Goal is to demonstrate how whole human genome sequencing of newborns can deliver important diagnostic findings associated with 250 genetic conditions
Clinical laboratory testing and genetics are moving closer to the delivery room than ever before. In the largest study of its kind in North America, genomic scientists plan to supplement traditional screening for inherited diseases—traditionally performed on a blood sample taken shortly after birth—with whole genome sequencing (WGS) on 100,000 newborns in New York City during their first five years of life, LifeSciencesIntelligence reported.
Conducted by genetic scientists at NewYork-Presbyterian (NYP) and Columbia University, in collaboration with genetic company GeneDx, a wholly-owned subsidiary of health intelligence company Sema4 (NASDAQ:SMFR), the genetic research study, called GUARDIAN (Genomic Uniform-screening Against Rare Diseases In All Newborns), will screen newborn babies for 250 rare diseases that are generally not tested for.
The GUARDIAN program will “drive earlier diagnosis and treatment to improve the health of the babies who participate, generate evidence to support the expansion of newborn screening through genomic sequencing, and characterize the prevalence and natural history of rare genetic conditions,” according to a Sema4 news release.
“The appetite for this is growing. The awareness of this is growing. We all see it as inevitable,” medical geneticist Robert Green, MD, at Brigham and Women’s Hospital and Harvard Medical School told USA Today. “We are grossly underutilizing the life-saving benefits of genetics and we have to get past that.” Clinical laboratory leaders understand the value of early detection of disease and subsequent early treatment. (Photo copyright: Harvard Medical School.)
Improving Health of Babies Through Early Detection of Disease
GUARDIAN aims to use WGS to identify conditions at birth that can affect long-term health and subsequently enhance treatment options and possibly prevent disability or death.
The 250 different diseases GUARDIAN will be screening for typically strike young children. They are mostly rare conditions that:
have an onset before five years of age,
have a greater than 90% probability of the condition developing based on the genetic result,
have effective approaches and treatments that are already available, and/or
have a well-established natural history of the condition.
“We’re entering the therapeutic era and leaving the diagnostic era,” Paul Kruszka, MD, Chief Medical Officer at GeneDx told USA Today. “This potentially has the opportunity to change the way we practice medicine, especially in rare disease.”
Some Parents Reluctant to Agree to Genetic Testing
Green and his research team first began analyzing the genetic sequences of newborns back in 2013. They believe the costs of performing infant WGS is worthwhile because it can improve lives. However, Green also recognizes that some parents are reluctant to agree to this type of genetic testing due to concerns regarding privacy and the fear of discovering their baby may have an illness.
“You’ve gone through all this pregnancy and you’re sitting there with a healthy baby (and I’m) offering you the opportunity to find out something that’s devastating and terrifying,” he told USA Today. “How fun is that?”
Green continued. “We can respect people who don’t want to know, but also respect people who do want to know. Some families will say ‘I treasure the precious ignorance.’ Others will say ‘If I could have known, I would have poured my heart and soul into clinical trials or spent more time with the child when she was healthy.’”
WGS Screening Identifies Undiagnosed Illnesses in Newborn’s Family
The scientists also found that performing WGS in newborns can detect diseases in the infants as well as unknown illnesses in the families of those babies. According to Kruszka, many parents often seek a diagnosis for a rare disease present in their children for several years. Since many common diseases develop as a result of certain combinations of genes, if illnesses are diagnosed at birth, it could extradite the treatment process, prevent complications, and provide better health outcomes for patients.
“We are relentlessly focused on accelerating the adoption and use of genomic information to impact the lives of as many people as possible, particularly newborns and children,” said Katherine Stueland, President and CEO, Sema4, in the Sema4 news release. “As the first commercial laboratory to launch a rapid whole genome sequencing offering, to address broad unmet needs for early diagnosis, participation in this study is an important step forward for healthcare and in delivering on our goal to sequence once, analyze forever.”
The study is open to all babies in New York City who are born in a health system that participates in the GUARDIAN program, regardless of their race, income, or health insurance coverage.
“The results from this study will help us understand the true impact sequencing at birth can have on newborns and their families in comparison to the current standard of care, particularly as we’ll evaluate clinical outcomes in addition to the psychosocial effect on families,” said Kruszka in the Sema4 news release.
Anything that improves the health of newborn babies is a good thing. Regardless of the cost, if DNA analysis can give newborns and their families a better chance at detecting inherited diseases early while clinical laboratory treatment could make a difference, it is worth pursuing.
There was cautious optimism about the ability of Canada’s medical laboratories to innovate in ways that advance patient care, while recognizing the ongoing challenge of adequate lab staffing and budget constraints
TORONTO, ONTARIO, CANADA—This week, more than 150 leaders representing clinical laboratories, anatomic pathology labs, in vitro diagnostics (IVD) companies, and provincial health officials gathered for the first “Canadian Diagnostic Executive Forum” (CDEF) since 2019. It would be apt to say that the speakers objectively addressed all the good, the bad, and the ugly of Canada’s healthcare system and its utilization of medical laboratory testing services.
Over the two days of the conference, speakers and attendees alike concurred that the two biggest issues confronting clinical laboratories in Canada were inadequate staffing and an unpredictable supply chain. There also was agreement that the steady increase in prices, fueled by inflation, is exacerbating continuing cost increases in both lab salaries and lab supplies.
Canada’s Health System Has Several Unique Attributes
Canada’s healthcare system has two unique attributes that differentiate it from those of other nations. First, healthcare is mandated by a federal law, but generally each of Canada’s 13 provinces and territories operates its own health plan. Thus, the health system in each province and territory may cover a different mix of clinical services, therapeutic drugs, and medical procedures. The federal government typically pays 40% of a province’s health costs and the province funds the balance.
Second, it is a fact that 90% of the Canadian population lives within 150 miles of the United States border. Yet there are provinces with large populations that have geography that ranges from the US border to north of the Arctic Circle. These provinces have a major challenge to ensure equal access to healthcare regardless of where their citizens live.
During day one of the conference, several presentations addressed innovations that supported those labs’ efforts to deliver value and timely insights during the COVID-19 pandemic. For example, a lab team in Alberta launched a research study involving SARS-CoV-2 virus surveillance from the earliest days of the outbreak. This study was presented by Mathew Diggle, PhD, FRCPath, Associate Professor and Program Lead for the Public Health Laboratory (ProvLab) Medical-Scientific Staff at Alberta Precision Laboratories in Edmonton, Alberta.
Study Designed to Identify Coinfections with COVID-19
While performing tens of thousands of COVID-19 tests from the onset of the pandemic, and identifying the emergence of variants, the ProvLab team also tracked co-infection involving other respiratory viruses.
“This is one of the largest eCoV [endemic coronavirus] studies performed during the COVID-19 pandemic,” Diggle said. “This broad testing approach helped to address a pivotal diagnostic gap amidst the emergence of a novel pathogen: cross-reactivity with other human coronaviruses that can cause similar clinical presentations. This broad surveillance enabled an investigation of cross-reactivity of a novel pathogen with other respiratory pathogens that can cause similar clinical presentations.
“Fewer than 0.01% of specimens tested positive for both SARS-CoV-2 and an eCoV,” he explained. “This suggested no significant cross-reactivity between SARS-CoV-2 and eCoVs on either test and provided a SARS-CoV-2 negative predictive value over 99% from an eCoV-positive specimen … The data we collected was highly compelling and the conclusion was that there was no coinfection.”
Chairing the two days of presentations at this weeks’ Canadian Diagnostic Executive Forum was Kevin D. Orr (above), Senior Director of Hospital Business at In-Common Laboratories. He also served on the program for this national conference serving clinical laboratories, anatomic pathology labs, and in vitro diagnostics (IVD) companies throughout Canada. This was the first gathering of this conference since 2019. Attendees were enthusiastic about the future of medical laboratory services in Canada, despite lab staffing shortages and rising costs due to inflation. (Photo copyright The Dark Report.)
Clinical Laboratory Regionalization in Quebec
One of Canada’s largest projects to regionalize and harmonize clinical laboratory services is proceeding in Quebec. Leading this effort is Ralph Dadoun, PhD, Project Director for OPTILAB Montreal, which is part of the Ministry of Health and Social Services in Quebec. The ambitious goal for this project is to move the 123 clinical laboratories within the province into 12 clusters. Initial planning was begun in 2013, so this project is in its ninth year of implementation.
During his presentation, Dadoun explained that the work underway in the 12 clusters involves creating common factors in these categories:
Implementation consistent with and respecting ISO-15189 criteria.
Another notable achievement in Quebec is the progress made to implement a common laboratory information system (LIS) within all 12 clusters. The first three laboratory clusters are undergoing their LIS conversions to the same platform during the next 180 days. The expectation is that use of a common LIS across all clinical laboratory sites in Quebec will unlock benefits in a wide spectrum of lab activities and work processes.
The 2022 CDEF featured speakers from most of the provinces. The common themes in these presentations were the shortage of lab personnel across all technical positions, disruptions in lab supplies, and the need to support the usual spectrum of lab testing services even as lab budgets are getting squeezed.
At the same time, there was plenty of optimism. Presentations involving adoption of digital pathology, advances in early disease detection made possible by new diagnostic technologies, and the expansion of precision medicine showed that clinical laboratories in Canada are gaining tools that will allow them to contribute to better patient care while helping reduce the downstream costs of care.
The Canadian Diagnostics Executive Forum is organized by a team from In-Common Laboratories in North York, Toronto, Ontario. Founded in 1967, it is a private, not-for-profit company that works with public hospitals and laboratory medicine providers. Information about CDEF can be found at its website, where several of this year’s presentations will be available for viewing.
Proof-of-concept study ‘highlights that using AI to integrate different types of clinically informed data to predict disease outcomes is feasible’ researchers say
Artificial intelligence (AI) and machine learning are—in stepwise fashion—making progress in demonstrating value in the world of pathology diagnostics. But human anatomic pathologists are generally required for a prognosis. Now, in a proof-of-concept study, researchers at Brigham and Women’s Hospital in Boston have developed a method that uses AI models to integrate multiple types of data from disparate sources to accurately predict patient outcomes for 14 different types of cancer.
The process also uncovered “the predictive bases of features used to predict patient risk—a property that could be used to uncover new biomarkers,” according to Genetic Engineering and Biotechnology News (GEN).
Should these research findings become clinically viable, anatomic pathologists may gain powerful new AI tools specifically designed to help them predict what type of outcome a cancer patient can expect.
“Experts analyze many pieces of evidence to predict how well a patient may do. These early examinations become the basis of making decisions about enrolling in a clinical trial or specific treatment regimens,” said Faisal Mahmood, PhD (above) in a Brigham press release. “But that means that this multimodal prediction happens at the level of the expert. We’re trying to address the problem computationally,” he added. Should they be proven clinically-viable through additional studies, these findings could lead to useful tools that help anatomic pathologists and clinical laboratory scientists more accurately predict what type of outcomes cancer patient may experience. (Photo copyright: Harvard.)
AI-based Prognostics in Pathology and Clinical Laboratory Medicine
The team at Brigham constructed their AI model using The Cancer Genome Atlas (TCGA), a publicly available resource which contains data on many types of cancer. They then created a deep learning-based algorithm that examines information from different data sources.
Pathologists traditionally depend on several distinct sources of data, such as pathology images, genomic sequencing, and patient history to diagnose various cancers and help develop prognoses.
For their research, Mahmood and his colleagues trained and validated their AI algorithm on 6,592 H/E (hematoxylin and eosin) whole slide images (WSIs) from 5,720 cancer patients. Molecular profile features, which included mutation status, copy-number variation, and RNA sequencing expression, were also inputted into the model to measure and explain relative risk of cancer death.
The scientists “evaluated the model’s efficacy by feeding it data sets from 14 cancer types as well as patient histology and genomic data. Results demonstrated that the models yielded more accurate patient outcome predictions than those incorporating only single sources of information,” states a Brigham press release.
“This work sets the stage for larger healthcare AI studies that combine data from multiple sources,” said Faisal Mahmood, PhD, Associate Professor, Division of Computational Pathology, Brigham and Women’s Hospital; and Associate Member, Cancer Program, Broad Institute of MIT and Harvard, in the press release. “In a broader sense, our findings emphasize a need for building computational pathology prognostic models with much larger datasets and downstream clinical trials to establish utility.”
Future Prognostics Based on Multiple Data Sources
The Brigham researchers also generated a research tool they dubbed the Pathology-omics Research Platform for Integrative Survival Estimation (PORPOISE). This tool serves as an interactive platform that can yield prognostic markers detected by the algorithm for thousands of patients across various cancer types.
The researchers believe their algorithm reveals another role for AI technology in medical care, but that more research is needed before their model can be implemented clinically. Larger data sets will have to be examined and the researchers plan to use more types of patient information, such as radiology scans, family histories, and electronic medical records in future tests of their AI technology.
“Future work will focus on developing more focused prognostic models by curating larger multimodal datasets for individual disease models, adapting models to large independent multimodal test cohorts, and using multimodal deep learning for predicting response and resistance to treatment,” the Cancer Cell paper states.
“As research advances in sequencing technologies, such as single-cell RNA-seq, mass cytometry, and spatial transcriptomics, these technologies continue to mature and gain clinical penetrance, in combination with whole-slide imaging, and our approach to understanding molecular biology will become increasingly spatially resolved and multimodal,” the researchers concluded.
Anatomic pathologists may find the Brigham and Women’s Hospital research team’s findings intriguing. An AI tool that integrates data from disparate sources, analyzes that information, and provides useful insights, could one day help them provide more accurate cancer prognoses and improve the care of their patients.
Study also may have found relationship between atherosclerosis and cholesterol
Chinese scientists have developed a cutting-edge method for non-invasively monitoring blood cholesterol levels in humans. The innovative technology utilizes images of skin on hands and may eliminate the need for both invasive venipunctures and fasting for testing cholesterol. Given the large volumes of blood cholesterol tests currently performed by clinical laboratories, this new technology could have significant impact on cholesterol testing if further studies confirm its capabilities.
Notably, the Chinese researchers have apparently already developed a lab analyzer to perform the procedure and it is being used in clinical care. However, in the United States and other countries, this technology will require additional clinical studies and regulatory review before clinical laboratories would be able to use it in daily patient care.
The cholesterol sensing system consists of a detection reagent associated with a fluorescent group that binds to skin cholesterol, and a detection device. Cholesterol levels are easily obtained from the skin, according to the researchers, by analyzing the manner in which the skin absorbs and scatters light via a scanner.
Should this technology be validated for clinical care, it could replace other invasive clinical laboratory tests for cholesterol measurement.
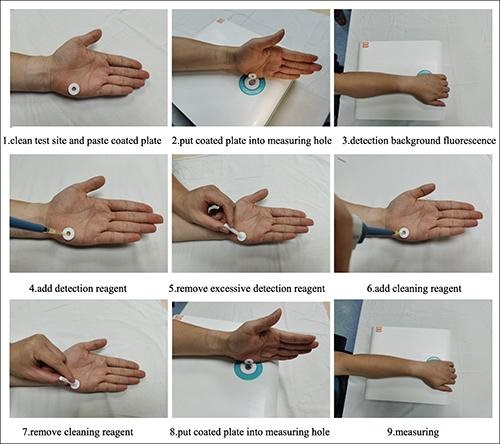
The series of images above, taken from the researchers’ Lipids in Health and Disease published study, demonstrates how their non-invasive clinical laboratory test for total blood cholesterol is performed. Non-invasive clinical laboratory tests for monitoring biomarkers in the blood are always preferred by patients over veinous punctures and fasting. (Photo copyright: Hefei Institutes of Physical Science, Chinese Academy of Sciences.)
First Evidence of Relationship between Cholesterol and Atherosclerosis
“Just put your hands on, and the system will tell you the cholesterol data,” Yikun Wang, PhD, Professor, Department of Physical Sciences, Hefei Institutes of Physical Science, Chinese Academy of Sciences, and leader of the research team, told Diagnostics World. “Cholesterol is one of several types of fats (lipids) that play an important role in human body, we can track your fats in this simple way.”
To perform the testing, clinicians first clean the test site located on the fleshy edge of the palm of the hand with an alcohol swab. A patient’s non-dominant hand is used for the test as the skin on that hand is typically less abrasive and contains fewer melanocytes, which allows for more stable results. A plastic-coated annulus is then applied to the test site and the examined portion is positioned on the measuring hole of the detection system to measure the background light spectrum of the skin.
Once the background signal is ascertained, the detection reagent is added to the annulus until it is full. After 60 seconds, any excess detection reagent is removed from the annulus. A cleaning reagent is then added to the annulus for 30 seconds and removed with a sterile cotton swab. The treated portion of the skin is then placed over the measuring hole of the detection system and two spectrums of light are compared to measure the skin cholesterol, which accurately correlates to the cholesterol in the bloodstream.
“Compared to in-situ detection used in the previous clinical research, our device may offer more accurate results for we can avoid the influence of pressure and skin background differences [person to person],” Wang said. “Study results offer the first evidence of a relationship between skin cholesterol and atherosclerotic disease in a Chinese population, which may be of great significance to researchers around the world.”
Initially, 154 patients diagnosed with acute coronary syndrome (ACS) between January 2020 and April 2021 were involved in the study. However, only 121 of those patients were included in the final study with the remaining being excluded due to at least one of the following criteria:
Severe hepatic (liver) or renal (kidney) insufficiency, and
Obesity.
Clinician Use Can Affect Accuracy of Test
Developed by researchers from the Hefei Institutes of Physical Science Chinese Academy of Sciences, and the University of Science and Technology of China, the researchers noted that how clinicians operate the device can have an impact on the accuracy of the test results.
“A critical step in the [testing] process that is subject to operator variability is blotting, which requires the operator to remove an unbound detector from the palm before adding the indicator,” Wang told Diagnostics World. “Excess residual indicator solution can result in falsely increased skin cholesterol levels. Considering this, we are planning to develop a simplified and standardized blotting procedure.”
Millions of people in the US live with illness that requires regular monitoring of blood cholesterol. Normal total cholesterol should be less than 200 milligrams per deciliter (mg/dL). According to the federal Centers for Disease Control and Prevention (CDC), nearly 94 million US adults over the age of 20 have total cholesterol levels higher than 200 mg/dL and 28 million adults have total cholesterol levels higher than 240 mg/dL. In addition, 7% of children and adolescents between the ages of six and 19 have high cholesterol. For these reasons, cholesterol testing represents a substantial portion of the clinical laboratory tests performed daily in this country.
This new non-invasive technology for monitoring total blood cholesterol in humans could greatly benefit patients, especially if it eliminates the need for venipunctures and fasting prior to testing. Clinical laboratory managers and pathologists may want to follow the progress of this new cholesterol testing technology as it demonstrates its value in China and is submitted for regulatory review in this country.
Officials also worry about diminishing smallpox vaccinations, which offered people protection against the infectious disease
Monkeypox challenges from the current outbreak have dogged public health agencies even though the disease was first identified more than 50 years ago. That is because the virus has found new avenues of infection. These developments will be relevant for the nation’s clinical laboratories, which are often the first healthcare providers to confirm a suspected case is positive for monkeypox and notify a public health laboratory about the positive test result.
The latest monkeypox numbers from the federal Centers for Disease Control and Prevention (CDC) indicate that, as of September 6, the US has identified 19,962 cases in the 2022 outbreak, while worldwide the case number is 52,037.
In “When It Comes to Monkeypox Testing, Clinical Laboratories Should Be Aware of Five Significant Developments,” Dark Daily wrote about steps being taken to identify and control infections in America as well as trends in medical laboratory testing for monkeypox. This included reports of phlebotomists refusing to draw monkeypox blood samples and how social stigma surrounding the disease can affect who gets a medical laboratory test.
Workers at clinical laboratories and anatomic pathology groups will gain from understanding why monkeypox has spread beyond its traditional geography.
“Monkeypox symptoms include swollen lymph nodes, fever, and body aches that result in red bumps on hands, feet, mouth, and genitals,” Bodhraj Acharya, PhD (above), of the Laboratory Alliance of Central New York, told Dark Daily. “It spreads by close contact, respiratory droplets, lesions, and bodily fluids.” Clinical laboratories engaged in testing for monkeypox will want to stay alert to patients presenting with such symptoms. (Photo copyright: Laboratory Alliance of Central New York.)
African Public Health Officials Saw New Monkeypox Challenges Coming
Researchers and public health experts have been perplexed about how and why the latest monkeypox outbreak has occurred so aggressively beyond its origin in rural Central Africa.
“Monkeypox is caused by the pox virus, with a close resemblance to smallpox,” said Bodhraj Acharya, PhD, Manager of Chemistry and Referral Testing at the Laboratory Alliance of Central New York, in a conversation with Dark Daily. “Unlike COVID-19, this is an old enemy which has roots in the 1970s from Congo, when the disease was erratically endemic in Africa.”
According to the World Health Organization (WHO), most monkeypox cases since 1970 have been reported from rural rainforest regions in Central and Western Africa.
Thus, a monkeypox outbreak occurring in Europe and the United States in 2022 has puzzled virologists and microbiologists because it does not follow the historical pattern of the virus’ spread. For example, the first monkeypox case in the US arrived in May from a Massachusetts patient who had traveled to Canada, a state press release noted.
Before the Nigerian outbreak, the virus rose from rural areas where hunters came in close contact with animals. The illness resulted in lesions on the face, hands, and feet, Nature wrote of Yinka-Ogunleye’s recollections.
However, after 2017, she and other epidemiologists warned peers that the virus was spreading in new ways and in urban settings. For example, infected people sometimes had genital lesions, suggesting that the virus might spread through human sexual contact.
Now, in 2022, “the world is paying the price for not having responded adequately” in 2017, Yinka-Ogunleye told Nature.
Lack of Smallpox Vaccination Increases Monkeypox Challenges
The waning effects of smallpox vaccinations, which ended in 1980 after smallpox was basically eradicated from the world, may have opened the door for monkeypox to spread earlier this year. Smallpox vaccines provided some protection against monkeypox, but by now three generations of people have not received smallpox inoculations.
“Eyebrows were raised when multiple cases of monkeypox were reported from various non-endemic countries starting in May of 2022,” Acharya said. “Due to genetic similarity, smallpox vaccination provided some cross-protection, but the termination of smallpox vaccination could have provided ground for the recent insurgence and spread of monkeypox.”
Trying to jumpstart a new monkeypox vaccination campaign on the heels of COVID-19 shots may be met with resistance from a virus-weary public. But other options at preventing the current spread of monkeypox may present challenges as well, such as trying to curtail sexual activity among affected population, the BBC reported.
“The easiest way to prevent it is to close down all highly active sexual networks for a couple of months until it goes away, but I don’t think that will ever happen. Do you?” Paul Hunter, PhD, Professor of Medicine at the University of East Anglia in Norwich, England, told the BBC.
For medical laboratory workers and others who may find themselves testing for the disease in the future, the biggest lessons from current monkeypox challenges are twofold: The virus has invaded new geography, and discontinued smallpox vaccination campaigns may have left younger people exposed to monkeypox.
Viral reservoir could be behind persistence, says study, which also suggests a blood biomarker could be found for clinical laboratory testing
Microbiologists and virologists working closely with physicians treating long COVID-19 patients will gain new insights in a study that found coronavirus spike protein in COVID-19 patients’ blood up to 12 months after diagnosis. The researchers believe their findings could be used to develop a clinical laboratory biomarker for long COVID-19.
Researchers at Brigham and Women’s Hospital and Massachusetts General Hospital said medical experts are not sure why some people have unwelcome symptoms weeks and months after a positive COVID-19 diagnosis, while others clear the infection without lingering effects.
The scientists believe if this work is validated, clinical laboratories might gain an assay to use in the diagnosis of long COVID-19.
“The half-life of spike protein in the body is pretty short, so its presence indicates that there must be some kind of active viral reservoir,” said David Walt, PhD (above), Professor of Pathology, Brigham and Women’s Hospital, and lead author of the study that found coronavirus spike protein in long COVID patients. The study findings indicate a potential clinical laboratory biomarker for long COVID-19. (Photo copyright: Brigham and Women’s Hospital.)
Viral Reservoir Possibly Behind Long COVID-19
The study suggests that SARS-CoV-2 finds a home in the body, particularly the gastrointestinal tract, “through viral reservoirs, where it continues to release spike protein and trigger inflammation,” Medical News Today reported.
Lead author of the study David Walt, PhD, Professor of Pathology, Brigham and Women’s Hospital and the Hansjörg Wyss Professor Biologically Inspired Engineering at Harvard Medical School, told The Guardian he “was motivated to carry out the study after earlier research by his colleagues detected genetic material from the COVID virus (viral RNA) in stool samples from children with multisystem inflammatory syndrome (a rare but serious condition that often strikes around four weeks after catching COVID) as well as spike protein and a marker of gut leakiness in their blood.”
Long COVID—also known as long-haul COVID, post-COVID-19, or its technical name, post-acute sequelae of COVID-19 or PASC—can involve health problems continuing weeks, months, or even years after a positive diagnosis, according to the federal Centers for Disease Control and Prevention (CDC).
Symptoms of long COVID, according to the researchers, include:
fatigue,
loss of smell,
memory loss,
gastrointestinal distress, and
shortness of breath.
“If someone could somehow get to that viral load and eliminate it, it might lead to resolution of symptoms,” Walt told the Boston Globe, which noted that the researchers may explore a clinical trial involving antiviral drugs for treatment of long COVID-19.
Clues from Earlier Studies on Long COVID-19
Medical conditions that persisted following a COVID-19 infection have been studied for some time. In fact, in an earlier study, Walt and others found children who developed a multisystem inflammation syndrome weeks after being infected by SARS-CoV-2, according to their 2021 paper published in The Journal of Clinical Investigation, titled, “Multisystem Inflammatory Syndrome in Children Is Driven by Zonulin-Dependent Loss of Gut Mucosal Barrier.”
Although these earlier studies provided clues, the cause of PASC remains unclear, the researchers noted. They planned to take a more precise look at PASC biology by using appropriate sampling and patient recruitment.
“Disentangling the complex biology of PASC will rely on the identification of biomarkers that enable classification of patient phenotypes. Here, we analyze plasma samples collected from PASC and COVID-19 patients to determine the levels of SARS-CoV-2 antigens and cytokines and identify a blood biomarker that appears in the majority of PASC patients,” the researchers wrote.
Finding a Marker of a Persistent Infection
The researchers used plasma samples from 63 people with a previous SARS-CoV-2 diagnosis (37 also had PASC), Medical News Today reported. Over a 12-month period, the researchers’ findings included:
Detection in 65% of PASC samples of full-length spike, S1 spike, and nucleocapsid throughout the year of testing.
Spike detected in 60% of PASC patient samples, and not found in the COVID-19 samples.
In an interview with Scientific American, bioengineer Zoe Swank PhD, post-doctoral researcher, Brigham and Women’s Hospital, and co-author of the study, said, “Our main hypothesis is that the spike protein is not causing the symptoms, but it’s just a marker that is released because you still have infection of some cells with SARS-CoV-2.”
In that article, Swank shared the scientists’ intent to do more research involving hundreds of samples over the course of the COVID-19 pandemic from many hospitals and people.
COVID-19 Not the Only Virus That Hangs On
Having a long-haul COVID-19 marker is a “game-changer,” according to an infectious disease expert who was not involved in the study.
“There has not so far been a clear, objective marker that is measurable in the blood of people experiencing long COVID-19,” Michael Peluso, MD, Assistant Professor, Medicine, University of California San Francisco, told Scientific American. “I hope their findings will hold up. It really would make a difference for a lot of people if a marker like this could be validated,” he added.
However, COVID-19 is not the only virus that could persist. Ebola also may linger in areas that skirt the immune system, such as the eye interior and central nervous system, according to a World Health Organization fact sheet.
Thus, medical laboratory leaders may want to follow the Brigham and Women’s Hospital research to see if the scientists validate their finding, discover a biomarker for long-haul COVID-19, and pursue a clinical trial for antiviral drugs. Such discoveries could have implications for how diagnostic professionals work with physicians to care for long COVID patients.