GI pathologists will be interested in how the Endoculus device uses tank-like treads to traverse the gastrointestinal tract, where it can capture images and perform biopsies
Gastroenterologists (GI) may soon gain a useful new tool for use in gathering both biopsies and diagnostic information when examining the gastrointestinal tract. Ongoing development of a new robotic device promises both capabilities using technology that will be of interest to GI pathologists and clinical laboratory scientists.
The minute robotic device uses tank-like treads to traverse the colon. While there, it can capture live images and perform biopsies under the control of a gastroenterologist. The researchers believe the robotic technology will benefit GIs performing the colonoscopies as well as the pathologists called upon to analyze biopsies.
“Currently, endoscopy consists of a gastroenterologist using a semi-rigid, long rope-like device and endoscope to propel through your colon manually,” Gregory Formosa, PhD (above) a member of the AMTL team that developed Endoculus, said in a YouTube video describing the device. “We think that a robotic capsule endoscope can replace conventional endoscopes by making them faster, safer, and more robust than a human operator can do currently with traditional techniques,” he added. (Photo copyright: University of Colorado.)
AMTL researcher Gregory Formosa, PhD, said the team’s goal is to “have a capsule-sized robot that can actively traverse [a patient’s] entire gastrointestinal tract and send out diagnostics in real time, as well as autonomously navigate itself to localize problematic areas within [the] intestinal tract.”
Formosa noted that colorectal cancer is “the third-most fatal and diagnosed cancer in the United States.” But if caught at an early stage, these cancers are “95% treatable,” he added. “So, if we can get people screened early, we definitely can reduce the fatality rate of colorectal cancers significantly.”
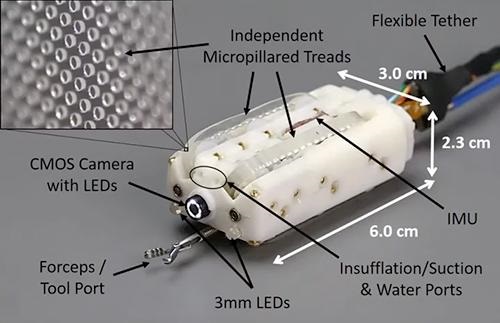
Currently about the size of a C battery, Endoculus (above) is a “fully packed medical device, complete with a camera, an air pump for inflating the colon, a water pump for cleaning, and a tool port for holding biopsy snares,” states a University of Colorado news story, titled, “A Robot May One Day Perform Your Colonoscopy.” (Photo copyright: University of Colorado.)
How Endoculus Works
One key to the device are the four treads, which are designed for traction on digestive tissue.
“You have to forget about everything you know from a locomotion standpoint because driving around inside the body is very different than driving around in a car,” said Rentschler in the University of Colorado news story. “The environment is highly deformable. It’s very slick. There are sharp peaks that you have to go over.”
The university news story noted the current availability of ingestible “pill cams” that can take photos as they travel through the digestive system. But once swallowed, their movements cannot be controlled.
“For our robots to be able to reach those regions that [can be] reached with a pill-cam—but also be able to stop and look around—that could be a big paradigm shift in the way we view these procedures,” said Micah Prendergast, PhD, an AMTL research team member.
Could Biopsies Be Diagnosed In Situ with Endoculus?
The researchers currently view Endoculus as a potentially better way to perform conventional biopsies. But could it lead to bigger advancements?
“Researchers continue to develop devices to help various specialist physicians—in this case GIs—do more when treating patients,” said Dark Daily Publisher and Editor-in-Chief Robert Michel. “This device fits that description. It is designed to improve the ability of GIs to evaluate the colon. Not only does this device do that, but it can also collect a biopsy at sites of interest. In this way, it is a device that can be a benefit to pathologists who will analyze the biopsy.
“With improvements in digital cameras and associated AI-powered analytical tools, the day might not be far off when a device like this can use the camera and artificial intelligence to diagnose the tissue of interest in situ,” he added. “This might create the opportunity for pathologists to be present in the exam room during the procedure, or even viewing the images remotely.
“Not only would that eliminate the need to collect a tissue specimen that must then be sent to a pathology lab, but it would create a new opportunity for pathologists to add value to patient care while shortening the time to diagnosis for the tissue of interest during these procedures,” Michel noted.
Combining robotic-assisted bronchoscopy with rapid on-site evaluation by cytopathologists enables cancer evaluation and diagnosis in one procedure
New technologies are making it possible to both collect a tissue biopsy and diagnose lung cancer during the same procedure. Cytopathologist are essential in this unique approach, which has the potential to greatly shorten the time required to diagnose lung cancer.
At USA Health Mitchell Cancer Institute in Alabama, a team consisting of pulmonology, pathology, surgical, and medical oncology specialists can diagnose lung cancer significantly faster thanks to the combining of a robotic-assisted bronchoscopy (RAB) system with rapid on-site evaluation of biopsies (ROSE) by a cytopathologist during the same procedure.
The RAB platform was created by Auris Health in Redwood City, Calif. According to a USA Health new release, the Auris Health Monarch “enables physicians to see inside the lung and biopsy hard-to-reach nodules using a flexible endoscope. When combined with rapid on-site evaluation (ROSE) it allows for diagnosis at the time of bronchoscopy.”
USA Health says it is the only academic health system in Alabama to combine the Auris Health Monarch (Monarch) with ROSE to diagnose lung cancer in a single procedure.
“Nine-nine percent of the time we make a diagnosis—negative or positive (at time of bronchoscopy). We don’t have to do repeat procedures,” said Elba Turbat-Herrera, MD, Director of Pathological Services at USA Health’s Mitchell Cancer Institute (MCI) and Professor, MCI Interdisciplinary Clinical Oncology, in an exclusive interview with Dark Daily.
The American Society for Cytopathology defines ROSE as “a clinical service provided for patients where a pathologist, or in certain settings, an experienced and appropriately qualified cytotechnologist provides immediate real‐time evaluation of a fine needle aspiration (FNA) biopsy or touch imprints of a core biopsy.”
As a cytopathologist, Turbat-Herrera performs ROSE during procedures at USA Health. “I think we have improved diagnostics very much. With the Monarch equipment, one can see where the needle is traveling in the bronchial tube. It is more precise,” Turbat-Herrera explained.
Patients Benefit from Robotic-assisted Bronchoscopy
Traditionally, anatomic pathologists receive core (tissue sampling) biopsies and fine-needle aspiration biopsies from doctors looking to determine if a lung nodule may be cancerous. But the procedures to secure the biopsies are invasive and stressful for patients waiting for results from clinical laboratories. And some nodules are difficult for surgeons to reach, which can delay care to patients.
“The Monarch and ROSE technologies represent a huge step forward in lung bronchoscopy. Being able to see directly inside the lung and evaluate samples immediately provides the most advanced care for patients,” said Brian Persing, MD (above), Medical Oncologist, Mitchell Cancer Institute, and Assistant Professor of Interdisciplinary Clinical Oncology at the University of South Alabama College of Medicine, in the news release. (Photo copyright: University of South Alabama.)
Currently, more than 112 US healthcare providers use the Monarch robotic-assisted bronchoscopy (RAB) platform, which garnered US Food and Drug Administration (FDA) clearance in 2018, the USA Health news release noted.
The Monarch platform, according to USA Health, “integrates robotics, micro-instrumentation, endoscope design, and data science into one platform to empower physicians.”
Monarch’s “controller-like interface” (seen above) enables physicians to operate the endoscope and access small and “hard-to-reach” lung nodules. “The Monarch platform,” Duluth News Tribune explained, “is an endoscope guided by a handheld controller very similar to an Xbox controller. As the Monarch Platform drives through the lungs, the camera and other diagrams on a screen help the physician locate the nodule, then collect the biopsy with better accuracy and precision.” (Photo copyright: Jed Carlson/Superior Telegram/Duluth News Tribune.)
Eric Swanson, a pulmonologist at Essentia Health-St. Mary’s Medical Center in Duluth, MD, calls Monarch a game changer. “It’s a big, big upgrade from what we had before,” Swanson told the Duluth News Tribune. “(Before), you’d just pass a small catheter through a regular bronchoscope, and you turn it and hope you land in the right spot.”
The Monarch platform has enabled USA Health to step-up diagnosis of lung cancer, as compared to FNA (fine needle aspiration) biopsy on its own, according to Turbat-Herrera.
“With FNA alone, you try to get (sample tissue), and you are not sure. Now, if it is there, you should get it because the (Monarch) equipment helps you get there. Our role in pathology is to help guide the hand of the pulmonologist: ‘you don’t have what we need,’ or ‘keep going in that area of the lung,’” she said, adding that physicians have been able to reach tiny lesions.
High Incidence of Lung Cancer
The American Cancer Society, says lung cancer is the second most common cancer, with an estimated 235,760 new lung cancer cases and 131,880 deaths from the disease in 2021.
It’s hoped that healthcare providers’ investment in new robotic technology—such as Monarch and others—may shorten the time required to diagnose lung cancer and eventually save lives.
Providers such as USA Health go a step further by integrating ROSE with RAB. The robotic technology—coupled with on-site rapid evaluation by a cytopathologist that averts repeat biopsy procedures—immediately secures an assessment of sample adequacy and a cancer diagnosis that may benefit patients as well.
This is yet another example of how a new technology in one field can have a benefit for anatomic pathologists.
MIT’s deep learning artificial intelligence algorithm demonstrates how similar new technologies and smartphones can be combined to give dermatologists and dermatopathologists valuable new ways to diagnose skin cancer from digital images
According to an MIT press release, “The paper describes the development of an SPL [Suspicious Pigmented Lesion] analysis system using DCNNs [Deep Convolutional Neural Networks] to more quickly and efficiently identify skin lesions that require more investigation, screenings that can be done during routine primary care visits, or even by the patients themselves. The system utilized DCNNs to optimize the identification and classification of SPLs in wide-field images.”
The MIT scientists believe their AI analysis system could aid dermatologists, dermatopathologists, and clinical laboratories detect melanoma, a deadly form of skin cancer, in its early stages using smartphones at the point-of-care.
“Our research suggests that systems leveraging computer vision and deep neural networks, quantifying such common signs, can achieve comparable accuracy to expert dermatologists,” said Luis Soenksen, PhD (above), Venture Builder in Artificial Intelligence and Healthcare at MIT and first author of the study in an MIT press release. “We hope our research revitalizes the desire to deliver more efficient dermatological screenings in primary care settings to drive adequate referrals.” The MIT study demonstrates that dermatologists, dermatopathologists, and clinical laboratories can benefit from using common technologies like smartphones in the diagnosis of disease. (Photo copyright: Wyss Institute Harvard University.)
Improving Melanoma Treatment and Patient Outcomes
Melanoma develops when pigment-producing cells called melanocytes start to grow out of control. The cancer has traditionally been diagnosed through visual inspection of SPLs by physicians in medical settings. Early-stage identification of SPLs can drastically improve the prognosis for patients and significantly reduce treatment costs. It is common to biopsy many lesions to ensure that every case of melanoma can be diagnosed as early as possible, thus contributing to better patient outcomes.
“Early detection of SPLs can save lives. However, the current capacity of medical systems to provide comprehensive skin screenings at scale are still lacking,” said Luis Soenksen, PhD, Venture Builder in Artificial Intelligence and Healthcare at MIT and first author of the study in the MIT press release.
The researchers trained their AI system by using 20,388 wide-field images from 133 patients at the Gregorio Marañón General University Hospital in Madrid, as well as publicly available images. The collected photographs were taken with a variety of ordinary smartphone cameras that are easily obtainable by consumers.
They taught the deep learning algorithm to examine various features of skin lesions such as size, circularity, and intensity. Dermatologists working with the researchers also visually classified the lesions for comparison.
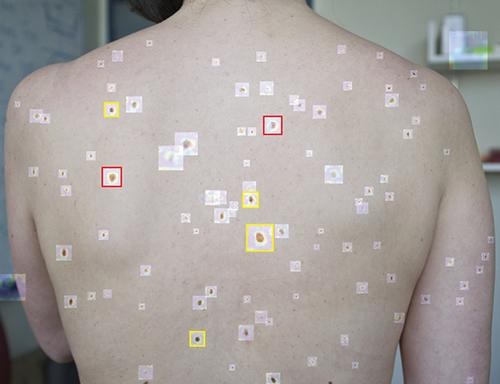
When the algorithm is “shown” a wide-field image like that above taken with a smartphone, it uses deep convolutional neural networks to analyze individual pigmented lesions and screen for early-stage melanoma. The algorithm then marks suspicious images as either yellow (meaning further inspection should be considered) or red (indicating that further inspection and/or referral to a dermatologist is required). Using this tool, dermatopathologists may be able to diagnose skin cancer and excise it in-office long before it becomes deadly. (Photo copyright: MIT.)
“Our system achieved more than 90.3% sensitivity (95% confidence interval, 90 to 90.6) and 89.9% specificity (89.6 to 90.2%) in distinguishing SPLs from nonsuspicious lesions, skin, and complex backgrounds, avoiding the need for cumbersome individual lesion imaging,” the MIT researchers noted in their Science Translational Medicine paper.
In addition, the algorithm agreed with the consensus of experienced dermatologists 88% of the time and concurred with the opinions of individual dermatologists 86% of the time, Medgadget reported.
Modern Imaging Technologies Will Advance Diagnosis of Disease
According to the American Cancer Society, about 106,110 new cases of melanoma will be diagnosed in the United States in 2021. Approximately 7,180 people are expected to die of the disease this year. Melanoma is less common than other types of skin cancer but more dangerous as it’s more likely to spread to other parts of the body if not detected and treated early.
More research is needed to substantiate the effectiveness and accuracy of this new tool before it could be used in clinical settings. However, the early research looks promising and smartphone camera technology is constantly improving. Higher resolutions would further advance development of this type of diagnostic tool.
In addition, MIT’s algorithm enables in situ examination and possible diagnosis of cancer. Therefore, a smartphone so equipped could enable a dermatologist to diagnose and excise cancerous tissue in a single visit, without the need for biopsies to be sent to a dermatopathologist.
Currently, dermatologists refer a lot of skin biopsies to dermapathologists and anatomic pathology laboratories. An accurate diagnostic tool that uses modern smartphones to characterize suspicious skin lesions could become quite popular with dermatologists and affect the flow of referrals to medical laboratories.
According to the Centers for Disease Control and Prevention (CDC), the 1918 influenza (aka, the Spanish Flu) pandemic took place worldwide between 1918 and 1919. It was caused by the H1N1 virus (A/H1N1), a subtype of the Influenza A virus, and infected approximately 500 million people worldwide (a third of the human population at the time). Fifty million people died. Many were children or otherwise healthy individuals, but people from all age groups perished.
The CDC calls the Spanish Flu the “deadliest pandemic of the 20th century.” Past pandemics have generally concluded after 2.5 to 3.5 years. That’s how long it takes for new viruses to mutate and become endemic diseases, Healthline reported.
The COVID-19 pandemic has been around for about that long. It stands to reason the natural end of the COVID-19 pandemic may be just around the corner. But is it? And is the Omicron variant an indicator that the COVID-19 pandemic is winding down?
“Our analysis suggests that in the US, this combination of characteristics would lead to Omicron replacing Delta as the dominant variant in the next few months and to a higher peak burden of disease than the country saw in the second half of 2021 (but likely below the peak reached in the winter of 2020-21),” the report states.
McKinsey analysts also acknowledged the possible impact of new therapeutics, COVID-19 vaccine booster doses, and public health measures on Omicron spread. “In the short term, an accelerated rollout of booster doses of COVID-19 vaccines is likely to be one of the best protections against an Omicron-fueled wave of the disease,” the analysts wrote.
Does How the Spanish Flu Came to an End Mirror the COVID-19 Pandemic?
Virologists and infectious disease experts explained that the Spanish Flu virus did what viruses still do: mutate and become less dangerous. Herd immunity also helped end the 1918 pandemic.
“The 1918 influenza virus eventually mutated to the point of not having a high number of deaths—eventually over three years or so. We may very well be witnessing this process with ongoing variants of SARS-CoV-2,” virologist Rodney Rohde, PhD, Director of the Clinical Laboratory Science Program at Texas State University, told Healthline.
Today’s flu strains have “ancestral links” to the 1918 flu, and thus, the SARS-CoV-2 coronavirus will most likely also leave its mark, The Boston Herald reported. “The coronavirus will evolve and hopefully morph into a seasonal illness to which we pay little mind, but it’s still too early to tell,” Todd Ellerin, MD (above,) Director of Infectious Diseases, South Shore Health, South Weymouth, Mass., told The Boston Herald. (Photo copyright: Greg Derr/The Patriot Ledger.)
“If you think about the way viruses behave, biologically, their reason for living is to replicate and spread, and there’s really no advantage for the virus to kill the host,” infectious disease specialist Keith Armitage, MD, Professor of Medicine, Division of Infectious Diseases at Case Western Reserve University, told Healthline. “The hope is, that if the pandemic doesn’t go away, we will get new variants that are highly contagious but don’t produce much of a clinical illness,” he added.
In “2021’s Top 10 Lab Stories Confirm Important Trends,” Dark Daily’s sister publication, The Dark Report (TDR), posed a similar question in its number one story of 2021: “COVID-19: Will it Become Endemic and a Respiratory Virus that Shows Up Every Year like Influenza?”
“The question of whether SARS-CoV-2 is a pandemic that fades, as did SARS in 2003, or becomes endemic and a respiratory virus that shows up every season like influenza and the common cold, is of major concern to clinical lab administrators. That’s because clinical labs and pathology groups must continue to serve physicians and patients with the usual menu of routine, reference, and esoteric testing,” TDR noted.
Clinical Laboratories to Continue COVID Testing
It would be most helpful for medical laboratories and pathology groups to have some idea of when the pandemic will end. Unfortunately, such predictions would not be very useful.
“Since COVID-19 infections have a high number of asymptomatic transmitters, we may not fully understand how societal and environmental pressures—masks, distancing, remote working, etc.—on the virus will allow it to evolve,” Rohde told Healthline.
For now, clinical laboratories will need to continue to remain prepared as COVID-19 cases rise and people seek SARS-COV-2 tests, vaccinations, and treatments. COVID-19 testing is likely to be in demand throughout the coming year. The current surge in demand for COVID-19 tests is putting additional stress on the supply chain.
“We know pandemics end; it’s just a matter of time,” Sara Paton, PhD, Associate Professor of Epidemiology, Wright State University, told the Journal-News. “It could be in 2022, maybe later in the year, but I can’t say for sure. It could be 2023.”
Teams from multiple Swedish organizations are investigating the relationship of protein-coding genes to antibodies
Scientists in Sweden are discovering new ways to map the expression of genes in cells, tissues, and organs within the human body thanks to advances in molecular profiling. Their study has successfully combined the analysis of single-cell transcriptomics with spatial antibody-based protein profiling to produce a high-resolution, single-cell mapping of human tissues.
The data links protein-coding genes to antibodies, which could help researchers develop clinical laboratory tests that use specific antibodies to identify and target infectious disease. Might this also lead to a new menu of serology tests that could be used by medical laboratories?
This research is another example of how various databases of genetic and proteomic information—different “omics”—are being combined to produce new understanding of human biology and physiology.
In a Human Protein Atlas (HPA) project press release, Director of the HPA consortium and Professor of Microbiology at Royal Institute of Technology in Stockholm, Mathias Uhlén, PhD, said, “The [Science Advances] paper describes an important addition to the Human Protein Atlas (HPA) which has become one of the world’s most visited biological databases, harboring millions of web pages with information about all the human protein coding genes.”
“We are excited that the new open-access Single Cell Type section constitutes a unique resource for studying the cell type specificity and exact spatial localization of all our proteins”, said Cecilia Lindskog, PhD (above), Head of the HPA Tissue Atlas and Associate Professor, Experimental Pathology, Uppsala University, in the Protein Atlas press release. Medical laboratories may soon have new serology tests to perform that were developed based on HPA data. (Photo copyright: Human Uterus Cell Atlas.)
Distinct Expression Clusters Consistent to Similar Cell Types
To perform their research, the scientists mapped the gene expression profile of all protein-coding genes across different cell types. Their analysis showed that there are distinct expression clusters which are consistent to cell types sharing similar functions within the same organs and between organs of the human body.
The scientists examined data from non-diseased human tissues and organs using three main criteria:
Publicly available raw data from human tissues containing good technical quality with at least 4,000 cells analyzed and at least 20 million read counts by the sequencing for each tissue.
High correlation between pseudo-bulk transcriptomics profile from the scRNA-Seq data and bulk RNA-Seq generated as part of the Human Protein Atlas (HPA).
High correlation between the cluster-specific expression and the expected expression pattern of an extensive selection of marker genes representing well-known tissue- and cell type-specific markers, including both markers from the original publications and additional markers used in pathology diagnostics.
According to the HPA press release, “across all analyzed cell types, almost 14,000 genes showed an elevated expression in particular cell types, out of which approximately 2,000 genes were found to be specific for only one of the cell types.”
The press release also states, “cell types in testis showed the highest numbers of cell type elevated genes, followed by ciliated cells. Interestingly, only 11% of the genes were detected in all analyzed cell types suggesting that the number of essential genes (‘house-keeping’) are surprisingly few.”
Omics-based Biomarkers for Accurate Diagnosis of Disease
The Human Protein Atlas is the largest and most comprehensive database for spatial distribution of proteins in human tissues and cells. It provides a valuable tool for researchers who study and analyze protein localization and expression in human tissues and cells.
Ongoing improvements in gene sequencing technologies are making research of genes more accurate, faster, and more economical. Advances in gene sequencing also could help medical professionals discover more personalized care for patients leading to improved outcomes. A key goal of precision medicine.
One of the conclusions to be drawn from this work is that clinical laboratories and anatomic pathology groups will need to be able to handle immense amounts of data, while at the same time having the capabilities to analyze that data and identify useful patterns that can help diagnose patients earlier and more accurately.
Survey shows more than 50% of hospitals and health systems plan to increase virtual care services within two years, a development that can change how patients access clinical laboratory testing services
If anything positive came out of the COVID-19 pandemic, it’s the growing acceptance by physicians and health payers of telehealth—including telepathology, teleradiology, and other types of virtual doctor visits—as a way for patients to meet with their physicians in place of in-office healthcare.
In earlier coverage about the rapid adoption of telehealth and virtual doctor visits, Dark Daily has observed that this trend creates a unique challenge for clinical laboratories. If the patient has a virtual consultation with his or her physician, how would a clinical laboratory get access to this patient to do a venipuncture and collect the samples necessary to perform the medical laboratory tests ordered by the physician?
Nevertheless, according to multiple reports, healthcare providers are planning to increase investment in telehealth technologies.
Disparate Technologies Led to Technical Difficulties for Virtual Healthcare Providers
The terms telemedicine and telehealth are often used interchangeably. However, according to the American Academy of Family Physicians (AAFP), there are subtle differences worth noting.
Telehealth is a broad term which refers to “electronic and telecommunications technologies and services used to provide care and services at-a-distance [while] telemedicine is the practice of medicine using technology to deliver care at a distance.
“Telehealth is different from telemedicine in that it refers to a broader scope of remote health care services than telemedicine. Telemedicine refers specifically to remote clinical services, while telehealth can refer to remote non-clinical services,” the AAFP notes.
Kelly Lewis, former Vice President of Revenue Strategy and Enablement at telehealth provider Amwell, told Healthcare IT News (HIT News) that “the COVID-19 pandemic caused telehealth adoption to skyrocket.
However, “Because much of this adoption was driven out of an abundance of necessity, there was little time for organizations to think strategically about their technology investments,” she added.
“With urgency at a high, payers, provider organizations and clinicians all turned to the quickest options available so patients could continue to get care. The result, however, was what we are calling platform ‘sprawl’—the use of a number of disparate solutions that are leading to a confusing and frustrating care delivery system and experience.”
Nevertheless, according to a survey conducted by HIT News and HIMSS Analytics, “More than half (56%) of hospital and health system leaders say they are planning to increase their investment in telemedicine during the next two years.” This, “shows that the huge surge in and mainstreaming of telehealth during the ongoing pandemic has caused the C-suite and other healthcare leaders to embrace the technology that has for so long existed on the periphery of medicine,” HIT News noted.
“The clear message is that telehealth is here to stay and will continue to expand,” Lewis told HIT News, adding, “The majority of payers without virtual care offerings also reported planning to add them in the next 24 months.”
“Clinicians agree that moving toward a fully integrated telehealth platform would be beneficial. More than 80% believe investing in a fully integrated virtual or hybrid care system would have a positive impact on clinical outcomes and patient experiences,” Kelly Lewis (above), former VP at telehealth provider Amwell, told Healthcare IT News. Considering the growing demand for telehealth, pathologists and clinical laboratories will need a strategy for supporting virtual healthcare providers. (Photo copyright: Healthcare IT News.)
The HIT News/HIMSS Analytics survey findings suggest telehealth will transition as providers aim for “smart-growth” instead of “pandemic-fueled expediency,” Becker’s Hospital Review reported.
Survey respondents expressed positive attitudes about telehealth:
56% of healthcare leaders plan to increase investment in virtual care over the next two years.
80% of respondents noted “very” or “extremely” important telehealth factors are integrating with existing workflows, fast video connections, and reducing administrative burden.
77% called telehealth platform integration with the electronic health record (EHR) “very” or “extremely” important.
80% envision positive clinical outcomes and patient experiences from a fully integrated telemedicine platform.
75% of payers said a single digital platform has potential to streamline member experiences.
“With telehealth visits stabilizing at roughly 10 times pre-pandemic levels, digital transformation initiatives are rising across the field. As a result of the pandemic, 60% of healthcare organizations are adding new digital projects, with telemedicine becoming a higher priority for 75% of executives (vs. 42% in 2019) to improve the patient experience,” the AHA reported.
Medical laboratories and anatomic pathology groups are advised to keep pace with the changing healthcare landscape which increasingly puts a premium on remote and virtual visits. This has become even more critical as healthcare providers and investors infuse more capital into telehealth technology.
As physicians expand telemedicine virtual office visits post-pandemic, a clinical laboratory strategy to reach patients and acquire specimens will be required.