New biomarkers for cancer therapies derived from the research could usher in superior clinical laboratory diagnostics that identify a patient’s suitability for personalized drug therapies and treatments
Once approved for clinical use, not only would these biomarkers become targets for specific cancer therapies, they also would require development of new diagnostic tests that anatomic pathologists could use to determine whether a biomarker was present in a patient.
If yes, the drug can be administered. If no, the patient is not a candidate for that drug. Thus, this research may produce both diagnostic biomarkers and therapeutic targets.
Relevance of In-Depth Tumor Profiling to Support Clinical Decision-Making
In the Swiss “Tumor Profiler” (TuPro) project, the research team is examining the cellular composition and biology of tumors of 240 patients with melanoma, ovarian cancer, and acute myeloid leukemia. Recruitment for the study began in 2018. Today, the melanoma cohort is fully enrolled, and the ovarian cancer and acute myeloid leukemia cohorts are nearing complete enrollment.
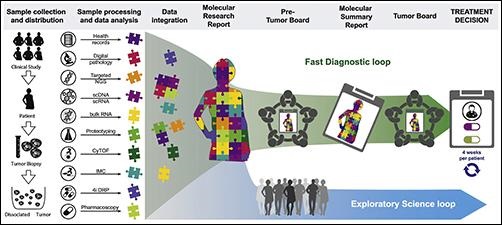
“The Tumor Profiler Study is an observational clinical study combining a prospective diagnostic approach to assess the relevance of in-depth tumor profiling to support clinical decision-making (“fast diagnostic loop”) with an exploratory approach to improve the biological understanding of disease (“exploratory science loop”),” the TuPro website states.
The graphic above taken from the Tumor Profiler project paper illustrates how the TuPro study’s workflow entails patient enrollment, sample collection, analysis by different technology platforms, and data integration, creation and discussion of molecular research and summary reports, discussion of treatment options in pre-tumor boards and the final treatment decision in tumor boards. (Photo copyright: Cancer Cell.)
In their published paper, the Swiss researchers say these three cancers were selected for the study “based on the potential clinical benefit and availability of sufficient tumor material for simultaneous analysis across all technologies.”
According to a University Hospital Basel blog post, the TuPro project examination of each cancer tumor goes “much further than the limited use of molecular biological methods” used by leading hospitals. “This results in huge amounts of data per patient, which we process and analyze using data science methods,” stated data scientist Gunnar Rätsch, PhD (above), Professor for BiomedicalInformatics at ETH Zurich and one of the study’s corresponding authors, in the blog post. This research could lead to new precision medicine biomarkers for clinical laboratory cancer diagnostics and therapies. (Photo copyright: ETH Zurich.)
The TuPro Project’s findings are available to doctors who analyze them at interdisciplinary tumor board meetings and generate treatment options, creating a “fast diagnostic loop” with an estimated four-week turnaround time from surgery to tumor board. “This approach has the potential to alter current diagnostics and paves the way for the translation of comprehensive molecular profiling into clinical decision-making,” the study’s authors wrote in Cancer Cell.
Could Oncologists Be Making Better Precision Medicine Decisions?
In its writeup on the TuPro Project’s research, Precision Oncology News concluded that the Swiss study “is rooted in the researchers’ notion that oncologists are not making the best personalized treatment decisions for patients by relying just on targeted DNA profiling using next-generation sequencing and digital pathology-based tests.
“The researchers within the TuPro consortium hypothesized that integrating a more comprehensive suite of omics tests could lead to a more complete understanding of patients’ tumors, including providing insights into the tumor microenvironment, heterogeneity, and ex vivo responses to certain drugs. This, in turn, could help inform the best course of treatment,” Precision Oncology News added.
“With the Tumor Profiler study, we want to show that the widespread use of molecular biological methods in cancer medicine is not only feasible, but also has specific clinical benefits,” said TuPro consortium member Viola Heinzelmann-Schwarz, MD, Head of Gynecological Oncology at University Hospital Basel, in an ET Zurich news release.
New Precision Medicine Biomarkers from TuPro’s Molecular Analysis
Researchers in the study also are investigating whether and what influence the molecular analysis had on doctors’ therapy decisions.
The University Hospital Basal blog notes the long-term benefits of the Tumor Profiler approach is to expand the personalized-medicine therapy options for patients, including determining whether patients would benefit in certain cases “if they were not treated with drugs from standard therapy, but with drugs that have been approved for other types of cancer.”
Anatomic pathologists and clinical laboratory scientists will want to take note of the TuPro project’s ultimate success or failure, since it could usher in changes in cancer treatments and bring about the need for new diagnostic tests for cancer biomarkers.
As many clinical laboratory scientists know, gene sequencing technology continues to become faster, more accurate, and less expensive per whole human genome sequenced
In February, Dark Daily reported that Personalis, Inc. (NASDAQ:PSNL) had delivered its 100,000th whole human genome sequence to the US Department of Veterans Affairs Million Veterans Program (VA MVP). Now, the Menlo Park, Calif.-based cancer genomics company has topped that achievement by delivering its 125,000 whole human genome sequence!
“This represents another important landmark for both the program and for Personalis,” said John West, Chief Executive Officer, Personalis, in a news release. “We congratulate the VA MVP for reaching this important milestone.
“We strongly believe that the research projects being performed today will enable precision medicine in healthcare systems in the future across a wide range of disease areas,” he added. This is a positive development for clinical laboratories, as personalized medicine services require a lab to sequence and interpret the patient’s DNA.
Personalis was contracted with the US federal government to perform genetic research in 2012 and has delivered 50,000 genomes to the VA MVP during the past twelve months.
The Personalis and VA MVP researchers seek to gain a better understanding of how genetic variants affect health. Before the COVID-19 pandemic hit the US, the VA was enrolling veterans in the Million Veterans Program at 63 VA medical centers across the country. There are currently about 830,000 veterans enrolled in the venture and the VA is expecting two million veterans to eventually sign up for the sequencing project.
“As a global leader in genomic sequencing and comprehensive analytics services, Personalis is uniquely suited to lead these population-scale efforts and we are currently in the process of expanding our business operations internationally,” West added.
According to the press release, “the VA MVP provides researchers with a rich resource of genetic, health, lifestyle, and military-exposure data collected from questionnaires, medical records, and genetic analyses. By combining this information into a single database, the VA MVP promises to advance knowledge about the complex links between genes and health.”
NIH All of Us Research Program Supports Precision Medicine Goals Another genetic research project being conducted by the US National Institutes of Health (NIH) is the All of Us Research Program. Using donated personal health information from thousands of participants, the NIH researchers seek to “learn how our biology, lifestyle, and environment affect health,” according to the program’s website.
“We’re changing the paradigm for research,” said Josh Denny, MD (above), Chief Executive Officer of the All of Us Research Program, in an NIH news release. “Participants are our most important partners in this effort, and we know many of them are eager to get their genetic results and learn about the science they’re making possible. We’re working to provide that valuable information in a responsible way,” he added. Clinical laboratories may soon see new precision medicine biomarkers derived from this type of research. (Photo copyright: Vanderbilt University.)
The All of Us Research Program intends to have at least one million US participants take part in the research. The researchers hope to help scientists discover new knowledge regarding how biological, environmental, and behavioral factors influence health, and to learn to tailor healthcare to patients’ specific medical needs, a key component of precision medicine.
Participants in the project share personal information via a variety of methods, including surveys, electronic health records, and biological samples.
A Better Sampling of Under-Represented Communities
Since opening enrollment in 2018, more than 270,000 people have contributed blood, urine, and saliva samples to the All of Us Research Program. More than 80% of the participants come from communities that are traditionally under-represented in biomedical research.
“We need programs like All of Us to build diverse datasets so that research findings ultimately benefit everyone,” said Brad Ozenberger, PhD, Genomics Program Director, All of Us, in the NIH news release. “Too many groups have been left out of research in the past, so much of what we know about genomics is based mainly on people of European ancestry. And often, genomic data are explored without critical context like environment, economics, and other social determinants of health. We’re trying to help change that, enabling the entire research community to help fill in these knowledge gaps.”
The All of Us Research Project’s analysis of the collected data includes both whole-genome sequencing (WGS) and genotyping and is taking a phased approach in returning genetic data to participants.
Participants initially receive data about their genetic ancestry and traits. That is followed later by health-related results, such as how their genetic variants may increase the risk of certain diseases and how their DNA may affect their reaction to drug therapies.
Genetic researchers hope programs like these will lead to improved in vitro diagnostics and drug therapies. Genetic sequencing also may lead to new diagnostic and therapeutic biomarkers for clinical laboratories.
Since all Americans have access to free COVID-19 vaccines, many pathologists and clinical lab managers will ask if this test is even necessary. Some experts say “maybe”
Here’s another example of genetic test developers who are willing to push boundaries and sell a diagnostic test directly to consumers that has some diagnostic experts and pathologists challenging its clinical validity.
The test was developed by molecular diagnostics company Genetic Technologies Ltd. (NASDAQ:GENE) of Melbourne, Australia, and, according to an article in Science, is an at-home saliva test that “combines genetic data with someone’s age, sex, and pre-existing medical conditions to predict their risk of becoming extremely ill from COVID-19.”
In a non-peer-reviewed preprint, titled, “Development and Validation of a Clinical and Genetic Model for Predicting Risk of Severe COVID-19,” Genetic Technologies’ Chief Scientific Officer Richard Allman, PhD, and Senior Biostatistician and the study’s first author, Gillian Dite, PhD, wrote, “Using SARS-CoV-2 positive participants from the UK Biobank, we developed and validated a clinical and genetic model to predict risk of severe COVID-19. … Accurate prediction of individual risk is possible and will be important in regions where vaccines are not widely available or where people refuse or are disqualified from vaccination, especially given uncertainty about the extent of infection transmission among vaccinated people and the emergence of SARS-CoV-2 variants of concern.”
But since every American already has access to free COVID-19 vaccines, one wonders why this test would be launched in the US?
Determining Risk for COVID-19 Infection
Can a genetic test predict an individual’s risk of contracting a SARS-CoV-2 infection that would require hospitalization or cause death? Genetic Technologies and its US partner, Infinity BiologiX (IBX) of Piscataway, N.J., believe so.
According to a Genetic Technologies news release, the saliva test, which reportedly costs $175, enables a “leading-edge risk assessment that estimates your personal risk of severe disease,” IBX says on its website.
The at-home saliva-based test, which is intended for people age 18 and older, gives a risk score for contracting a serious COVID-19 case based on genetic and clinical information, IBX stated in its own news release.
The two companies partnered with Vault Health, a “virtual platform for telemedicine and diagnostics” developer, to distribute, and sell the COVID-19 Serious Disease Risk Test in the US.
In the IBX news release, IBX’s Chief Executive Officer, Robin Grimwood, said, “We see this initial agreement for the sale and distribution of Genetic Technologies’ COVID-19 Risk Test (above) as a critical collaboration in line with our mission to understand the genetic causes of common, complex diseases and to discover diagnoses, treatments and, eventually, cures for these diseases.” However, as Dark Daily’s sister publication The Dark Report previously reported, some geneticists, epidemiologists, and clinical laboratory professionals have expressed concerns. (Photo copyright: Infinity BiologiX.)
Is There a Place for Genetic COVID-19 Risk Test in the US?
“Alongside existing treatment options and vaccines, we believe this test will enable more insightful decisions for states, workplaces, and individuals,” said Simon Morriss, Genetic Technologies’ CEO, in the news release.
Meanwhile, some experts are uncertain about predictive types of testing for the SARS-CoV-2 coronavirus. “I think it’s premature to use a genetic test to predict a person’s likely COVID-19 severity. We don’t understand exactly what these genetic variants mean or how they affect disease,” epidemiologist Priya Duggal PhD, a professor in the Genetics Epidemiology Division at the Johns Hopkins University School of Public Health, told Science.
According to Science, “The test debuts in a regulatory gray zone …. The two companies did not seek [FDA] approval for validity because, [Genetic Technologies Chief Scientific Officer Richard Allman] says, the test is not a direct-to-consumer product that falls under its review. After a customer receives results from IBX’s federally-approved labs, they can consult with a ‘telehealth’ physician.”
“We are uniquely and strategically positioned with our partners to deliver the test and provide remote telehealth services and reporting, utilizing our extensive array capability and capacity across a number of platforms,” Grimwood said in the IBX news release.
However, Science reported that “Several geneticists who reviewed the company’s preprint” said “the test needs to be validated in other, more diverse populations than one detailed in the UK Biobank, and they wonder whether its predictions are reliable for people infected with new SARS-CoV-2 variants.”
“It’s a good start, but by no means is it calibrated or validated sufficiently to say this is a test I would take, or my wife should take,” cancer geneticist Stephen Chanock, MD, Director of the Division of Cancer Epidemiology and Genetics at the National Cancer Institute, National Institutes of Health, told Science.
The question remains unanswered as to why a genetic risk test for SARS-CoV-2 and its variants is needed in the United States. Nevertheless, clinical laboratory leaders and pathologists may want to monitor these developments for new biomarkers and COVID-19 diagnostics.
Following a nearly two-year disruption due to the SARS-CoV-2 pandemic, pathologists and clinical laboratory professionals once again have an opportunity to gather and learn from each other
It is good news that the daily number of new cases of COVID-19 continue declining here in the United States. That fact, and the growing number of vaccinations, have encouraged state and federal officials to lift many restrictions on business and social activities.
Clinical laboratories are watching a big drop in the daily number of COVID-19 tests they perform, even as routine test volumes climb and more patients show up in doctors’ offices for the typical mix of ailments and health conditions.
It’s true that many familiar routines are back. But it is also true that things are not exactly the way they were pre-pandemic. And that’s the rub. Going forward, what should medical laboratory managers and pathologists expect to be the “post-pandemic normal” in how patients access care and how providers deliver clinical services? How will healthcare in this country be different from what it was pre-pandemic?
Preparing Clinical Lab Leaders for What Comes Next
These questions and more will be front and center when the Executive War College on Lab and Pathology Management returns on Nov. 2-3, 2021, at the Hyatt Riverwalk Hotel in San Antonio. The theme of this first live gathering since the spring of 2019 will be “Preparing Your Clinical Laboratory and Pathology Group for Post-Pandemic Success.”
“Today, lab managers have the interesting challenge of understanding the new opportunities they can use to advance their labs, both clinically and financially,” stated Robert L. Michel, Editor-in-Chief of Dark Daily and its sister publication The Dark Report, and founder of the Executive War College. “It isn’t that the pandemic changed healthcare in fundamental ways. Rather, it is that the pandemic accelerated changes that were underway before the outbreak began.
“That’s true of telehealth as well, for example,” he continued. “Once the nation was locked down, utilization of virtual physician visits and telehealth services skyrocketed. Today, national surveys confirm that as many as 50% of all patients and physicians have used a telehealth service, are comfortable with this type of appointment, and are ready to continue to use virtual office visits.
Robert Michel (above), Editor-in-Chief of Dark Daily, its sister publication The Dark Report, and founder of The Dark Intelligence Group, will host the first live edition of the Executive War College since May 2019 in San Antonio. The theme will be “Preparing Your Clinical Laboratory and Pathology Group for Post-Pandemic Success.” Attendees from clinical laboratories and pathology groups will gain critical insights they can act on immediately. (Photo copyright: The Dark Report.)
“Another trend accelerated by the pandemic is patient self-testing at home,” Michel added. “Government health officials saw the benefit of clearing for clinical use different specimen collection systems and COVID-19 test methods designed for use by consumers in the comfort of their home. Today, consumers can choose from multiple specimen collection products and SARS-CoV-2 tests designed for in-home use. Clinical laboratory managers should consider this development to be a consumer home-test baseline. Federal officials have created a regulatory pathway that will make it easier and faster for federal regulators to clear other types of diagnostic tests for consumer home use.”
What if the FDA Approves More Consumer At-Home Tests?
There are implications to each of the two trends described above. In the case of telehealth, if patients see their doctors virtually and the doctors order medical tests, how do clinical laboratories access these patients to collect the specimens needed to do this testing?
Similarly, if, in coming years, the federal Food and Drug Administration (FDA) increases the number of diagnostic test specimen-collection kits that consumers can use from home, how should local clinical laboratories position themselves to receive those kits and perform those tests?
These are two examples of important questions to be answered at sessions scheduled for the Executive War College in San Antonio on Nov. 2-3. Case studies by innovative lab leaders will address topics ranging from high-level strategy to daily management, operations, marketing, and managed care contracting.
Attendance Limited at This Fall’s Executive War College
At the first live edition of the Executive War College since May 2019, attendees will notice one significant difference from earlier years. By design, and for the safety and well-being of attendees, the number of attendees will be limited to 300. The hotel follows the Centers for Disease Control and Prevention (CDC) guidelines and is prepared to adjust those numbers as CDC guidance evolves. Thus, those interested in attending this year’s conference are advised to register early to guarantee their place and avoid being disappointed.
Suggestions for session topics and speakers are welcome and can be sent to info@darkreport.com. Conference details, session topics, and speakers will be updated regularly at www.executivewarcollege.com.
So, register today because seating is limited at the 2021 Executive War College Presents “Preparing Your Clinical Laboratory and Pathology Group for Post-Pandemic Success.” To ensure your place at this valuable conference, click HERE or place this URL (https://dark.regfox.com/2021-ewc-presents) into your browser.
The study ‘shows that measurement using a urine test provides improved accuracy relative to other measurement methods, for example certain kinds of blood tests,’ a KI news release states
Researchers at the Karolinska Institute (KI) in Sweden have developed a non-invasive urine-based test that can identify what type of asthma a patient has and its severity. If developed into a clinical laboratory diagnostic, such a test also could give clinicians a better idea of what treatment is more likely to be effective—a core goal of precision medicine.
Another benefit of this methodology is that it is a non-invasive test. Should further studies conclude that this urine-based test produces accurate results acceptable for clinical settings, medical laboratories would certainly be interested in offering this assay, particularly for use in pediatric patients who are uncomfortable with the venipunctures needed to collect blood specimens. Also, given the incidence of asthma in the United States, there is the potential for a urine-based asthma test to generate a substantial number of test requests.
The objective of the study, according to the Karolinska Institute researchers, was “To test if urinary eicosanoid metabolites can direct asthma phenotyping.” The team used mass spectrometry to measured certain lipid biomarkers (prostaglandins and leukotrienes), which are known to play a key role in the inflammation that occurs during asthma attacks.
According to a KI news release, “The study is based on data from the U-BIOPRED study (Unbiased BIOmarkers in PREDiction of respiratory disease outcomes), which was designed to investigate severe asthma. The study included 400 participants with severe asthma, which often requires treatment with corticosteroid tablets, nearly 100 individuals with milder forms of asthma, and 100 healthy control participants.”
“We discovered particularly high levels of the metabolites of the mast cell mediator prostaglandin D2 and the eosinophil product leukotriene C4 in asthma patients with what is referred to as Type 2 inflammation. Using our methodology, we were able to measure these metabolites with high accuracy and link their levels to the severity and type of asthma,” said Johan Kolmert, PhD (above), a post-doctoral researcher at the Institute of Environmental Medicine, Karolina Institute, and first author of the study, in the KI news release. If perfected, such accuracy could lead to effective precision medicine clinical laboratory tests. (Photo copyright: Karolinska Institute.)
More Accurate Testing Could Lead to Biomarker-guided Precision Medicine
In the US alone, 25,131,132 people currently suffer from asthma, about five million of which are children under the age of 18, according to 2019 CDC statistics. The World Health Organization (WHO) reports that worldwide, “Asthma affected an estimated 262 million people in 2019 and caused 461,000 deaths.”
People with mild asthma may have good success using steroid inhalers. However, for those with moderate to severe asthma where inhalers are not effective, oral corticosteroids may also be necessary. But corticosteroids have been associated with high blood pressure and diabetes, among other negative side effects.
“To replace corticosteroid tablets, in recent times several biological medicines have been introduced to treat patients with Type 2 inflammation characterized by increased activation of mast cells and eosinophils,” said Sven-Erik Dahlén, Professor at the Institute of Environmental Medicine, Karolinska Institute, in the news release.
Currently, there are no simple tests that show what type of asthma a patient has. Instead, clinicians rely on lung function tests, patient interviews, allergy tests, and blood tests.
Earlier this year, researchers at Brigham and Women’s Hospital and Exosome Diagnostics in Massachusetts investigated a non-invasive, urine-based test for transplant rejection. According to a news release, “Patients can spend up to six years waiting for a kidney transplant. Even when they do receive a transplant, up to 20% of patients will experience rejection.”
“If rejection is not treated, it can lead to scarring and complete kidney failure. Because of these problems, recipients can face life-long challenges,” said Jamil Azzi, MD, Director of the Kidney Transplantation Fellowship Program at Brigham and Women’s Hospital, and Associate Professor of Medicine at Harvard School of Medicine. “Our goal is to develop better tools to monitor patients without performing unnecessary biopsies. We try to detect rejection early, so we can treat it before scarring develops,” he said.
Detecting Bladder Cancer with Urine Testing
Another condition where urine tests are being investigated is bladder cancer. An article in Trends in Urology and Men’s Health states, “Several point-of-care urine tests have been developed to help identify patients who may be at higher risk of bladder cancer.” Those tests could have the potential for use in primary care, which could mean fewer people would need invasive, painful, and risk-carrying cystoscopies.
“New tests to help identify hematuria patients who are at a higher risk of cancer would help to improve the diagnostic pathway, reduce the number diagnosed by emergency presentation, lessen the burden on urology services, and spare those who do not have cancer an invasive and costly examination, such as cystoscopy,” the article’s authors wrote.
These urine-based tests are still under investigation by various research teams and more research is needed before clinical trials can be conducted and the tests can be submitted for regulatory approval. Though still in the early stages of development, urine-based diagnostic testing represents far less invasive, and therefore safer, ways to identify and treat various diseases.
Studies into how the elements in urine might be used as biomarkers for clinical laboratory tests may lead to improved non-invasive precision medicine diagnostics that could save many lives.
The rapid diagnostic test costs less than $5 per unit and can be adapted for other diseases, the developers say, which opens a slew of possibilities for clinical laboratories
Just as the SARS-CoV-2 coronavirus spurred deployment of new vaccine technology based on messenger RNA (mRNA), the COVID-19 pandemic also could prove to be a watershed for in vitro diagnostics (IVD) innovation in ways that benefit clinical laboratories.
A Penn Medicine news release noted that “The RAPID technology … transforms the binding event between the SARS-CoV-2 viral spike protein and its receptor in the human body, the protein ACE2 (which provides the entry point for the coronavirus to hook into and infect human cells), into an electrical signal that clinicians and technicians can detect. That signal allows the test to discriminate between infected and healthy human samples. The signal can be read through a desktop instrument or a smartphone.”
Though still in its early stages, the technique potentially offers dramatically lower costs and faster results than traditional RT-PCR (reverse transcription polymerase chain reaction) molecular tests. Moreover, the RAPID technology might be useful for identifying other types of biomarkers and could be the basis for diagnostic tests that help reduce the cost-per-test in medical laboratory testing while providing comparable sensitivity and specificity to existing methodologies.
Clinical trials began on January 5, 2021, and the Penn Medicine researchers say the IVD test technology can be applied to other infectious diseases, which, if proven accurate, would be a boon to clinical laboratory testing.
Diagnostic Test Results in Four Minutes for Less than $5/Test
According to the news release, the RAPID 1.0 (Real-time Accurate Portable Impedimetric Detection prototype 1.0) biosensor test costs less than $5 and can deliver results in four minutes. The researchers reported overall accuracy of 87.1% on (139) nasal swab samples and 90% on (50) saliva samples.
The technology uses electrodes that can be mass-produced at low cost on commercially-available screen printers, the researchers said. Results can be read on electronic devices connected to a PC or smartphone.
RAPID 1.0 (above) is a low-cost COVID-19 diagnostic test developed at the César de la Fuente clinical laboratory at the Perelman School of Medicine University of Pennsylvania in Philadelphia. At less than $5/test, plus the ability to be adapted to other diseases, clinical laboratories performing disease screenings in rural or remote locations may have a new tool in the fight against infections. (Photo copyright: University of Pennsylvania.)
Does Penn Medicine’s RAPID 1.0 Test Replace Traditional RT-PCR Testing?
In their published study, the Penn Medicine researchers cited the need for “fast, reliable, inexpensive, and scalable point-of-care diagnostics.”
RT-PCR tests, they said, “are limited by their requirement of a large laboratory space, high reagent costs, multistep sample preparation, and the potential for cross-contamination. Moreover, results usually take hours to days to become available.”
Researchers who have studied the SARS-CoV-2 coronavirus know that it uses a spike-like protein to bind to angiotensin-converting enzyme 2 (ACE2) receptors on the surfaces of human cells.
As described in Penn Medicine’s published study, the biosensor contains ACE2 and other biochemical agents anchored to an electrode. When the SARS-CoV-2 coronavirus attaches to the ACE2, the biosensor transforms the chemical reaction into an electrical signal that can be measured on a device known as a potentiostat.
The researchers tested their RAPID 1.0 technology with two commercially available potentiostat models:
The researchers initially developed the electrode as a printed circuit board, which is relatively expensive. To reduce costs, they constructed a version that uses filter paper as the main component. The researchers noted that one screen printer in a lab can produce 35,000 electrodes per day, including time needed to incorporate the chemical elements. “However, it must be noted that these steps can be fully automated into a production line for industrial purposes, drastically reducing time requirements,” they wrote.
The test can be performed at room temperature, they added, and total cost per unit is $4.67. Much of that—$4.50—is for functionalizing the ACE2 recognition agent. The cost for the bare electrode is just seven cents.
“The overall cost of RAPID may be further reduced through recombinant production of ACE2 and ACE2 variants,” the researchers said, adding that the RAPID 1.0 test can detect the SARS-CoV-2 coronavirus at low concentrations correlating to the earliest stages of the COVID-19 disease.
The Penn Medicine research team was led by César de la Fuente, PhD (above), an Assistant Professor in Psychiatry, Microbiology, Chemical and Biomolecular Engineering and Bioengineering at the Perelman School of Medicine. “Prior to the pandemic, our lab was working on diagnostics for bacterial infections,” he said in the Penn Medicine news release. “But then, COVID-19 hit. We felt a responsibility to use our expertise to help—and the diagnostic space was ripe for improvements.” (Photo copyright: University of Pennsylvania.)
Testing Penn Medicine’s RAPID 1.0 Test
The researchers evaluated the technology in blinded tests with clinical samples from the Hospital of the University of Pennsylvania. The evaluation included 139 nasal swab samples, of which 109 were determined to be COVID-19 positive by RT-PCR tests and clinical assessments. Among these, the RAPID test successfully detected the SARS-CoV-2 coronavirus in 91 samples, for a sensitivity rate of 83.5%. One sample was from a patient diagnosed with the highly contagious SARS-CoV-2 Alpha variant B.1.1.7, which the test correctly identified as positive.
Among the 30 samples determined to be COVID negative, the RAPID test scored a specificity rate of 100%, meaning no false positives. Overall accuracy, including sensitivity and specificity, was 87.1%.
The researchers also analyzed 50 saliva samples: 13 COVID-positive and 37 COVID-negative. The test correctly identified all 13 positive samples but produced five false-positives among the 37 negative samples, for a specificity rate of 86.5%. The researchers speculated that this could be due to interactions between ACE2 and other biomolecules in the saliva but suggested that performance “will improve when using fresh saliva samples at the point-of-care.”
Are There Other Applications for the RAPID Test?
The Penn Medicine news release said the RAPID technology can be adapted to detect other viruses, including those that cause Influenza and sexually-transmitted diseases.
Robert Michel, Editor-in-Chief of Dark Daily and its sister publication The Dark Report, said the test points to one silver lining in the COVID-19 pandemic. “Researchers around the world intensified their work to find ways to identify the SARS-CoV-2 virus that are faster, cheaper, and more accurate than the diagnostic technologies that existed at the time of the outbreak. In this regard, the COVID-19 pandemic may have accelerated the development and refinement of useful diagnostic technologies that will disrupt long-established methods of testing.”
Marcelo Der Torossian Torres, PhD, postdoctoral researcher at Penn Medicine and lead author of the study, said in the news release, “Quick and reliable tests like RAPID allow for high-frequency testing, which can help identify asymptomatic individuals who, once they learn they are infected, will stay home and decrease spread.
“We envision this type of test being able to be used at high-populated locations such as schools, airports, stadiums, companies—or even in one’s own home,” he added.
Clinical laboratory managers may want to stay current on the development and possible commercialization of the RAPID 1.0 (Real-time Accurate Portable Impedimetric Detection prototype 1.0) biosensor test by the research team at Penn Medicine.