Advancements in genetic sequencing continue to enable microbiologists and genetic scientists to explore the origins and mutations of deadly diseases
Microbiologists and researchers can now study the gene sequence of 5,000-year-old bubonic plague bacteria. The scientific team that achieved this feat of gene sequencing believes this is the oldest case of the ancient strain of the plague found to date.
For microbiologists, this demonstrates how advances in gene sequencing technologies are allowing scientists to go further back in time to look at how the genomes of bacteria and viruses have evolved and mutated. This helps science understand the process of genetic mutation, as well as learning which mutations survived because they could more easily infect humans.
Missing Gene has ‘Dramatic Influence on Virulence’ of Plague
To conduct their study, the researchers sequenced the genomes of samples from the teeth and bones of four hunter-gatherers and tested the remains for bacterial and viral pathogens. They found evidence of Yersinia pestis (Y. pestis) in the dental remains of a 20- to 30-year-old male dubbed RV 2039.
The jaw bones used for the research were discovered in the late 1800s in the Rinnukalns, a stone age settlement unearthed in present-day Republic of Latvia in the late 19th century.
Missing Genetic Element in Ancient Bacterium
The scientists were surprised to find evidence of Y. pestis in the remains and noted that the analysis of the microbe lacked a crucial genetic element observed in later strains of the bacteria. Missing was the gene that allows biting fleas to act as vectors to spread the plague to humans.
“What’s so surprising is that we see already in this early strain more or less the complete genetic set of Y. pestis, and only a few genes are lacking,” said biochemist and archeologist Ben Krause-Kyora, Professor and head of the Ancient DNA (aDNA) Laboratory at the University of Kiel in Germany, and one of the authors of the study, in a press release.
“But even a small shift in genetic settings can have a dramatic influence on virulence,” he added.
This absent gene also is responsible for creating the pus-filled buboes associated with the Black Death (bubonic plague) that occurred in the 1300s. The Black Death killed 75 million to 200 million people worldwide, mostly in Eurasia and North Africa. It is to date the most fatal pandemic recorded in human history.
“Different pathogens and the human genome have always evolved together,” said Professor Ben Krause-Kyora (above left with and Steve Zäuner at center and Dr. Silvia Codreanu-Windauer at right), in the press release. “We know Y. pestis most likely killed half of the European population in a short time frame, so it should have a big impact on the human genome. But even before that, we see major turnover in our immune genes at the end of the Neolithic Age, and it could be that we were seeing a significant change in the pathogen landscape at that time as well,” he added. (Photo copyright: Mittelbayerische.)
A Less Lethal Bubonic Plague?
Although RV 2039 most likely perished from the bubonic plague, the researchers believe his strain of the infection was more mild, less contagious, and not as lethal as the later genetic mutations of the bacteria that caused the Black Death pandemic. The researchers concluded that the man most likely contracted the disease through a bite from an infected rodent or other animal, the press release notes.
“Isolated cases of transmission from animals to people could explain the different social environments where these ancient diseased humans are discovered,” Krause-Kyora said in the press release. “We see it in societies that are herders in the steppe, hunter-gatherers who are fishing, and in farmer communities—totally different social settings but always spontaneous occurrence of Y. pestis cases.”
From Animal Bite to Flea Infection in 7,000 Years’ Worth of Mutations
The Y. pestis bacteria that infected RV 2039, the researchers surmised, most likely split from its predecessor, Yersinia pseudotuberculosis, which first appeared on Earth about 7,000 years ago. It most likely took Y. pestis over a thousand years to acquire all the mutations necessary for flea-based transmission of the bacteria to humans, the researchers noted.
“What’s most astonishing is that we can push back the appearance of Y. pestis 2,000 years farther than previously published studies suggested,” Krause-Kyora said. “It seems that we are really close to the origin of the bacteria.”
It is unknown how many cases still occur worldwide due to unreliable diagnoses and poor reporting in developing countries. However, data from the World Health Organization (WHO) states that there were 3,248 cases of plague reported worldwide between 2010 and 2015, including 584 deaths. Currently, the three most endemic countries for plague are the Democratic Republic of the Congo, Madagascar, and Peru.
The researchers’ findings illustrate how advances in gene sequencing technologies are helping microbiologists, virologists, and genetic scientists understand the affect mutations have on diseases that have plagued humans since the beginning of humanity itself.
Will this lead to new genomic diagnostics? Perhaps. The research is worth watching.
Microbiologists will want to take note of the CDC’s statement that the illness can masquerade as other diseases
It is the latest example of a bacterium uncommon in the United States that has infected patients in this country—one of whom has died. The three infected patients live in separate states, but genetic analysis indicates their cases may be related.
According to the health alert, “Based on genomic analysis, these three cases (one male, two females; two adults and one child) may share a potential common source of exposure. The first case, identified in March 2021, was fatal. Two other patients were identified in May 2021, one of whom is still hospitalized. One has been discharged to a transitional care unit. None of the patients’ families reported a history of traveling outside of the continental United States.”
The CDC warned, “Symptoms of melioidosis are varied and nonspecific and may include pneumonia, abscess formation, and/or blood infections. Due to its nonspecific symptoms, melioidosis can initially be mistaken for other diseases such as tuberculosis, and proper treatment may be delayed.”
Microbiology Laboratories Should Be on Alert
Melioidosis is typically only seen in subtropical and tropical regions and can be highly fatal. It is unknown how the trio of patients who contracted the illness became infected, but according to the CDC the cases do appear to be connected.
“Testing suggests a common source of infection, but that source has not yet been identified,” a CDC representative told Gizmodo. “CDC is working with states to assess exposures or products these individuals have in common, as well as environmental samples from the states where cases have been identified. Additionally, CDC experts are providing epidemiologic assistance to help investigate the cause of infection,” the CDC added.
“Melioidosis is a serious neglected tropical disease of Southeast Asia, India, and Australia where it is a major cause of pneumonia, abscesses, and sepsis. The fact that it may be gaining a foothold in the US is concerning,” pediatrician Peter Hotez, MD, PhD (above), Dean of the National School of Tropical Medicine, Professor of Pediatrics and Molecular Virology and Microbiology at Baylor College of Medicine, and Director of the Center for Vaccine Development at Texas Children’s Hospital, told Gizmodo. Clinical laboratories and microbiologists will want to monitor these cases for future developments. (Photo copyright: Baylor College of Medicine.)
Melioidosis, also called Whitmore’s disease, was first described by Alfred Whitmore, an English pathologist, in 1912 in what is now present-day Myanmar. The bacterium (Burkholderia pseudomallei) can be found in contaminated soil and water. It is predominately found in tropical climates in Southeast Asia and northern Australia and can affect humans and many species of animals.
Researchers believe the disease may be acquired through the inhalation of contaminated dust particles or water droplets, the ingestion of contaminated water or soil-contaminated food, or other contact with tainted soil, especially through skin abrasions. It is very rare to contract melioidosis from infected individuals.
Melioidosis Masquerades as Other Illnesses
The symptoms of melioidosis are wide-ranging and non-specific and can resemble those of other illnesses. In addition, there are several types of the illness, and they can each act differently depending on where the infection is in the body. The most common symptoms of melioidosis include:
Localized Infection:
Localized pain or swelling
Fever
Ulceration
Abscess
Pulmonary Infection:
Cough
Chest pain
High fever
Headache
Anorexia
Bloodstream Infection:
Fever
Headache
Respiratory distress
Abdominal discomfort
Joint pain
Disorientation
Disseminated Infection:
Fever
Weight loss
Stomach or chest pain
Muscle or joint pain
Headache
Central nervous system/brain infection
Seizures
According to the CDC, the time between an exposure to Burkholderia pseudomallei and the first emergence of Melioidosis symptoms is not clearly defined but could range from one day to many years. However, most infected individuals begin experiencing symptoms of melioidosis within two to four weeks after exposure.
Melioidosis is difficult to diagnose, and some automated bacterial reading instruments can mistake Burkholderia pseudomallei for other bacteria. It is estimated that the disease accounts for 89,000 deaths per year worldwide. Delays in diagnosis and treatment often lead to poor patient outcomes and the mortality rate can exceed 40% in some regions, Nature reported.
The illness is typically treated with appropriate drug therapies including intravenous antimicrobial medications, such as Ceftazidime or Meropenem, followed by an oral antimicrobial therapy such as Trimethoprim-sulfamethoxazole or Amoxicillin/Clavulanic Acid. It may take several months for a patient to be cured of melioidosis, depending on the extent of the infection.
Deadly Bacterium’s Countries of Origin and Spread to the US
According to CDC data, the greatest number of melioidosis cases are reported in Thailand, Malaysia, Singapore, and northern Australia. Cases also have been reported in other Asian countries as well as Mexico and Central America.
Burkholderia pseudomallei does not occur naturally in the US, and cases of melioidosis identified in the US are usually only seen in world travelers and immigrants who come from countries where the disease is widespread. The bacterium has been found in soil in Mexico, so it is possible that it could spread to parts of the US, which has led to concern among microbiologists.
“Due to changes in weather patterns, some pathogens that normally were not present in a particular area might start causing disease,” Alfredo Torres, PhD, Associate Provost, Department of Microbiology and Immunology, University of Texas Medical Branch, told Gizmodo. “Therefore, it is important to make the health professionals aware of this pathogen and the disease that it causes, so quick identification can be done, and treatment is properly used to save lives. Without that, it might be too late for the next melioidosis patient when the proper diagnosis is done.”
The CDC has suggested that healthcare workers consider melioidosis as a possible diagnosis for patients who have compatible symptoms, even if they have not recently traveled outside of the US.
CDC Suggests Rerunning Certain Clinical Laboratory Tests
Because Burkholderia pseudomallei can be mistaken for other bacteria, the CDC also urges the rerunning of clinical laboratory tests using automated identification, especially if another bacterium that is often mistaken for Burkholderia pseudomallei is present, Gizmodo noted.
“CDC encourages healthcare workers to be aware of the potential for more cases and to report cases to their state health departments,” the CDC stated.
The CDC considers the risk of melioidosis to the public in the US to be low, and that the chances of a potential outbreak are unlikely. However, the origins of these three cases remain a mystery and warrant further investigation.
Microbiologists and clinical laboratories should be aware of and remain alert about this potentially fatal illness. It is possible that more cases will arise in the future, especially in the three states where it has already been found.
Six-episode show is based on popular ABC Radio podcast “The Dropout,” which focused on the three-year investigation that brought down clinical laboratory test developer Theranos
While former Theranos CEO Elizabeth Holmes awaits the start of her August 31 criminal fraud trial in a federal court in Northern California, one streaming video service is lining up a star-studded cast to tell the story of the Silicon Valley executive’s fall from grace and the demise of her clinical laboratory blood-testing company.
This six-part series is being produced by Hulu, an on-demand video streaming service offering live and on-demand content. Back in 2019, it announced that it would produce the “The Dropout,” a limited series chronicling Holmes’ rise and fall from Founder and CEO of $9 billion tech company Theranos to criminal defendant.
Hulu says the series will launch this fall, so pathologists and medical laboratory managers have time to set their recorders to capture what may be a compelling story of hubris that took investors and the news media on a wild ride. The Theranos publicity machine was so effective that many hospital CEOs went to their clinical laboratory administrators and told them to delay equipment purchases because Theranos would be able to do the same medical laboratory tests at just pennies on the existing lab-cost dollar.
Holmes’ carefully-crafted public image as Theranos’ CEO drew comparisons to the late Apple CEO Steve Jobs, Business Insider noted. This has made her a popular topic not only among clinical laboratory scientists but also Hollywood moviemakers.
“The Dropout” took its inspiration from the ABC Audio podcast of the same name, hosted by ABC Chief Business, Technology and Economics correspondent Rebecca Jarvis. The ABC Audio podcast’s description provides a glimpse into the direction the miniseries will take.
“Money. Romance. Tragedy. Deception. The story of Elizabeth Holmes and Theranos is an unbelievable tale of ambition and fame gone terribly wrong. How did the world’s youngest self-made female billionaire lose it all in the blink of an eye? How did the woman once heralded as ‘the next Steve Jobs’ find herself facing criminal charges—to which she pleaded not guilty—and up to 20 years in jail? How did her technology, meant to revolutionize healthcare, potentially put millions of patients at risk? And how did so many smart people get it so wrong along the way?” the ABC Audio website states.
The Hulu series originally was to star “Saturday Night Live” cast member Kate McKinnon as Holmes but was recast with Amanda Seyfried in the starring role. According to Variety, the series will include a notable lineup of guest stars including:
Naveen Andrews will play former Theranos President and COO Ramesh Balwani, whose own criminal fraud trial is expected to begin early next year.
A release date for the limited series has not yet been announced, Town and Country reported.
Elizabeth Holmes (above), former CEO of now defunct company Theranos, faces 11 counts of fraud for alleged false claims that the clinical laboratory testing company had created a revolutionary finger-prick technology capable of performing a wide range of clinical laboratory tests. Among the charges are two counts of conspiracy to commit wire fraud and nine counts of wire fraud, for which Holmes could serve up to 20 years in jail if found guilty of all charges, according to court documents. She has pleaded not guilty. (Photo copyright: The Wall Street Journal.)
The ‘Real World’ Wall Street Journal Investigation of Theranos and Holmes
Dark Daily has reported extensively on the Holmes/Theranos saga, including the recent development that Holmes’ repeatedly-delayed trial would be pushed back from mid-July to August 31 because Holmes is due to give birth in July.
Theranos’ alleged deceptions first were brought to light in a series of 2015 investigative reports in The Wall Street Journal (WSJ). Then-WSJ investigative reporter John Carreyrou alleged Theranos had not disclosed publicly that the vast majority of its tests were not being done with proprietary technology, but instead with traditional machines purchased from Siemens AG and other companies.
And for those looking for even more drama centered around the Theranos saga, a feature film starring Jennifer Lawrence as Elizabeth Holmes, titled, “Bad Blood,” remains “in development” according to People magazine. Though the project was announced in 2016, filming has yet to begin.
Meanwhile, clinical laboratory scientists will soon get to watch the next “real world” chapter in the Holmes’ saga play out in federal court later this summer. They will also have multiple opportunities in the coming years to be “entertained” by the Theranos scandal on big and small screens.
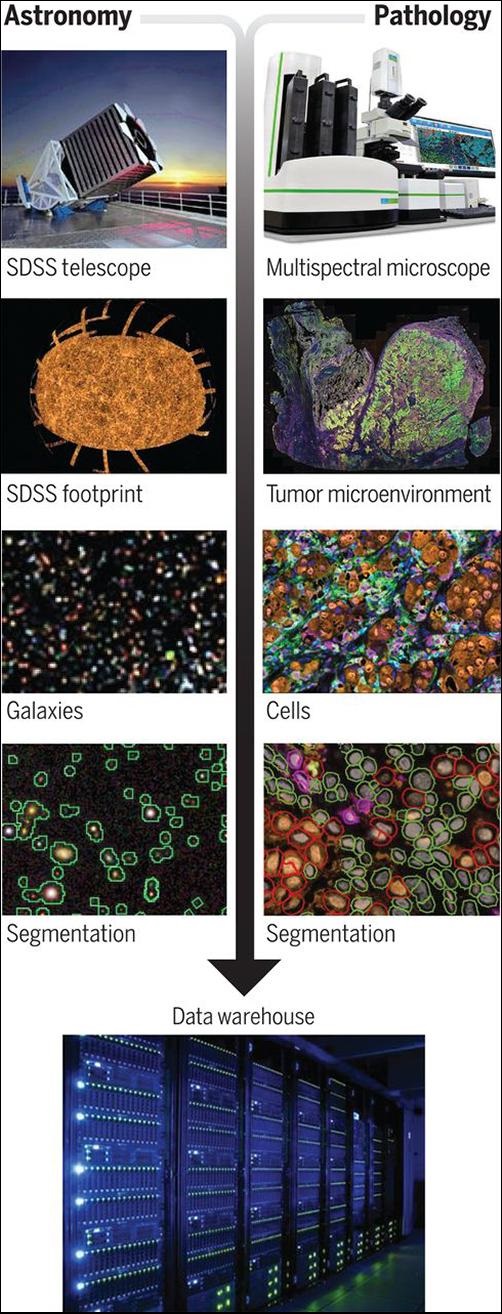
Using algorithmic technology designed for mapping the stars, the scientists have created an imaging/spatial location platform called AstroPath which may help oncologists develop immunotherapies that work best on specific cancers. Such a capability is key to effective precision medicine techniques.
Dark Daily has regularly pointed out that technologies developed in other fields of science will eventually be brought into anatomic pathology and clinical laboratory medicine. Use of the star-mapping technology in oncology and the diagnosis of cancer is one such example.
In “Analysis of Multispectral Imaging with the AstroPath Platform Informs Efficacy of PD-1 Blockade,” published in the journal Science, the multi-institution research team wrote, “Here, we present the AstroPath platform, an end-to-end pathology workflow with rigorous quality control for creating quantitative, spatially resolved mIF [multiplex immunofluorescence] datasets. Although the current effort focused on a six-plex mIF assay, the principles described here provide a general framework for the development of any multiplex assay with single-cell image resolution. Such approaches will vastly improve the standardization and scalability of these technologies, enabling cross-site and cross-study comparisons. This will be essential for multiplex imaging technologies to realize their potential as biomarker discovery platforms and ultimately as standard diagnostic tests for clinical therapeutic decision-making.
“Drawing from the field of astronomy, in which petabytes of imaging data are routinely analyzed across a wide spectral range, [the researchers] developed a platform for multispectral imaging of whole-tumor sections with high-fidelity single-cell resolution. The resultant AstroPath platform was used to develop a multiplex immunofluorescent assay highly predictive of responses and outcomes for melanoma patients receiving immunotherapy,” the researchers added.
Using Star Mapping Software to Fight Cancer
“The application of advanced mapping techniques from astronomy has the potential to identify predictive biomarkers that will help physicians design precise immunotherapy treatments for individual cancer patients,” said Michele Cleary, PhD, CEO of the Mark Foundation for Cancer Research, in a Johns Hopkins news release.
Although the universe we live in and the universe of a cancerous tumor may not seem related, the fact is the same visualization technology can be used to map them both.
“What should be pointed out is that astronomy is mapping the sky in three dimensions, so keeping the spatial relationships while also identify each heavenly body is the goal of these algorithms,” said Robert Michel, Publisher and Editor-in-Chief of Dark Daily and its sister publication The Dark Report.
“Both aspects of that information technology have value in surgical pathology, where the spatial relationship of different cells and cell structures is relevant and important while also having the ability to identify and characterize different types of cells and cell structures. This technology appears to also be capable of identifying multiple biomarkers,” he added.
The image above, taken from the researchers’ Science paper, illustrates the “strong parallels between multispectral analyses in astronomy and emerging multiplexing platforms for pathology.” The researchers wrote, “the next generation of tissue-based biomarkers are likely to be identified by use of large, well-curated datasets. To that end, image analysis approaches originally developed for astronomy were applied to pathology specimens to produce trillions of pixels of robust tissue imaging data and facilitate assay and atlas development.” Anatomic pathologists may be direct recipients of new cancer diagnostic tools based on the AstroPath platform. (Photo copyrights: Johns Hopkins University/Mark Foundation Center for Advanced Genomics/Bloomberg-Kimmel Institute.)
AstroPath Provides 1,000 Times the Information Content from A Single Biopsy
According to the news release, “[The researchers] characterized the immune microenvironment in melanoma biopsies by examining the immune cells in and around the cancer cells within the tumor mass and then identified a composite biomarker that includes six markers and is highly predictive of response to a specific type of an immunotherapy called Anti-PD-1 therapy.”
This is where the use of AstroPath is truly innovative. Previously, researchers could only identify those biomarkers one at a time, through a painstaking process.
“For the last 40 years, pathology analysis of cancer has examined one marker at a time, which provides limited information,” said Drew Pardoll, MD, PhD, Director of the Bloomberg-Kimmel Institute for Cancer Immunotherapy and a Johns Hopkins professor of oncology, in the news release. “Leveraging new technology, including instrumentation to image up to 12 markers simultaneously, the AstroPath imaging algorithms provide 1,000 times the information content from a single biopsy than is currently available through routine pathology,” he added.
More information about a cancerous tumor means clinicians have more tools to combat it. Treatment becomes less about finding the right immunotherapy and more about treating it immediately.
“This facilitates precision cancer immunotherapy—identifying the unique features of each patient’s cancer to predict who will respond to a given immunotherapy, such as anti-PD-1, and who will not. In doing so, it also advances diagnostic pathology from uniparameter to multiparameter assays,” Pardoll said.
Big Data and Data Analysis Is the Future of Precision Medicine
The use of data in science is changing how researchers, clinicians, pathologists, and others provide healthcare in the modern world. When it is properly collected and analyzed, data holds the key to precision medicine’s personalized and targeted patient care.
“Big data is changing science. There are applications everywhere, from astronomy to genomics to oceanography,” said Alexander S. Szalay, PhD, Bloomberg Distinguished Professor and Professor in the Department of Computer Science at Johns Hopkins University, and Director of the Institute for Data Intensive Engineering and Science (IDIES), in the news release.
“Data-intensive scientific discovery is a new paradigm. The technical challenge we face is how to get consistent, reproducible results when you collect data at scale. AstroPath is a step towards establishing a universal standard,” he added.
Should AstroPath prove to be a clinically safe and accurate method for developing precision medicine cancer therapies, anatomic pathologists can look forward to exciting new ways to diagnose cancer and determine the best courses of treatment based on each patient’s unique medical needs.
New biomarkers for cancer therapies derived from the research could usher in superior clinical laboratory diagnostics that identify a patient’s suitability for personalized drug therapies and treatments
Once approved for clinical use, not only would these biomarkers become targets for specific cancer therapies, they also would require development of new diagnostic tests that anatomic pathologists could use to determine whether a biomarker was present in a patient.
If yes, the drug can be administered. If no, the patient is not a candidate for that drug. Thus, this research may produce both diagnostic biomarkers and therapeutic targets.
Relevance of In-Depth Tumor Profiling to Support Clinical Decision-Making
In the Swiss “Tumor Profiler” (TuPro) project, the research team is examining the cellular composition and biology of tumors of 240 patients with melanoma, ovarian cancer, and acute myeloid leukemia. Recruitment for the study began in 2018. Today, the melanoma cohort is fully enrolled, and the ovarian cancer and acute myeloid leukemia cohorts are nearing complete enrollment.
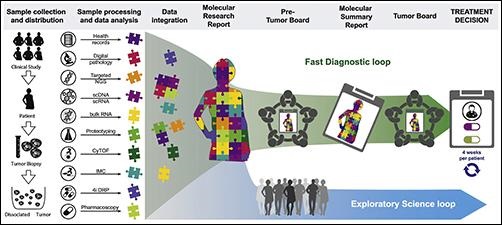
“The Tumor Profiler Study is an observational clinical study combining a prospective diagnostic approach to assess the relevance of in-depth tumor profiling to support clinical decision-making (“fast diagnostic loop”) with an exploratory approach to improve the biological understanding of disease (“exploratory science loop”),” the TuPro website states.
The graphic above taken from the Tumor Profiler project paper illustrates how the TuPro study’s workflow entails patient enrollment, sample collection, analysis by different technology platforms, and data integration, creation and discussion of molecular research and summary reports, discussion of treatment options in pre-tumor boards and the final treatment decision in tumor boards. (Photo copyright: Cancer Cell.)
In their published paper, the Swiss researchers say these three cancers were selected for the study “based on the potential clinical benefit and availability of sufficient tumor material for simultaneous analysis across all technologies.”
According to a University Hospital Basel blog post, the TuPro project examination of each cancer tumor goes “much further than the limited use of molecular biological methods” used by leading hospitals. “This results in huge amounts of data per patient, which we process and analyze using data science methods,” stated data scientist Gunnar Rätsch, PhD (above), Professor for BiomedicalInformatics at ETH Zurich and one of the study’s corresponding authors, in the blog post. This research could lead to new precision medicine biomarkers for clinical laboratory cancer diagnostics and therapies. (Photo copyright: ETH Zurich.)
The TuPro Project’s findings are available to doctors who analyze them at interdisciplinary tumor board meetings and generate treatment options, creating a “fast diagnostic loop” with an estimated four-week turnaround time from surgery to tumor board. “This approach has the potential to alter current diagnostics and paves the way for the translation of comprehensive molecular profiling into clinical decision-making,” the study’s authors wrote in Cancer Cell.
Could Oncologists Be Making Better Precision Medicine Decisions?
In its writeup on the TuPro Project’s research, Precision Oncology News concluded that the Swiss study “is rooted in the researchers’ notion that oncologists are not making the best personalized treatment decisions for patients by relying just on targeted DNA profiling using next-generation sequencing and digital pathology-based tests.
“The researchers within the TuPro consortium hypothesized that integrating a more comprehensive suite of omics tests could lead to a more complete understanding of patients’ tumors, including providing insights into the tumor microenvironment, heterogeneity, and ex vivo responses to certain drugs. This, in turn, could help inform the best course of treatment,” Precision Oncology News added.
“With the Tumor Profiler study, we want to show that the widespread use of molecular biological methods in cancer medicine is not only feasible, but also has specific clinical benefits,” said TuPro consortium member Viola Heinzelmann-Schwarz, MD, Head of Gynecological Oncology at University Hospital Basel, in an ET Zurich news release.
New Precision Medicine Biomarkers from TuPro’s Molecular Analysis
Researchers in the study also are investigating whether and what influence the molecular analysis had on doctors’ therapy decisions.
The University Hospital Basal blog notes the long-term benefits of the Tumor Profiler approach is to expand the personalized-medicine therapy options for patients, including determining whether patients would benefit in certain cases “if they were not treated with drugs from standard therapy, but with drugs that have been approved for other types of cancer.”
Anatomic pathologists and clinical laboratory scientists will want to take note of the TuPro project’s ultimate success or failure, since it could usher in changes in cancer treatments and bring about the need for new diagnostic tests for cancer biomarkers.
As many clinical laboratory scientists know, gene sequencing technology continues to become faster, more accurate, and less expensive per whole human genome sequenced
In February, Dark Daily reported that Personalis, Inc. (NASDAQ:PSNL) had delivered its 100,000th whole human genome sequence to the US Department of Veterans Affairs Million Veterans Program (VA MVP). Now, the Menlo Park, Calif.-based cancer genomics company has topped that achievement by delivering its 125,000 whole human genome sequence!
“This represents another important landmark for both the program and for Personalis,” said John West, Chief Executive Officer, Personalis, in a news release. “We congratulate the VA MVP for reaching this important milestone.
“We strongly believe that the research projects being performed today will enable precision medicine in healthcare systems in the future across a wide range of disease areas,” he added. This is a positive development for clinical laboratories, as personalized medicine services require a lab to sequence and interpret the patient’s DNA.
Personalis was contracted with the US federal government to perform genetic research in 2012 and has delivered 50,000 genomes to the VA MVP during the past twelve months.
The Personalis and VA MVP researchers seek to gain a better understanding of how genetic variants affect health. Before the COVID-19 pandemic hit the US, the VA was enrolling veterans in the Million Veterans Program at 63 VA medical centers across the country. There are currently about 830,000 veterans enrolled in the venture and the VA is expecting two million veterans to eventually sign up for the sequencing project.
“As a global leader in genomic sequencing and comprehensive analytics services, Personalis is uniquely suited to lead these population-scale efforts and we are currently in the process of expanding our business operations internationally,” West added.
According to the press release, “the VA MVP provides researchers with a rich resource of genetic, health, lifestyle, and military-exposure data collected from questionnaires, medical records, and genetic analyses. By combining this information into a single database, the VA MVP promises to advance knowledge about the complex links between genes and health.”
NIH All of Us Research Program Supports Precision Medicine Goals Another genetic research project being conducted by the US National Institutes of Health (NIH) is the All of Us Research Program. Using donated personal health information from thousands of participants, the NIH researchers seek to “learn how our biology, lifestyle, and environment affect health,” according to the program’s website.
“We’re changing the paradigm for research,” said Josh Denny, MD (above), Chief Executive Officer of the All of Us Research Program, in an NIH news release. “Participants are our most important partners in this effort, and we know many of them are eager to get their genetic results and learn about the science they’re making possible. We’re working to provide that valuable information in a responsible way,” he added. Clinical laboratories may soon see new precision medicine biomarkers derived from this type of research. (Photo copyright: Vanderbilt University.)
The All of Us Research Program intends to have at least one million US participants take part in the research. The researchers hope to help scientists discover new knowledge regarding how biological, environmental, and behavioral factors influence health, and to learn to tailor healthcare to patients’ specific medical needs, a key component of precision medicine.
Participants in the project share personal information via a variety of methods, including surveys, electronic health records, and biological samples.
A Better Sampling of Under-Represented Communities
Since opening enrollment in 2018, more than 270,000 people have contributed blood, urine, and saliva samples to the All of Us Research Program. More than 80% of the participants come from communities that are traditionally under-represented in biomedical research.
“We need programs like All of Us to build diverse datasets so that research findings ultimately benefit everyone,” said Brad Ozenberger, PhD, Genomics Program Director, All of Us, in the NIH news release. “Too many groups have been left out of research in the past, so much of what we know about genomics is based mainly on people of European ancestry. And often, genomic data are explored without critical context like environment, economics, and other social determinants of health. We’re trying to help change that, enabling the entire research community to help fill in these knowledge gaps.”
The All of Us Research Project’s analysis of the collected data includes both whole-genome sequencing (WGS) and genotyping and is taking a phased approach in returning genetic data to participants.
Participants initially receive data about their genetic ancestry and traits. That is followed later by health-related results, such as how their genetic variants may increase the risk of certain diseases and how their DNA may affect their reaction to drug therapies.
Genetic researchers hope programs like these will lead to improved in vitro diagnostics and drug therapies. Genetic sequencing also may lead to new diagnostic and therapeutic biomarkers for clinical laboratories.