, machine learning, and artificial intelligence (AI) give Medicare officials and the OIG powerful tools to spot questionable provider billing. This includes medical laboratories whose billing patterns could arouse suspicions and trigger audits.
Upcoding is a long-standing problem for the Medicare program. What is changing is that federal officials now have better tools and resources to use in identifying patterns of upcoding that fall outside accepted parameters.