Self-insured and campus health markets are contract opportunities for small and midsize clinical laboratories through investment in data infrastructure and management
Bordenave spoke this week at the Executive War College in San Antonio. During two intriguing presentations, she shared that the self-insured employer and campus health markets are areas of opportunity for small and midsize clinical laboratories. This is because employer groups and college campuses are busy communities of covered individuals, and these population health groups are well-suited for proactive care models.
In fact, she said, some clinical laboratories may already be well-positioned to serve these customers.
Self-Insured Employer Groups and Campus Health Markets as New Clinical Laboratory Customers
According to CMS national health expenditure data, in 2020, a whopping $4 trillion was spent on healthcare in the US. In the middle of all that are people living, going to school, and working who have high blood pressure, rising lipid levels, lower-back pain, migraines, and other health conditions waiting to be diagnosed and flagged for follow-up.
And as pathologists and clinical laboratory managers know, 80% of those healthcare encounters result in lab test data.
Clinical laboratories, therefore, can gain customers among self-insured employer groups and similarly functioning campus health markets that serve students.
During her presentations at the 2021 Executive War College in San Antonio, Kristine Bordenave, MD, FACP (above), a strategic consultant in precision medicine, population health, Medicare compliance, and cost management, noted that “just about all paths forward post-COVID will require the data infrastructure of clinical laboratories to achieve an advanced level of functionality.” (Photo copyright: The Dark Intelligence Group.)
In one example she gave during her presentation, Bordenave noted that self-insured employer groups “were more than willing to contract directly, and they were contracting for care that directly relates to lab. Anything that would help reduce presenteeism and absenteeism with their employees.”
Presenteeism and Absenteeism
For years, presenteeism and absenteeism have plagued employee productivity in organizations large and small. Both have been attributed to numerous individual health and wellness factors among individuals. At some point, these issues culminate into various forms of reactive healthcare services and safety issues, she added.
The cost of presenteeism is estimated at between $150 billion and $225 billion. Meanwhile, at least 60% of employees are now covered in fully-funded or partially-funded self-insured plans, Healthcare Finance reported.
The way a campus health system operates is similar to a self-insured model but more of an integrated delivery system, Bordenave said. Among the priorities are controlling the spread of infectious diseases, such as COVID-19 and measles.
Clinical Laboratory Data Valuable in Treating-to-Goal and Closing Care Gaps
During two featured Executive War College general session discussions, Bordenave explained the focus of her work: aligning primary care with the clinical laboratory to treat-to-goal and close care gaps.
“There was a lot of focus on us taking laboratory information and treating people to goal, and that was with respect to diabetes, cholesterol, and hypertension, because those are three common diseases that exist within their [employee] populations. [Primary care doctors] know [that] if they [can] maximize the care in those patients—so that the patient is maximally treated—that patient performs. There’s a lot of literature around this.”
In the state of New Mexico where Bordenave’s project evolved, a culture of innovation prevails, where like-minded people have an opportunity to “do the unique,” she explained. The state’s population is spread out, there is a shortage of healthcare providers, and people generally lack access to health services and other social determinants of health. The liberty to think outside the box—to ensure care in creative ways—was essential to the success of Bordenave’s project.
“Blue Cross Blue Shield paid handsomely for improving healthcare outcomes in diabetes,” she said, adding, “and we never did a standard visit with any of those patients, ever. Then we got paid by a big employer group to do the same thing for them.”
Future of Clinical Laboratory Functionality
Bordenave noted that just about all paths forward post-COVID will require the data infrastructure of clinical laboratories to achieve an advanced level of functionality. Dark Daily will cover more opportunities for labs to capitalize on their structured data in future ebriefings.
Executive War College is scheduled to reconvene April 27-28, 2022, in New Orleans. In the meantime, recordings of this year’s presentations will be available for download, including:
A Roundtable Discussion on Current Activity Involving Clinical Laboratory and Pathology Mergers and Acquisitions.
Taking a Deeper Dive into How Artificial Intelligence Analyzes a Digital Pathology Image: What Current Technology Can and Cannot Do, Steps to Implement, and Understanding How the FDA Views AI in Digital Pathology.
Open Conversation About the Healthcare Data Aggregation Hub Model.
And more.
To learn about Executive War College’s complete program package, send an email request to info@darkreport.com.
Under-resourced British healthcare system faces a record high backlog of care with 5.61 million people in England waiting for hospital-based medical procedures
Healthcare in the United Kingdom (UK) is about to become much more expensive. The UK government has announced plans to substantially increase payroll taxes to fund the surging demand for care due to the COVID-19 pandemic. But that may only be the part of the healthcare-funding iceberg visible above the surface. Below the surface is a healthcare system where wait times for access to many types of care—including cancer diagnoses—are already unacceptable.
Some pathologists and medical laboratory executives in the US who have long questioned healthcare reformers’ desire to introduce an NHS-like single-payer healthcare system in this country will not be surprised to learn that the UK’s notoriously underfunded National Health Service (NHS) is facing a record waitlist for hospital-based medical diagnostic tests and procedures.
Consequently, Reuters reported, the high cost of fighting the COVID-19 pandemic has pushed British Prime Minister Boris Johnson into breaking with election promises and announcing plans to raise payroll taxes to record levels so that more money can be funneled into the struggling government-run healthcare system.
Speaking to lawmakers in the House of Commons, British Prime Minister Boris Johnson (above) acknowledged his tax plan breaks his Conservative Party’s election year pledge to not raise VAT (value-added tax), income, or national insurance taxes. He insists that the COVID-19 pandemic created unprecedented challenges for the national health system. “I accept that this breaks a manifesto commitment, which is not something I do lightly, but a global pandemic was in no one’s manifesto,” he told lawmakers, Reuters reported. (Photo copyright: The Independent.)
5.6M People on Growing NHS Waiting List for Treatments and Procedures
When the COVID-19 pandemic struck the UK in March 2020, the NHS suspended elective surgeries such as hip or knee replacements and cataract removal and postponed many patients’ medical laboratory diagnostic tests.
In “Record 5.6M People in England Waiting for Hospital Treatment,” The Guardian estimated that 1.4 million patients were added to the waiting lists during the pandemic’s first 18 months. More than one-third of the 5.6 million people waiting for care in July 2021 had been on a waitlist for at least 18 months, the paper noted. Since then, the waiting list has grown by 150,000 people per month, as more people who did not seek or could not access NHS treatments during the pandemic returned to their doctors’ offices.
Johnson’s tax hike formula for fixing the record NHS backlog and improving social care for the elderly created shockwaves in the UK’s Conservative Party, which, like the Republican Party in this country, has championed low taxes. But Johnson maintains the government is out of options.
“It would be wrong for me to say that we can pay for this recovery without taking the difficult but responsible decisions about how we finance it,” Johnson told Parliament. “It would be irresponsible to meet the costs from higher borrowing and higher debt,” he added.
But Johnson’s proposal drew the wrath of some members of his own party and provided the opposition Labor Party with ammunition to denounce the prime minister’s leadership during the pandemic.
In “U.K. Is Among First Western Nations to Increase Taxes to Cover COVID-19 Costs,” The Wall Street Journal (WSJ) reported that Labor Party leader Keir Starmer compared Johnson’s tax increases to putting a bandage “on gaping wounds that his party inflicted,” and questioned why they weren’t levied more directly on the rich. The UK government says the wealthiest 14% will pay about half of the extra tax revenues, the WSJ noted.
“This is a tax rise that breaks a promise that the prime minister made at the last election … Read my lips, the Tories can never again claim to be the party of low tax,” Starmer told Reuters.
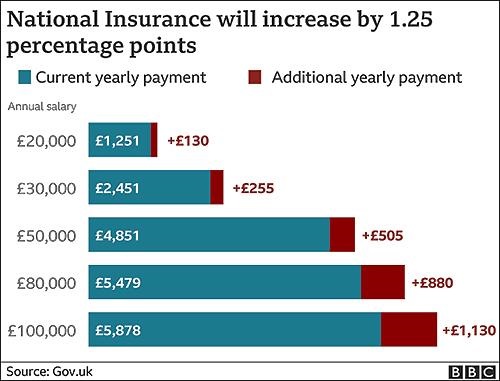
The BBC graphic above illustrates how the tax hikes, which were approved by the Parliament on September 8 by a 319 to 248 vote, will increase the national insurance payroll tax paid by workers and employers by 1.25% each. CNBC reported that the UK government projects the increased taxes will raise £36 billion (US$49.6 billion) over the next three years. (Graphic copyright: BBC.)
Politics versus Hard Facts
According to The Guardian, in 2023-2024, national insurance contributions will be rebranded as a health and social care levy, with more of the money raised going to social care. The added funding will enable the UK government to implement a new cap on total care costs so that no individual will pay more than £86,000 (US$117,142) over their lifetime for social-care programs. Currently, many seniors are forced to sell their homes to meet unexpected care costs, the newspaper noted.
“One message to voters and investors is that taxes are set to rise for years to come,” the WSJ editorial board wrote, predicting the cost of social care will escalate as the UK’s population ages, and that the planned diversion of future taxes for social care will be presented as a “cut” in NHS funding. They maintained that the danger in Johnson’s decision goes deeper than breaking an election campaign pledge or nationalizing more of the UK’s healthcare economy.
“The larger problem is that national healthcare and other entitlements become ever more unaffordable even as they are politically impossible to reform,” the newspaper stated. “The Tories are becoming tax collectors for the entitlement state, which is deadly for parties of the right.”
Bloomberg noted that the UK Institute for Fiscal Studies predicts the planned April 1 tax increase will “raise the UK tax burden to its highest-ever sustained level since records began in 1955—about 35% of national income.”
But, according to the UK-based The Health Foundation, at £2,646.95 (US$3,648.43) per person in 2019, the United Kingdom spends less on healthcare than many developed countries. Less per person than the:
US (£6,782.80),
Germany (£4,131.21),
France (£3,307.54),
Japan (£2,949.19) and
Canada (£2,823.07).
And when healthcare costs are viewed as a percentage of a country’s gross domestic product (GDP), the UK (8% GDP) lags behind the US (13.9%), Germany (9.9%), Japan (9.3%) and France (9.3%) and exceeds only Canada (7.6%) and Italy (6.4%).
While US hospitals, healthcare systems, and patients continue to struggle with ever-increasing healthcare costs, reformers who promote a single-payer healthcare system as an answer to this nation’s healthcare ills may want to take a hard look at the outcomes of the UK’s model.
Clinical laboratory managers and pathologists interested in how the US healthcare system can be improved might be well-served to study the experience of the National Health Service in the UK, that, like all other health systems in the world, has its own unique methods for how it serves its population.
Proteins in human saliva make up its proteome and may be the key to new, precision medicine diagnostics that would give clinical pathologists new capabilities to identify disease
Clinical pathologists may soon have an array of new precision medicine diagnostic tools based on peoples’ saliva. There are an increasing number of “–omes” that can be the source of useful diagnostic biomarkers for developing clinical laboratory tests. The latest is the world’s first saliva protein biome wiki.
Called the Human Salivary Proteome Wiki (HSP Wiki), the “public data platform,” which was created by researchers at the University of Buffalo, is the “first of its kind,” according to Labroots, and “contains data on the many thousands of proteins present in saliva.”
The HSP Wiki brings together data from independent studies on proteins present in human saliva. One of the researchers’ goals is to speed up the development of saliva-based diagnostics and personalized medicine tools.
In “The Human Salivary Proteome Wiki: A Community-Driven Research Platform,” published in the Journal of Dental Research, the researchers wrote, “Saliva has become an attractive body fluid for on-site, remote, and real-time monitoring of oral and systemic health. At the same time, the scientific community needs a saliva-centered information platform that keeps pace with the rapid accumulation of new data and knowledge by annotating, refining, and updating the salivary proteome catalog.
“We developed the Human Salivary Proteome (HSP) Wiki as a public data platform for researching and retrieving custom-curated data and knowledge on the saliva proteome. … The HSP Wiki will pave the way for harnessing the full potential of the salivary proteome for diagnosis, risk prediction, therapy of oral and systemic diseases, and preparedness for emerging infectious diseases,” they concluded.
“This community-based data and knowledge base will pave the way to harness the full potential of the salivary proteome for diagnosis, risk prediction, and therapy for oral and systemic diseases, and increase preparedness for future emerging diseases and pandemics,” Stefan Ruhl, DDS, PhD (above right, with Omer Gokcumen, PhD, Associate Professor of Biological Sciences on left), Professor, Department of Oral Biology, University of Buffalo, and lead researcher of the study, told Labroots. Development of precision medicine clinical laboratory diagnostics is part of their research goals. (Photo copyright: University of Buffalo.)
Where Does Saliva Come From?
Saliva is a complex biological fluid that has long been linked to oral health and the health of the upper gastrointestinal tract. Only recently, though, have scientists begun to understand from where in the body saliva proteins originate.
The authors wrote: “Salivary proteins are essential for maintaining health in the oral cavity and proximal digestive tract, and they serve as potential diagnostic markers for monitoring human health and disease. However, their precise organ origins remain unclear.
“Through transcriptomic analysis of major adult and fetal salivary glands and integration with the saliva proteome, the blood plasma proteome, and transcriptomes of 28+ organs, we link human saliva proteins to their source, identify salivary-gland-specific genes, and uncover fetal- and adult-specific gene repertoires,” they added.
“Our results pave the way for future investigations into glandular biology and pathology, as well as saliva’s use as a diagnostic fluid,” the researchers concluded.
Saliva plays a crucial role in digestion by breaking down starches. It also provides a protective barrier in the mouth. When salivary glands malfunction, patients can face serious health consequences. Although clinicians and scientists have long understood the importance of saliva to good health, the question now is whether it contains markers of specific diseases.
“The Human Salivary Proteome Wiki contains proteomic, genomic, transcriptomic data, as well as data on the glycome, sugar molecules present on salivary glycoproteins. New data goes through an interdisciplinary team of curators, which ensures that all input data is accurate and scientifically sound,” noted Labroots.
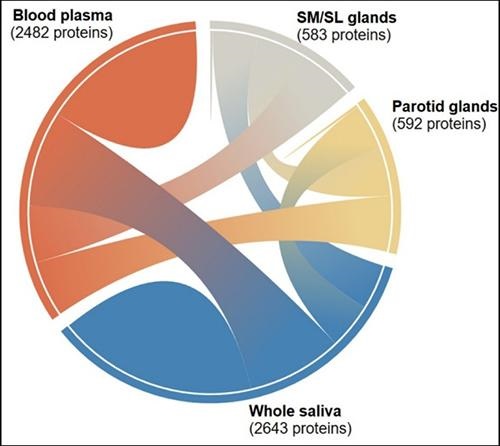
The graphic above “shows the interconnectedness of the thousands of salivary proteins originating from blood plasma, parotid glands, and submandibular and sublingual glands. The diagram is one of many tools available to researchers and clinicians through the Human Salivary Proteome Wiki,” noted a UBNow blog post. (Graphic copyright: University of Buffalo.)
Omics and Their Role in Clinical Laboratory Diagnostics
Proteomics is just one of several hotly-researched -omics that hold the potential to develop into important personalized medicine and diagnostics tools for pathologists. Genomics is a related area of research being studied for its potential to benefit precision medicine diagnostics.
However, unlike genomes, which do not change, proteomes change constantly. That is one of the main reasons studying the human salivary proteome could lead to valuable diagnostics tools.
Combining the study of the -omes with tools like mass spectrometry, a new era of pathology may be evolving. “With the rapid decrease in the costs of omics technologies over the past few years, whole-proteome profiling from tissue slides has become more accessible to diagnostic labs as a means of characterization of global protein expression patterns to evaluate the pathophysiology of diseases,” noted Pathology News.
Saliva and the Age of Precision Medicine
The study of the -omes may be an important element in the evolution of precision medicine, because of its ability to provide information about what is happening in patients’ bodies at the point of care.
Thus, a full understanding of the proteome of saliva and what causes it to change in response to different health conditions and diseases could open the door to an entirely new branch of diagnostics and laboratory medicine. It is easy and non-invasive to gather and, given that saliva contains so much information, it offers an avenue of study that may improve patients’ lives.
It also would bring us closer to the age of precision medicine where clinical laboratory scientists and pathologists can contribute even more value to referring physicians and their patients.
The discovery is yet another factor that must be considered when developing a liquid biopsy test clinical laboratories can use to detect cancer
How often do disruptive elements present in Liquid biopsies result in misdiagnoses and unhelpful drug therapies for cancer? Researchers at the University of Washington School of Medicine (UW Medicine) in Seattle wanted to know. And the results of their study provide another useful insight for pathologists about the elements that circulate in human blood which must be understood so that liquid biopsy tests can be developed that are not affected by that factor.
Based on their case series study of 69 men with advanced prostate cancer, the UW Medicine researchers determined that 10% of men have a clonal hematopoiesis of indeterminate potential (CHIP) that can “interfere” with liquid biopsies and cause incorrect reports and unneeded prostate cancer treatment, according to their paper published in the journal JAMA Oncology.
The UW Medicine researchers advised testing for “variants in the cell-free DNA (cfDNA)” shed in blood plasma to enable appropriate treatment for people with already diagnosed prostate cancer, noted to a UW Medicine news release.
According to pathologist Colin Pritchard, MD, PhD, Associate Professor of Laboratory Medicine and Pathology at the UW Medicine, who led the research team, “clonal hematopoiesis can interfere with liquid biopsies. For example, mutations in the genes BRCA1, BRCA2, and ATM have been closely linked to cancer development.
“The good news is that, by looking at the blood cellular compartment, you can tell with pretty good certainty whether something is cancer, or something is hematopoiesis,” he said in the news release.
What Does CHIP Interference Mean to a Clinical Laboratory Blood Test?
In their published study, the UW Medicine researchers stressed the “urgent need to understand cfDNA testing performance and sources of test interferences” in light of recent US Food and Drug Administration (FDA) clearance of two PARP inhibitors (PARPi) for prostate cancer:
“We found that a strikingly high proportion of DNA repair gene variants in the plasma of patients with advanced prostate cancer are attributable to CHIP,” the researchers wrote. “The CHIP variants were strongly correlated with increased age, and even higher than expected by age group.
“The high rate of CHIP may also be influenced by prior exposure to chemotherapy,” they added. “We are concerned that CHIP interference is causing false-positive cfDNA biomarker assessments that may result in patient harm from inappropriate treatment, and delays in delivering alternative effective treatment options.
“Without performing a whole-blood control, seven of 69 patients (10%) would have been misdiagnosed and incorrectly deemed eligible for PARP-inhibitor therapy based on CHIP interference in plasma. In fact, one patient in this series had a BRCA2 CHIP clone that had been previously reported by a commercial laboratory testing company with the recommendation to use a PARPi. To mitigate these risks, cfDNA results should be compared to results from whole-blood control or tumor tissue,” the researchers concluded.
To find the clinically relevant CHIP interference in prostate cancer cfDNA testing, researchers used the UW-OncoPlex assay (developed and clinically available at UW Medicine). The assay is a multiplexed next-generation sequencing panel aimed at detecting mutations in tumor tissues in more than 350 genes, according to the UW Medicine Laboratory and Pathology website.
“To improve cfDNA assay performance, we developed an approach that simultaneously analyzes plasma and paired whole-blood control samples. Using this paired testing approach, we sought to determine to what degree CHIP interferes with the results of prostate cancer cfDNA testing,” the researchers wrote in JAMA Oncology.
Men May Receive Unhelpful Prostate Cancer Drug Therapies
The research team studied test results from 69 men with advanced prostate cancer. They analyzed patients’ plasma cfDNA and whole-blood control samples.
Tumor sequencing enabled detection of germline (cells relating to preceding cells) variants from CHIP clones.
The UW Medicine study suggested CHIP variants “accounted for almost half of the somatic (non-germline) DNA repair mutations” detected by liquid biopsy, according to the news release.
> “About half the time when the plasma is thought to contain a mutation that would guide therapy with these drugs, it actually contains CHIP variants, not prostate cancer DNA variants. That means that in about half of those tested, a patient could be told that he should be administered a drug that is not indicated to treat to his cancer,” said Colin Pritchard, MD, PhD, pathologist and Associate Professor of Laboratory Medicine and Pathology at UW Medicine in the new release. (Photo copyright: University of Washington School of Medicine.)
Other detailed findings of the UW Medicine Study:
CHIP variants of 2% or more were detected in cfDNA from 13 of 69 men.
Seven men, or 10%, having advanced prostate cancer “had CHIP variants in DNA repair genes used to determine PARPi candidacy.
CHIP variants rose with age: 0% in those 40 to 50; 12.5% in men 51 to 60; 6.3% in those 61 to 70; 20.8% in men 71 to 80; and 71% in men 81 to 90.
Whole-blood control made it possible to distinguish prostate cancer variants from CHIP interference variants.
“Men with prostate cancer are at high risk of being misdiagnosed as being eligible for PARPi therapy using current cfDNA tests; assays should use a whole-blood control sample to distinguish CHIP variants from prostate cancer,” the researchers wrote in JAMA Oncology.
Liquid Biopsies Are ‘Here to Stay’
Surgical oncologist William Cance, MD, Chief Medical and Scientific Officer, American Cancer Society (ACS) in Atlanta, recognizes the challenge of tumor biology to liquid biopsies.
“Genetic abnormalities are only one piece of the puzzle. We need to look comprehensively at tumors for the best therapy, from their metabolic changes and protein signatures in the blood to the epigenetic modifications that may occur, as cancers take hold,” he told Oncology Times. “It’s not just shed DNA in the blood.”
The UW Medicine study demonstrates the importance of understanding how all elements in liquid biopsies interact to affect clinical laboratory test results.
“I think liquid biopsies are here to stay,” Cance told Oncology Times. “They’re all part of precision medicine, tailored to the individual.”
The antibodies target portions of the SARS-CoV-2 spike protein that resist mutation, potentially leading to better treatments and vaccines
One challenge in the battle against COVID-19 is the emergence of SARS-CoV-2 variants, especially the Delta variant, which may be more resistant to neutralizing antibodies compared with the original coronavirus. But now, scientists led by researchers at the Fred Hutchinson Cancer Research Center (Fred Hutch) in Seattle say they have identified antibodies that could be broadly protective against multiple sarbecoviruses, the subgenus that contains SARS-CoV-2 as well as SARS-CoV-1, the virus responsible for the 2002-2004 severe acute respiratory syndrome (SARS) outbreak.
In “SARS-CoV-2 RBD Antibodies That Maximize Breadth and Resistance to Escape,” the researchers described how they compared 12 antibodies obtained from patients infected with either SARS-CoV-2 or SARS-CoV-1. They pointed to one antibody in particular—S2H97—that could lead to development of new vaccines and therapies against current and future variants. It might even protect against sarbecoviruses that have not yet been identified, they wrote.
Unsaid in the news release about these research findings is the fact that these particular antibodies could eventually become useful biomarkers for clinical laboratory tests designed to help physicians determine which patients have these antibodies—and the protection from infection they represent—and which do not.
So far, however, S2H97 has only been tested in hamsters. But results are promising.
“This antibody, which binds to a previously unknown site on the coronavirus spike protein, appears to neutralize all known sarbecoviruses—the genus of coronaviruses that cause respiratory infections in mammals,” said Jay Nix, PhD, an affiliate in Berkeley Lab’s Biosciences Area and Beamline Director of the Molecular Biology Consortium at Berkeley Lab’s Advanced Light Source (ALS), in a Berkeley Lab news release. “And, due to the unique binding site on mutation-resistant part of the virus, it may well be more difficult for a new strain to escape,” he added.
Scientists have long known that the SARS-CoV-2 virus uses the spike protein to attach to human cells. The federal Centers for Disease Control and Prevention (CDC) notes that the variants have mutations in their spike proteins that make some of them more transmissible.
The Delta variant, the CDC notes, was the predominant variant in the US as of August 28, 2021. It “has been shown to have increased transmissibility, potential reduction in neutralization by some monoclonal antibody treatments, and reduction in neutralization by post-vaccination sera,” the agency states.
The key to S2H97, the researchers wrote, is that it targets a portion of the spike protein that is common among sarbecoviruses, and that is likely to be resistant to mutations.
The researchers used a variety of techniques to analyze how the 12 antibodies bind to the virus. They “compiled a list of thousands of mutations in the binding domains of multiple SARS-CoV-2 variants,” Nature reported. “They also catalogued mutations in the binding domain on dozens of SARS-CoV-2-like coronaviruses that belong to a group called the sarbecoviruses. Finally, they assessed how all these mutations affect the 12 antibodies’ ability to stick to the binding domain.”
William Schaffner, MD (above), Professor of Preventive Medicine in the Department of Health Policy as well as Professor of Medicine in the Division of Infectious Diseases at the Vanderbilt University School of Medicine in Nashville, believes that “people who test positive for SARS-CoV-2 and who are at risk of progressing to severe disease—including those who are over the age of 65 years and those who have weakened immune systems—should talk with a doctor about receiving monoclonal antibody treatment,” Medical News Today reported. “[The monoclonal antibody treatment is] designed to prevent the evolution of the infection from a mild infection into a serious one,” he noted. “In other words, you’ve just [contracted the virus], but we can now give you a medication that will help prevent [you] being hospitalized and getting seriously ill.” (Photo copyright: Vanderbilt University.)
Earlier Antibody Treatment Receives an EUA from the FDA
In issuing the EUA for sotrovimab, the FDA cited “an interim analysis from a phase 1/2/3 randomized, double-blind, placebo-controlled clinical trial in 583 non-hospitalized adults with mild-to-moderate COVID-19 symptoms and a positive SARS-CoV-2 test result. Of these patients, 291 received sotrovimab and 292 received a placebo within five days of onset of COVID-19 symptoms.”
Among these patients, 21 in the placebo group were hospitalized or died compared with three who received the therapy, an 85% reduction.
“While preventive measures, including vaccines, can reduce the total number of cases, sotrovimab is an important treatment option for those who become ill with COVID-19 and are at high risk—allowing them to avoid hospitalization or worse,” stated Adrienne E. Shapiro, MD, PhD, of the Fred Hutchinson Cancer Research Center in a GSK news release. Shapiro was an investigator in the clinical trial.
The EUA allows use of sotrovimab in patients who have tested positive for SARS-CoV-2, have mild-to-moderate symptoms, and “who are at high risk for progression to severe COVID-19, including hospitalization or death. This includes, for example, individuals who are 65 years of age and older or individuals who have certain medical conditions.” It is not authorized for patients who are hospitalized or for those who require oxygen therapy.
The therapy was originally known as VIR-7831. The companies say they have developed a similar treatment, VIR-7832, with modifications designed to enhance T cell function against the disease.
The antibody, they wrote, targets a region of the SARS-CoV-1 spike protein that is “highly conserved” among sarbecoviruses. Clinical laboratory testing, they wrote, also indicated that the therapy was likely to be effective against known SARS-CoV-2 variants.
“Our distinctive scientific approach has led to a single monoclonal antibody that, based on an interim analysis, resulted in an 85% reduction in all-cause hospitalizations or death, and has demonstrated, in vitro, that it retains activity against all known variants of concern, including the emerging variant from India,” stated Vir Biotechnology CEO George Scangos, PhD, in the GSK news release. “I believe that sotrovimab is a critical new treatment option in the fight against the current pandemic and potentially for future coronavirus outbreaks, as well.”
Pathologists and clinical laboratory managers working with rapid molecular tests and antibody tests for COVID-19 will want to monitor the development of monoclonal antibody treatments, as well as further research studies that focus on these specific antibodies.
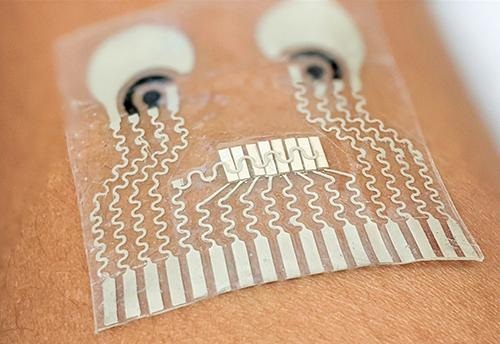
Skin patch technologies could enable clinical laboratories to monitor patients’ vitals and report to medical professionals in real time
Pathologists and clinical laboratory leaders have read many Dark Daily ebriefings on the development of skin patches over the years that do everything from monitoring fatigue in the military to being a complete lab-on-skin technology. Now, researchers at the University of California San Diego (UCSD) have developed a wearable patch that can monitor cardiovascular signals and other various biochemical levels in the body simultaneously.
The researchers believe there is enormous potential for such a patch in helping patients monitor conditions such as hypertension or diabetes. They also foresee a scenario where the patch could be used in settings where vitals must be constantly monitored. They hope to develop future versions of the patch that can detect more biomarkers within the body.
“This type of wearable would be very helpful for people with underlying medical conditions to monitor their own health on a regular basis,” Lu Yin, a PhD student and co-first author of the study, told New Atlas. “It would also serve as a great tool for remote patient monitoring, especially during the COVID-19 pandemic when people are minimizing in-person visits to the clinic,” she added.
Combining Precision Medicine with Telehealth and the Internet of Things
About the size of a postage stamp and consisting of stretchy polymers that conform to the skin, the UCSD patch monitors blood pressure and contains sensors that measure different biochemical levels in the body, such as:
The sensors are carefully arranged on the patch to eliminate interference between the signals, noted a UCSD press release.
In their published research, the UCSD researchers wrote of their new skin patch monitoring device, “Intertwined with concepts of telehealth, the internet of medical things, and precision medicine, wearable sensors offer features to actively and remotely monitor physiological parameters. Wearable sensors can generate data continuously without causing any discomfort or interruptions to daily activity, thus enhancing the self-monitoring compliance of the wearer, and improving the quality of patient care.” (Photo copyright: University of California San Diego.)
“Each sensor provides a separate picture of a physical or chemical change. Integrating them all in one wearable patch allows us to stitch those different pictures together to get a more comprehensive overview of what’s going on in our bodies,” said Sheng Xu, PhD, Principle Investigator, Xu Research Group at UCSD, Assistant Professor in the Department of NanoEngineering Department, and a co-first author of the study, in the press release.
The UCSD researchers developed their skin patch to monitor specific biomarkers that can affect blood pressure.
“Let’s say you are monitoring your blood pressure and you see spikes during the day and think that something is wrong,” co-first author Juliane Sempionatto, PhD, a postdoctoral researcher at California Institute of Technology (Caltech) and co-first author of the study, told New Atlas. “But a biomarker reading could tell you if those spikes were due to an intake of alcohol or caffeine. This combination of sensors can give you that type of information,” she added.
The blood pressure sensor sits near the center of the patch and consists of a set of small transducers welded to the patch via a conductive link. Voltage applied to the transducers send ultrasound waves through the body which bounce off arteries and create echoes that are detected by the sensor and converted into an accurate blood pressure reading.
The chemical sensor releases the drug pilocarpine into the skin to induce sweat and then measures the chemicals contained in the sweat to provide readings of certain biochemical levels.
The glucose sensor located in the patch emits a mild electrical current to the body that stimulates the release of interstitial fluid and then reads the glucose level in that fluid.
“The novelty here is that we take completely different sensors and merge them together on a single small platform as small as a stamp,” Joseph Wang, D.Sc, SAIC Endowed Chair, Distinguished Professor of NanoEngineering, Director of the Center for Wearable Sensors at UCSD, and co-author of the study told New Atlas. “We can collect so much information with this one wearable and do so in a non-invasive way, without causing discomfort or interruptions to daily activity.” (Photo copyright: University of Southern California San Diego.)
Skin Patch Measurements Closely Match Those of Traditional Devices
Test subjects wore the patch on their neck while performing various combinations of the following tasks:
exercising on a stationary bicycle,
eating a high-sugar meal,
drinking an alcoholic beverage, and
drinking a caffeinated beverage.
The results of the measurements taken from the patch closely matched measurements collected by traditional monitoring devices such as a:
For now, the patch must be connected to an external power source which transmits the reading to a counter-top machine, but the researchers hope to create a wireless version in the future.
“There are opportunities to monitor other biomarkers associated with various diseases,” Sempionatto said in the UCSD press release. “We are looking to add more clinical value to this device.”
Other Similar Skin Patch Monitoring Technologies
Though an important breakthrough, the UCSD’s device is not the first skin patch monitor to be developed.
Multiple research and clinical studies are underway that hope to prove the accuracy and safety of wearable devices at detecting and monitoring certain health conditions. It’s a worthy goal.
Skin patches, such as the one created at UCSD, could enable clinical laboratories to provide value-added service to medical professionals and patients alike. Medical labs could potentially monitor skin patch readings in real-time and notify physicians and patients of changes in biomarkers that require attention.
Further, as this technology is developed, it will likely find a ready market with the latest generation of consumers who are more willing than previous generations to buy their own diagnostic tests for home use. These “next-generation” healthcare consumers have demonstrated their willingness to use Apple watches, Fitbits, and similar wearable devices to monitor their condition during exercise and other health metrics.
Pathologists and clinical laboratory managers should not overlook the potential for robust consumer demand to accelerate development and market adoption of such skin patches.