No explanation for the delay was provided by court after nine weeks of testimony in the prosecution of the former clinical laboratory executive
Former Theranos president/chief operating officer Ramesh “Sunny” Balwani’s often-delayed fraud trial was scheduled to resume on May 27 with a full day of defense witness testimony. It will now be delayed until June 7.
According to NBC Bay Area, a court assistant announced the delay but did not provide a reason for the postponement. A copy of the clerk’s notice posted on Twitter by Law360 also provided no further details. Pathologists and clinical laboratory managers must now wait several more months to learn what may be next revealed in testimony during this trial.
It is also yet one more delay in Balwani’s trial. His original trial date was January 2022 before being rescheduled for February. The needs for COVID-19 pandemic protocols further delayed the start multiple times until opening arguments began March 22 in a federal court room in San Jose, Calif.
One part of the trial has concluded. On May 20, the government rested its case against Balwani, who faces 12 counts of wire fraud and conspiracy to commit wire fraud while serving as second in command at Theranos, the now defunct Silicon Valley medical laboratory startup.
Former Theranos president and COO Ramesh “Sunny” Balwani (above) faces 12 charges of wire fraud and conspiracy to commit wire fraud while serving as chief operating officer of Theranos, the company that boldly declared it would disrupt the clinical laboratory testing industry. His trial, which began in March in US District Court in San Jose, Calif., is now delayed until June 7, when his defense attorneys will begin their first full day of witness testimony. (Photo copyright: Stephen Lam/Reuters/The New York Times.)
According to The Wall Street Journal (WSJ), nine weeks of testimony in US District Court in San Jose, Calif., included testimony from 24 witnesses. Prosecutors aimed to convince jurors Balwani controlled much of the day-to-day decision-making at Theranos and was a full participant in the fraud scheme.
NBC Bay Area stated prosecutors worked to link Balwani to two key decisions:
The rollout of the failed Edison blood testing device in Walgreens, and
The company’s improper use of the Pfizer logo on a report to Walgreens executives that appeared to validate Theranos’ technology.
Before this latest postponement, Balwani’s attorneys had begun their client’s defense by putting a naturopathic physician from Arizona on the stand. The witness testified to sending more than 150 patients to Theranos and to using the company’s blood tests for herself, the WSJ reported.
Bloomberg reported that prosecutors followed the previous outline used to gain the conviction of Elizabeth Holmes, founder and former CEO of Theranos, with many of the same witnesses from her trial reappearing on the stand to testify in the Balwani trial.
Prosecutors primarily focused their case on the injury to investors, which has angered some former Theranos customers.
“I feel like I belong to a group of people who were on the receiving end of a crime,” said Erin Tompkins—a Theranos customer who testified against both Holmes and Balwani—outside the courthouse shortly after finishing her testimony in the Balwani case, Bloomberg reported.
According to CNBC, Tompkins testified she was misdiagnosed as having HIV after having her blood drawn from a Theranos device at a Walgreens in Arizona.
“Despite the dedication and support of prosecutors, patient witnesses have been treated as peripheral” compared to the investors, Tompkins told Bloomberg. “We were defrauded because we trusted them with our blood and however many dollars for the test. But we weren’t robbed of millions of dollars.”
Susanna Stefanek, editorial manager at Apple Inc. who served on the Holmes jury, told Bloomberg, “[The prosecution] didn’t really prove that these patients were persuaded to get these blood tests by something she said or did, or even the advertising. The connection between Elizabeth Holmes and the patients was not that strong to us.”
Proving Patient Fraud
Michael Weinstein, JD, a former federal prosecutor turned Chair of White-Collar Litigation and Government at Cole Schotz in New Jersey, told Bloomberg that to convict Balwani of patient fraud, prosecutors must prove Balwani knew what was going on inside Theranos and that his misrepresentations caused patients to suffer.
“The government wants to show there was an inconsistency between what he was learning internally versus what he was saying externally,” Weinstein said.
With the Balwani trial likely to conclude this month, clinical laboratory directors and pathologists who have closely followed Theranos’ rise and fall should prepare for the final chapter in the saga.
With Millennials soon to make up the majority of the medical laboratory workforce, it’s only natural that digital networking is gaining momentum at events like the Executive War College
At any hour during the in-person event in New Orleans, attendees scheduled meetups, participants asked questions to conference organizers, and users discussed important clinical laboratory and anatomic pathology topics. All of those interactions occurred within the Whova meeting application, which served as the Executive War College’s virtual guide.
In many ways, widespread use of the meeting app reflects a younger crowd that lives life on mobile phones. It’s not all that different than the changing face of the clinical lab industry as laboratory veterans retire and new faces come in, said Robert Michel, Founder of the Executive War College (EWC) and Editor-in-Chief of Dark Daily’s sister publication The Dark Report.
“It’s clear from the soaring use of our conference’s meeting app at the Executive War College that a younger generation is changing how business is conducted during and after a lab industry conference,” he observed. “Generation X and Millennials are steadily influencing how people network at live events.”
“It is remarkable that, among the 900 attendees at this year’s event, there were more than 750,000 impressions involving the sponsors and companies supporting this year’s conference,” said Robert Michel (above), Editor-in-Chief of Dark Daily and Founder of the Executive War College. “It shows that these attendees are serious about identifying solutions and vendors who can help them solve the various pain points in their laboratories.” (Photo copyright: Dark Intelligence Group.)
88% of Attendees at Executive War College Used the Event App
Usage numbers aggregated during the EWC conference of people who downloaded and used the meeting app speak for themselves:
A large majority of attendees (88%) downloaded the app.
Users sent 11,398 messages in the app.
There were 136 community board discussions posted.
Users created 80 meetups, with 677 people attending those gatherings.
There were 764,745 sponsor impressions in the app (in other words, clicks on a sponsor link or attendees navigating to sponsor material).
What the numbers don’t convey is that the conference’s meeting app was also fun to use!
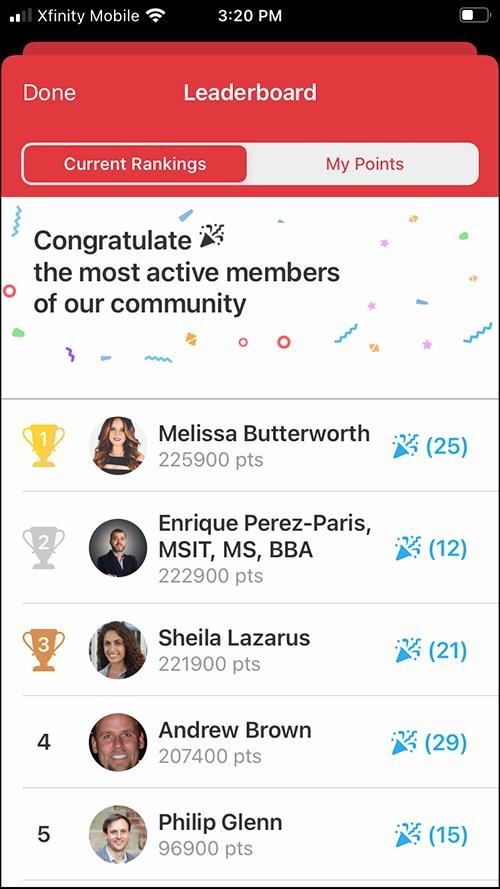
Butterworth spoke during a special session at the Executive War College. She also took the No. 1 spot on the meeting app’s leaderboard for the event, collecting an impressive 225,900 points. Users gained points for the leaderboard based on activities they completed in the app.
Spirited competition ensued among the leaderboard’s top users, who jockeyed for position as the conference progressed. Plenty of off-topic conversations took place in the app as well, as attendees helped each other navigate New Orleans with tips about restaurants, local cemetery tours, or where to work out.
The leaderboard on the Whova meeting application (above) at the conclusion of this year’s Executive War College on Laboratory and Pathology Management showed the top point gainers. (Photo copyright: Dark Intelligence Group.)
Clinical Laboratory Sponsors Reached Out to Attendees in New Ways
For sponsors and other vendors visiting the conference, the meeting app provided a different avenue to approach attendees beyond the typical networking that takes place during breaks, cocktail receptions, luncheons, and off-site parties.
For example, some sponsors shared white papers or YouTube videos via the app’s community boards or asked questions about topics of interest. Additionally, sponsors could respond directly to queries from attendees.
“At the Executive War College, there was clearly a sustained exchange between vendors looking to engage business development opportunities and participants who have pain points that need to be addressed and are looking for solutions,” Michel said.
The next Executive War College will return to New Orleans on April 25-26, 2023. Click on this link to access early registration discounts.
Potentially increasing the revenue write-off burden for clinical laboratories, HRSA changes, insurance contracting, policy and coverage questions for genetic and genomic testing, and patient relationship disconnects will expose cracks in lab test claim generation and billing processes
Last year it was estimated that collection agencies held $140 billion in unpaid medical bills, in addition to the amount of unpaid bills in pre-collection status, according to a New York Times report. More recently, the American Hospital Association showed that hospitals have provided upwards of $700 billion in uncompensated care since 2000, with over $40 billion in 2019 alone.
Because strategies to collect the unpaid can be complicated and time-consuming, many healthcare organizations, including clinical laboratories, choose to write off these uncollectible bills. Dark Daily and The Dark Report have covered clinical laboratory revenue challenges for many years. In considering the paths forward, software-as-a-service (SaaS) provider FrontRunner Healthcare (FrontRunnerHC) recently provided snapshots into the how and where of improved collections.
Fixing Data Issues that Lead to Forfeited Clinical Laboratory Revenue
The underpinnings of unpaid lab tests are many. In a recent interview with Dark Daily, FrontRunnerHC CEO and Founder John (JD) Donnelly estimated that about one-third of claims (prior to submission) include incorrect or missing patient information, such as insurance policy identification or demographics. These gaps undermine an organization’s ability to get paid. Donnelly estimates that bad-debt write-offs for commercial payer claims average over 15% of charges. To address these challenges, the company’s clean claims SaaS provides “instantaneous” patient insurance, demographic, and financial information.
Whether lower-dollar accessions such as routine testing, or the higher-dollar accessions of genetic tests, uncollected payments add up. Donnelly said that, in 2021, almost one-third of the company’s clients uncovered revenue ranging from $1 million to over $90 million using the software. Donnelly also estimated that the return for clients averages eight times the value of the investment in using the automated solution.
In one example, Sonora Quest, a joint venture between Banner Health and Quest Diagnostics, reported a 10-15% decline in write-offs due to aged claims, a savings of over $1million annually, as published in a case study. “As an aside, in a presentation at the Executive War College last November, they also attributed improvements in patient satisfaction measures to the software, including a 65% decrease in abandoned calls, 28% improvement in their call service factor, and 19% decrease in patient call volumes,” stated Donnelly.
Questions About Cost of Care Likely Cause Stress for Patients
As many know, nonpay issues are problematic not only for lab businesses and anatomic pathology practices but also for patients and their families who have little predictability with their cost of care in the midst of stressful health events. “From the time a patient is registered to the time the claim is paid, there are more challenges than people realize that jeopardize the patient’s experience as well as the provider’s ability to get reimbursed,” Donnelly explained. Medical laboratory administrators have struggled to respond, often by using traditional manual methods such as call centers, or more recently by considering the use of data automation tools.
From the patient payment perspective, Donnelly said, a good strategy is having the ability, on demand, to understand each patient’s specific financial situation and likelihood to pay. For example, using FrontRunnerHC’s software to gauge patients’ propensity to pay and determine financial disposition strategies, lab administrators may choose to offer payment plans or hardship discounts to those falling under the federal poverty level (FPL). Or they may choose to send a collection agency only the past-due accounts for patients who have a low likelihood to pay rather than sending them all past due accounts and focus in-house efforts on the others. One genetics lab client who recently started leveraging these software capabilities “is already seeing more than 5% in incremental net collections,” according to Donnelly.
Further, an estimated 2 million people switch insurance plans each month, reported Axios. “That velocity of change is tough for providers to manage, but it’s critical as insurance eligibility and registration issues are the number one reason for claims denials,” Donnelly said.
For a sense of the magnitude of the problem, “Between 25 and 33 cents of every dollar you spend on medical care pays for health care’s back office,” wrote Dana Miller Ervin in September 2021 for a series of investigations called “The Price We Pay,” published at WFAE 90.7 news in Charlotte, North Carolina. “Every medical provider and laboratory in the country has to negotiate with insurance companies. And since there are 900 health insurers, 6,000 hospitals and more than 100,000 physician practices—many of which are independent of larger systems—there are hundreds of thousands of negotiations.”
New Clinical Laboratory Business Challenges Making News Now
All these issues affecting revenue cycle management (RCM) for independent clinical laboratories, hospital and health system laboratories, and physician office laboratories could be compounded by three emerging issues.
Donnelly said that many lab clients have yet to be reimbursed for COVID tests they have performed, despite their HRSA-required due diligence prior to submitting the claims before the deadline. To avoid additional reimbursement risk, many labs have made the decision to stop testing the uninsured or charge them for it, ABC News reported in late March. As of early April, however, Congress was in discussions to re-fund at least some of the Uninsured Program, reported Politico.
Secondly, and also daunting, are the questions surrounding payer coverage and reimbursement for genetic tests and genomic testing. Thanks to high-deductible health plans (HDHPs), clinical laboratories and anatomic pathology groups increasingly must collect deductibles that may be the full amount of the test – and directly from patients rather than from insurance companies. Therefore, there is more demand from patients to understand their expected cost before the test, Donnelly added.
Problems can arise, for both labs and patients, if they don’t know whether a test has been preauthorized for medical necessity or if they lack accurate insurance information such as in-network or out-of-network. “Getting all the needed and accurate info upfront prior to it going into the LIS [Laboratory Information System] can be a reimbursement game changer,” stated Donnelly.
“For a high complexity, high-throughput diagnostic lab, an efficient workflow is critical,” stated Kyle Koeppler, President of nuCARE Medical Solutions Inc., a FrontRunnerHC client. “Capturing the correct patient demographics and insurance information at patient intake increases the accuracy of every order and makes every process involving patient information much more efficient,” Koeppler shared. “It’s simply too costly to risk having inaccurate information at intake.”
And lest we forget, the Protecting Access to Medicare Act (PAMA) is looming with its reimbursement cuts planned through 2026, and requirements of many labs to report private payer rates on a test-by-test basis. While delayed again, the 2023 PAMA reporting requirements and payment cuts must not be ignored, and planning is needed in order to ensure appropriate reimbursement, Donnelly added.
Addressing Long Payment Cycles for Claims, Dead Ends, and Decreased Collection Rates
The CAQH report cites that data automation resulted in efficiency savings of $122 billion annually for the US healthcare system in 2020 yet “meaningful opportunities for additional savings remain.”
Data automation can reduce the burden of labor-intensive functions in coding, billing, filing appeals, and collecting from payers and patients and, therefore, reduce overall RCM costs. The Council for Affordable Quality Healthcare’s (CAQH) 2020 Index reported, “Considering the millions of times these transactions occur every day, the savings potential across the healthcare economy [from streamlining administrative processes] is significant.”
“One way to avoid potential write-offs is by reworking a claim, but the rework is often left undone,” stated John (JD) Donnelly (above), CEO and Founder of FrontRunnerHC. “The better way to avoid a potential write-off is to ensure you’ve got a clean claim in the first place.” (Photo copyright: FrontRunnerHC.)
The intended outcome is an increase in the total amount of revenue collected from the same number of claims.
To that end, FrontRunnerHC’s software links critical data within its partner ecosystem. This ecosystem includes the well-established credit reporting agencies as well as data available through connected healthcare payers and providers equipped with electronic data interchange (EDI) capabilities. “While an employee may be able to manually work about six accessions in an hour, clients can process approximately 40,000 patients in an hour through software automation, leaving staff to work on more value-added initiatives,” stated Donnelly.
Ideally, missing and inaccurate patient information or insurance verification, which are crucial for producing prompt payments and clean claims, should be corrected before a specimen is collected, Donnelly said. However, if the laboratory is nursing aging accounts receivable (AR), Donnelly advises an audit and cleanup of the AR backlog as a first step to quickly fix information errors and reduce write-offs. “In your AR bucket of $10 million, you may have $3 million that’s collectible or $9.8 million that’s collectible. By leveraging software to clean up what can be collected, clients can go after the money they deserve.”
Improve Collections Through Data Automation While Assisting in the Patient Financial Journey
With the rise of telehealth/telemedicine, healthcare consumerism, and care delivered to nontraditional sites, it makes sense that the idea of the clinical laboratory as a silent partner in healthcare could be changing.
“Could we one day see patients asked for not only their preferred pharmacy but their preferred clinical laboratory as well?” Donnelly pondered and added, “I think the answer is yes, and it’s sooner than many think.”
Understanding the patient’s experience is a key step in providing patient-centered care. Therefore, patient experience programs that originate at clinical laboratories where specimens are processed, but before specimens have been collected, could make these labs more visible in their markets and enable them to capitalize on the advantages of data automation to sustainably improve revenue cycle management.
“The patient’s financial journey which runs in parallel to their clinical journey can get pretty bumpy, and those bumps impact their overall experience as well as the provider’s bottom line,” added Donnelly. “Getting accurate patient information upfront and catching any changes to the information as needed throughout the process helps clients create a smoother patient journey by enabling them to quickly manage through the bumps or eliminate them altogether.”
—Liz Carey
This article was produced in collaboration with FrontRunnerHC.
Gottlieb will speak about the state of AI in healthcare at the event May 11-12
Medical technicians in clinical laboratories and pathology groups may worry that artificial intelligence (AI) will eventually put them out of their jobs.
However, that’s not likely to be the case, according to former Food and Drug Administration (FDA) Commissioner Scott Gottlieb. He was just announced as a top speaker at the Artificial Intelligence in Healthcare and Diagnostics (AIHD) Conference, which takes place May 10-11 in San Jose, Calif.
Instead, expect AI in healthcare to help labs better aggregate and analyze an ever-growing repository of clinical data.
“As we start to digitize more of this information, build out bigger repositories, and correlate more of this information with experimental evidence that’s also captured digitally, it’s going to become an immensely powerful tool,” Gottlieb said during a 2021 webinar hosted by Proscia, which develops pathology software embedded with AI.
Former FDA Commissioner Scott Gottlieb said AI in healthcare will “become an immensely powerful tool.” (Photo courtesy of: Worldwide Speakers Group)
“[AI is] going to be a predictive tool,” he continued. “So, now you start to think about digital data from traditional pathology, digital data from characterizing tumors to sequencing, alongside digital data capture through electronic health records. And you start to have a really powerful, robust set of information.”
Writing for MobiHealthNews last year, Liz Kwo, MD, also noted the potential of AI to deal with unstructured data—in other words, information that is not in a pre-set data model and thus difficult to analyze.
“In many cases, health data and medical records of patients are stored as complicated unstructured data, which makes it difficult to interpret and access,” wrote Kwo, who is Deputy Chief Clinical Officer at insurer Anthem and Faculty Lecturer at Harvard Medical School.
“AI can seek, collect, store, and standardize medical data regardless of the format, assisting repetitive tasks and supporting clinicians with fast, accurate, tailored treatment plans and medicine for their patients instead of being buried under the weight of searching, identifying, collecting and transcribing the solutions they need from piles of paper formatted EHRs,” she added.
AIHD conference to explore the state of artificial intelligence in healthcare
At AIHD, Gottlieb will take part in a fireside chat and also contribute to a panel discussion with other keynote speakers.
“There’s no better individual than Dr. Gottlieb to address AIHD participants about the state of artificial intelligence, where it’s going, how it’s regulatory oversight will unfold, and what’s likely to be the most surprising contribution of AI in patient care,” said Robert Michel, founder of AIHD, Executive Director of the Precision Medicine Institute, and Editor-in-Chief of clinical lab intelligence publication The Dark Report.
The event will bring together senior-level representatives from AI companies, hospitals, physician offices, and diagnostic providers.
Gottlieb promoted greater use of digital tools for clinicians
“I can envision a world where, one day, artificial intelligence can help detect and treat challenging health problems, for example by recognizing the signs of disease well in advance of what we can do today,” Gottlieb stated at the time. “These tools can provide more time for intervention, identifying effective therapies and ultimately saving lives.”
During and after his tenure at the FDA, he has been a prolific commentator about the SARS-CoV-2 pandemic and steps public health agencies have taken to curb COVID-19.
Gottlieb is currently a Senior Fellow at the American Enterprise Institute, a public policy think tank. He is also partner at venture capital firm New Enterprise Associates and serves on the boards of Pfizer and Illumina.
The Department of Justice steps beyond the law’s original focus on opioid-related lab testing fraud
An interesting aspect with enforcement of the Eliminating Kickbacks in Recovery Act of 2018 (EKRA) is the government’s willingness to go after charges tied to fraudulent COVID-19 testing.
The case U.S. vs. Malena Badon Lepetich provides a good example of this approach. A grand jury indicted Lepetich on various healthcare fraud charges last year, including that she allegedly offered to pay kickbacks for referrals of specimens for COVID-19 testing.
“The government had really only used EKRA in the context of addiction treatment space,” attorney Alexander Porter, a Partner at law firm Davis Wright Tremaine in Los Angeles, said in the latest issue of The Dark Report. “The Lepetich case shows that the government’s going to use EKRA beyond that context and go into other areas where they think that it can be useful—in particular, in the area of COVID-19 testing.”
Clinical laboratories and pathology groups should take note of this development.
Attorney Alexander Porter said EKRA enforcement now goes after fraudulent COVID-19 testing. (Photo: Davis Wright Tremaine)
Defendant Allegedly Filed $10 Million in Fraudulent Lab Claims
Lepetich was the owner of MedLogic, a clinical laboratory in Baton Rouge, La.
In addition to the fraudulent COVID-19 testing charges, she allegedly solicited and received kickbacks in exchange for referrals of urine specimens for medically unnecessary tests, according to the U.S. Department of Justice (DOJ).
EKRA Provisions Rose from the Opioid Crisis in the U.S.
EKRA is a criminal law that falls under the Communities and Patients Act, which lifted restrictions on medications for opioid treatment and sought to limit overprescribing of opioid painkillers. Originally, EKRA targeted fraudulent practices at sober homes and substance abuse treatment centers. However, the final draft of the bill added clinical laboratories to the list of providers under potential scrutiny.
At the time Congress passed EKRA, the law was primarily aimed at fraudulent activity in opioid treatment centers, including related lab testing.
Thus, the government’s use of EKRA in the COVID-19 charges against Lepetich case is newsworthy and establishes a precedent, noted Porter. He’ll speak about EKRA at the 2022 Executive War College on Laboratory and Pathology Management. The event takes place April 27-28 in New Orleans.
A contentious part of EKRA for clinical laboratories and pathology groups is that certain conduct protected under the federal Anti-Kickback Statute is treated as a criminal offense under EKRA. Some common lab practices come under that confusing designation, such as paying lab sales reps on a commission-based formula based on testing volumes they generate.
Proof of vaccination, masking, and availability of on-site testing will continue to be measures taken at in-person events for pathologists and medical laboratory professionals
Organizers of in-person clinical laboratory conferences face an interesting dilemma as they plan events in 2022: Where do they draw the line with COVID-19 safety protocols?
On one hand, the surge of cases caused by the SARS-CoV-2 Omicron variant seems to be in its waning stages and large swaths of the population are vaccinated. On the other hand, clinical laboratory and anatomic pathology events want potential registrants to have confidence that it is safe to travel and attend the gatherings.
One lab industry conference producer who happens to be knee-deep in preparing for an in-person meeting this spring is Robert Michel, Editor-in-Chief of The Dark Report and Founder of the 27th Annual Executive War College on Laboratory and Pathology Management. This informative event takes place on April 27-28 in New Orleans and includes COVID-19 protocols to protect attendees.
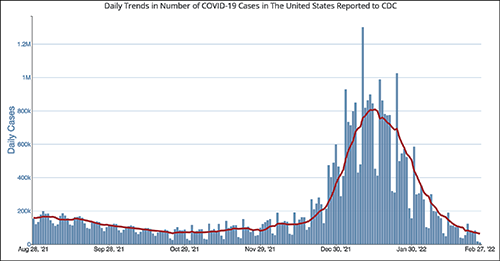
The CDC chart above shows the daily number of new COVID-19 cases in the US for the six-month period ending Feb. 28, 2022. Clinical laboratory managers should note that the number of new cases is at its lowest level since the Omicron variant showed up early this year.
“It’s important for all those planning to attend this year’s Executive War College to know that screening COVID-19 protocols will be in place to ensure the health and safety of all participants,” Michel noted. “We did a large lab conference in the fall of 2021 that included protocols for COVID-19 and the attendees told us they appreciated the protection provided by those protocols.”
After a significant rise in COVID-19 cases in January 2022 due to the Omicron variant, current daily case levels now are lower than they were six months ago before the new variant hit, according to numbers from the federal Centers for Disease Control and Prevention (CDC).
The in-person 2021 Executive War College, which took place in San Antonio on Nov. 2-3, 2021, followed the CDC’s recommendations:
COVID-19 protocols included a daily set of questions and a temperature check for all speakers and attendees before they were allowed to enter the conference area.
CLIA-complex rapid PCR COVID-19 tests were available for individuals whose temperature and answers to the screening questions indicated the need for such testing.
Attendees used an app to answer the daily screening questions and upload proof of vaccination.
“At last fall’s Executive War College, approximately 400 attendees were screened on each of the three days before entering the conference area and not one rapid COVID-19 test was needed,” Michel said. “Not only is that an outstanding outcome, but a number of attendees also told us they appreciated our efforts to keep them safe and protect their health.”
The 2022 Executive War College will follow the CDC’s updated COVID-19 guidelines, along with any state and local directives in effect as of April 27.
Although 300 attendees were expected at the 2021 Executive War College, 400 registered and participated.
Proof of Vaccination Has Been Required at Other Clinical Lab Industry Events
Organizers of other clinical lab conferences also have dealt with COVID-19 safety protocols. For example, the American Clinical Laboratory Association (ACLA) will hold its annual meeting in Washington, D.C., on March 9. COVID-19-related requirements for attendees will include proof of vaccination uploaded to a vaccine verification vendor and proof of a negative PCR test taken within 72 hours prior to the event.
The annual meeting of the American Society of Clinical Pathology (ASCP) occurs later this year in September in Chicago—too early yet to publish protocols. Last year’s ASCP conference in Boston was a hybrid event, offering both in-person and virtual options. Those who attended in person needed to upload proof of vaccination to a third-party vendor and were required to wear masks. On-site COVID-19 testing was available.
Revived Corporate Travel Could Boost Clinical Laboratory Conferences
The path back to live events across all industries has not been easy given various COVID-19 surges, political divisiveness over masking, frozen corporate travel budgets, and corporate policies banning or limiting employee travel.
Conference organizers throughout the United States universally hope those barriers will lower as 2022 progresses.
“With the fast-spreading Omicron triggering another round of setbacks to start 2022, event planners now are betting on spring to finally mark a turning point for the hard-hit industry,” MarketWatch reported on Feb. 4. “Their hopes hinge on American corporations taking a note from the recovery already under way for domestic air travel for leisure purposes, with the linchpin being a robust revival of trade show attendance and other in-person business gatherings.”
For Michel, offering actionable advice through well-thought-out sessions has been a cornerstone of the content offered each year at the Executive War College. He believes that approach will continue to be the strongest drawing point for clinical laboratory and pathology executives now considering attending the event.
“Our reading of the tea leaves is that across the profession of laboratory medicine, a great many managers, administrators, executives, and pathologists want to return to in-person conferences,” Michel noted. “Registrations for our April event are running ahead of 2019, and people tell us that they recognize the changes in healthcare and the lab marketplace because of the pandemic. They want to understand what’s driving current trends, like greater consumer involvement in lab testing and how to get private payers to reimburse claims for COVID-19 and genetic tests, as well as how a growing number of clinical laboratories are incorporating artificial intelligence solutions in both clinical care settings and lab operations.”