Results of the UK study confirm for clinical laboratory professionals the importance of fully understanding the design and function of SNP chips they may be using in their labs
Here is another example of a long-established clinical laboratory test that—upon new evidence—turns out to be not as accurate as once thought. According to research conducted at the University of Exeter in Devon, UK, Single-nucleotide polymorphism (SNP) chips (aka, SNP microarrays)—technology commonly used in commercial genetic testing—is inadequate at detecting rare gene variants that can increase breast cancer risk.
A news release announcing the results of the large-scale study states, “A technology that is widely used by commercial genetic testing companies is ‘extremely unreliable’ in detecting very rare variants, meaning results suggesting individuals carry rare disease-causing genetic variants are usually wrong.”
Why is this a significant finding for clinical laboratories? Because medical laboratories performing genetic tests that use SNP chips should be aware that rare genetic variants—which are clinically relevant to a patient’s case—may not be detected and/or reported by the tests they are running.
UK Researchers Find ‘Shockingly High False Positives’
The conclusion reached by the Exeter researchers, the BMJ study states, is that “SNP chips are extremely unreliable for genotyping very rare pathogenic variants and should not be used to guide health decisions without validation.”
Leigh Jackson, PhD, Lecturer in Genomic Medicine at University of Exeter and co-author of the BMJ study, said in the news release, “The number of false positives on rare genetic variants produced by SNP chips was shockingly high. To be clear: a very rare, disease-causing variant detected using [an] SNP chip is more likely to be wrong than right.”
In the news release, Caroline Wright, PhD (above), Professor in Genomic Medicine at the University of Exeter Medical School and senior author of the BMJ study, said, “SNP chips are fantastic at detecting common genetic variants, yet we have to recognize that tests that perform well in one scenario are not necessarily applicable to others.” She added, “We’ve confirmed that SNP chips are extremely poor at detecting very rare disease-causing genetic variants, often giving false positive results that can have profound clinical impact. These false results had been used to schedule invasive medical procedures that were both unnecessary and unwarranted.” (Photo copyright: University of Exeter.)
Large-Scale Study Taps UK Biobank Data
The Exeter researchers were concerned about cases of unnecessary invasive medical procedures being scheduled by women after learning of rare genetic variations in BRCA1 (breast cancer type 1) and BRCA2 (breast cancer 2) tests.
“The inherent technical limitation of SNP chips for correctly detecting rare genetic variants is further exacerbated when the variants themselves are linked to very rare diseases. As with any diagnostic test, the positive predictive value for low prevalence conditions will necessarily be low in most individuals. For pathogenic BRCA variants in the UK Biobank, the SNP chips had an extremely low positive predictive value (1-17%) when compared with sequencing. Were these results to be fed back to individuals, the clinical implications would be profound. Women with a positive BRCA result face a lifetime of additional screening and potentially prophylactic surgery that is unwarranted in the case of a false positive result,” they wrote.
Using UK Biobank data from 49,908 participants (55% were female), the researchers compared next-generation sequencing (NGS) to SNP chip genotyping. They found that SNP chips—which test genetic variation at hundreds-of-thousands of specific locations across the genome—performed well when compared to NGS for common variants, such as those related to type 2 diabetes and ancestry assessment, the study noted.
“Because SNP chips are such a widely used and high-performing assay for common genetic variants, we were also surprised that the differing performance of SNP chips for detecting rare variants was not well appreciated in the wider research or medical communities. Luckily, we had recently received both SNP chip and genome-wide DNA sequencing data on 50,000 individuals through the UK Biobank—a population cohort of adult volunteers from across the UK. This large dataset allowed us to systematically investigate the performance of SNP chips across millions of genetic variants with a wide range of frequencies, down to those present in fewer than 1 in 50,000 individuals,” wrote Wright and Associate Professor of Bioinformatics and Human Genetics at Exeter, Michael Weedon, PhD, in a BMJ blog post.
The Exeter researchers also analyzed data from a small group of people in the Personal Genome Project who had both SNP genotyping and sequencing information available. They focused their analysis on rare pathogenic variants in BRCA1 and BRCA2 genes.
The researchers found:
The rarer the variant, the less reliable the test result. For example, for “very rare variants” in less than one in 100,000 people, 84% found by SNP chips were false positives.
Low positive predictive values of about 16% for very rare variants in the UK Biobank.
Nearly all (20 of 21) customers of commercial genetic testing had at least one false positive rare disease-causing variant incorrectly genotyped.
SNP chips detect common genetic variants “extremely well.”
Advantages and Capabilities of SNP Chips
Compared to next-gen genetic sequencing, SNP chips are less costly. The chips use “grids of hundreds of thousands of beads that react to specific gene variants by glowing in different colors,” New Scientist explained.
Common variants of BRCA1 and BRCA2 can be found using SNP chips with 99% accuracy, New Scientist reported based on study data.
However, when the task is to find thousands of rare variants in BRCA1 and BRCA2 genes, SNP chips do not fare so well.
“It is just not the right technology for the job when it comes to rare variants. They’re excellent for the common variants that are present in lots of people. But the rarer the variant is, the less likely they are to be able to correctly detect it,” Wright told CNN.
SNP chips can’t detect all variants because they struggle to cluster needed data, the Exeter researchers explained.
“SNP chips perform poorly for genotyping rare genetic variants owing to their reliance on data clustering. Clustering data from multiple individuals with similar genotypes works very well when variants are common,” the researchers wrote. “Clustering becomes more difficult as the number of people with a particular genotype decreases.”
Clinical laboratories Using SNP Chips
The researchers at Exeter unveiled important information that pathologists and medical laboratory professionals will want to understand and monitor. Cancer patients with rare genetic variants may not be diagnosed accurately because SNP chips were not designed to identify specific genetic variants. Those patients may need additional testing to validate diagnoses and prevent harm.
At-home genetic test kits face scrutiny for providing information that may provide consumers with an incomplete picture of their genetic health risks and ancestry
Genetic testing for disease risk and heritage are hugely popular. But though clinical laboratory and pathology professionals understand the difference between a doctor-ordered genetic health risk (GHR) test and a direct-to-consumer (DTC) genetic test, the typical genetic test customer may not. And misunderstanding the results of a DTC at-home genetic test can lead to confusion, loss of privacy, and potential harm, according to Consumer Reports.
To help educate consumers about the “potential pitfalls” of at-home DTC testing kits offered by companies such as Ancestry and 23andMe, Consumer Reports has published an article, titled, “Read This Before You Buy a Genetic Testing Kit.” The article covers “four common claims from the manufacturers of these products, whether they deliver, and what to know about their potential pitfalls.”
Are Genetic Ancestry Tests Accurate?
Ancestry and 23andMe are the DTC genetic test industry leaders, with databases of genetic information about 18 million individuals and 10 million individuals respectively. According to a Consumer Reports survey, as of October 2020 about one in five Americans had taken a DTC genetic test. Reported reasons for doing so included:
66% of respondents wanted to learn more about their ancestry.
20% wanted to locate relatives.
18% wanted to learn more about their health.
11% wanted to learn if they have or are a carrier for any medical conditions.
3% wanted to get a medical test they could not get through their doctor.
Though DTC genetic tests remain popular, Consumer Reports is now warning consumers to view the genealogical or medical insights gleaned through these tests with caution. “If you go in there thinking that this test is going to tell you who you are, you’re going to be wrong,” Wendy Roth, PhD (above), Associate Professor of Sociology at the University of Pennsylvania, told the publication. (Photo copyright: University of Pennsylvania.)
As Consumer Reports notes, doctor-ordered genetic health risk (GHR) testing typically aims to answer a specific question about a patient’s risk for a certain disease. DTC at-home genetic testing, on the other hand, examines a “whole range of variants that have been linked—sometimes quite loosely—to a number of traits, some not related to your health at all.
“Think of it this way: When your doctor orders genetic testing, it’s akin to fishing for a particular fish, in a part of the ocean where it’s known to live,” Consumer Reports noted, “A DTC test is more like throwing a net into the ocean and seeing what comes back.”
In its article, Consumer Reports addressed four common DTC genetic test claims:
The Tests Can Find Far-Flung Relatives: While the tests can unearth people in its database whom you might be related to, 9% of respondents in the Consumer Reports survey discovered unsettling information about a relative.
Testing Can Uncover Where Your Ancestors Are From: Genetic tests may show the percentage of your DNA that comes from Europe or Asia or Africa, but accuracy depends on how many DNA samples a company has from a particular region. As genetic test manufacturers’ reference databases widen, a customer’s genetic ancestry test results can “change over time.” Also, finding a particular variation in genetic code does not definitively place someone in a specific region, or ethnic or racial group.
Genetic Tests Can Reveal Your Risk for Certain Diseases: Testing companies such as 23andMe are authorized by the Food and Drug Administration (FDA) to offer physician-mediated tests, which are analyzed in a federally-certified clinical laboratory. However, test results may provide a false sense of security because DTC tests look for only select variants known to cause disease.
The Tests Can Tell What Diet Is Best for You: Incorporating genetic information into diet advice has the potential to be transformative, but the science is not yet there to offer personalized nutritional advice.
Consumer Reports pointed to a 2020 study published in the MDPI journal Nutrients, titled, “Direct-to-Consumer Nutrigenetics Testing: An Overview,” which evaluated 45 DTC companies offering nutrigenetics testing and found a need for “specific guidelines” and “minimum quality standards” for the services offered. For example, the study authors noted that more than 900 genetic variants contribute to obesity risk. However, weight-loss advice from DTC test companies was based on a “limited set of genetic markers.”
In the Consumer Reports article, Mwenza Blell, PhD, a biosocial medical anthropologist and Rutherford Fellow and NUAcT Fellow at Newcastle University in the United Kingdom, said “genetic ancestry tests are closer to palm reading than science.”
Seattle Cancer Care Alliance and an Associate Professor of Oncology at the University of Washington, fears consumers “miss important limitations on a test’s scope” or “misunderstand critical nuances in the results.”
Cheng says the ability to use flexible or health savings accounts (HSAs) to cover the cost of 23andMe’s GHR assessments, as well as the FDA’s approval of 23andMe’s Personal Genome Service Pharmacogenetic Reports test on medication metabolism, may have added to the confusion.
“This may further mislead people into thinking these tests are clinically sound. Again, they are not,” Cheng wrote.
As an oncologist, Cheng is particularly concerned about consumer GHR testing for heritable cancer risk, which screen for only a handful of genetic variants.
“The results are inadequate for most people at high risk of cancers associated with inherited mutations in BRCA1 or BRCA2 genes, including families whose members have experienced ovarian cancer, male breast cancer, multiple early breast cancers, pancreatic cancer, or prostate cancer,” Cheng wrote. “Put simply, this recreational test has zero value for the majority of people who may need it for true medical purposes.”
DTC genetic health-risk assessments may one day lead to consumers collecting samples at home for tests that aid in the diagnosis of disease. In the meantime, clinical laboratory professionals can play a role in educating the public about the limitations of current DTC genetic test offerings.
With improved genetic sequencing comes larger human genome databases that could lead to new diagnostic and therapeutic biomarkers for clinical laboratories
As the COVID-19 pandemic grabbed headlines, the human genome database at the US Department of Veterans Affairs Million Veterans Program (MVP) quietly grew. Now, this wealth of genomic information—as well as data from other large-scale genomic and genetic collections—is expected to produce new biomarkers for clinical laboratory diagnostics and testing.
In December, cancer genomics company Personalis, Inc. (NASDAQ:PSNL) of Menlo Park, Calif., achieved a milestone and delivered its 100,000th whole human genome sequence to the MVP, according to a news release, which also states that Personalis is the sole sequencing provider to the MVP.
The VA’s MVP program, which started in 2011, has 850,000 enrolled veterans and is expected to eventually involve two million people. The VA’s aim is to explore the role genes, lifestyle, and military experience play in health and human illness, notes the VA’s MVP website.
Health conditions affecting veterans the MVP is researching include:
The VA has contracted with Personalis through September 2021, and has invested $175 million, Clinical OMICS reported. Personalis has earned approximately $14 million from the VA. That’s about 76% of the company’s revenue, according to 2nd quarter data, Clinical OMICS noted.
“The VA MVP is the largest whole genome sequencing project in the United States, and this is a significant milestone for both the program and for Personalis,” said John West (above with wife Judy), Founder and CEO of Personalis, in the news release. “Population-scale sequencing projects of this nature represent a cornerstone in our effort to accelerate the advancement of precision medicine across a wide range of disease areas,” he added. (Photo copyright: MIT Technology Review.)
Database of Veterans’ Genomes Used in Current Research
What has the VA gained from their investment so far? An MVP fact sheet states researchers are tapping MVP data for these and other veteran health-related studies:
Differentiating between prostate cancer tumors that require treatment and others that are slow-growing and not life-threatening.
How genetics drives obesity, diabetes, and heart disease.
How data in DNA translates into actual physiological changes within the body.
Gene variations and patients’ response to Warfarin.
NIH Research Program Studies Effects of Genetics on Health
Another research program, the National Institutes of Health’s All of Us study, recently began returning results to its participants who provided blood, urine, and/or saliva samples. The NIH aims to aid research into health outcomes influenced by genetics, environment, and lifestyle, explained a news release. The program, launched in 2018, has biological samples from more than 270,000 people with a goal of one million participants.
“We’re changing the paradigm for research. Participants are our most important partners in this effort, and we know many of them are eager to get their genetic results and learn about the science they’re making possible,” said Josh Denny, MD, CEO of the NIH’s All of Us research program in the news release. Denny, a physician scientist, was Professor of Biomedical Informatics and Medicine, Director of the Center for Precision Medicine and Vice President for Personalized Medicine at Vanderbilt University Medical Center prior to joining the NIH. (Photo copyright: National Institutes of Health.)
Inclusive Data Could Aid Precision Medicine
The news release notes that more than 80% of biological samples in the All of Us database come from people in communities that have been under-represented in biomedical research.
“We need programs like All of Us to build diverse datasets so that research findings ultimately benefit everyone,” said Brad Ozenberger, PhD, All of Us Genomics Program Director, in the news release.
Precision medicine designed for specific healthcare populations is a goal of the All of Us program.
“[All of Us is] beneficial to all Americans, but actually beneficial to the African American race because a lot of research and a lot of medicines that we are taking advantage of today, [African Americans] were not part of the research,” Chris Crawford, All of US Research Study Navigator, told the Birmingham Times. “As [the All of Us study] goes forward and we get a big diverse group of people, it will help as far as making medicine and treatment that will be more precise for us,” he added.
Large Databases Could Advance Care
Genome sequencing technology continues to improve. It is faster, less complicated, and cheaper to sequence a whole human genome than ever before. And the resulting sequence is more accurate.
Thus, as human genome sequencing databases grow, researchers are deriving useful scientific insights from the data. This is relevant for clinical laboratories because the new insights from studying bigger databases of genomic information will produce new diagnostic and therapeutic biomarkers that can be the basis for new clinical laboratory tests as well as useful diagnostic assays for anatomic pathologists.
Clinical laboratory managers and pathology practice administrators should consider how these trends may affect their business and patients when planning for the future.
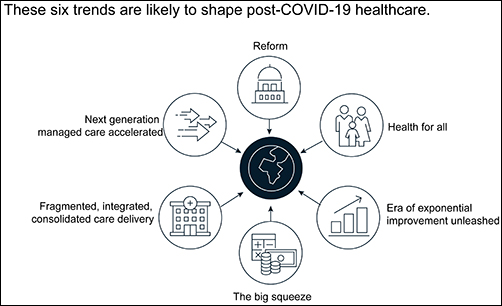
The McKinsey graphic above illustrates the “six trends that are likely to shape post-COVID-19 healthcare.” Clinical laboratories that support health networks struggling with any of these challenges should take steps to prepare for anticipated changes to healthcare delivery. (Graphic copyright: McKinsey and Company.)
1: Healthcare Reform
McKinsey identified three areas where the coronavirus pandemic may impact healthcare reform:
“COVID-19-era waivers that could become permanent.
“Actions that may be taken to strengthen the healthcare system to deal with pandemics.
“Reforms to address the COVID-19-induced crisis.”
McKinsey reports that “the Centers for Medicare and Medicaid Services has introduced more than 190 waivers since the beginning of March 2020.” These waivers can affect all aspects of healthcare, from clinical practice to reimbursement. Some of them, according to McKinsey, are “only relevant during the crisis (for example, the waiver of intensive care unit death reporting). A retrospective assessment of others (for example, expansion of telehealth access) could reveal beneficial innovation worth preserving.”
Several areas that McKinsey says are clearly ripe for reform include improving the resiliency of the healthcare system and the way the system is funded.
Public sector budgets are generally kept strictly separate, each with its own rules and policies that dictate operations. But in his article, “After COVID-19—Thinking Differently About Running the Health Care System,” published in JAMA Health Network, Stuart M. Butler, PhD, Senior Fellow in Economic Studies at the Brookings Institution, wrote, “The intensity of the COVID-19 pandemic … is forcing jurisdictions all across the country to find ways to be nimble so that multiple agencies can work together.”
Thus, McKinsey recommends, “Given the substantial shifts in relative market positioning among industry players that prior reforms have created, leaders would do well to plan ahead now.”
2: Better Access to Healthcare Services
Some people who develop COVID-19 are at far greater risk of hospitalization and death than others, including those who have:
Chronic health conditions, including obesity.
Mental and behavioral health challenges, such as substance abuse.
Unmet social needs, such as food or housing insecurity.
Poor access to healthcare.
McKinsey wrote that these “intersecting health and social conditions,” combined with certain races that have higher risk for severe complications, including Black, Indian, and Hispanic/Latino Americans, “correlated with poorer health outcomes.”
Value-based healthcare, telehealth, and greater attention to the social determinants of health may help address some of these issues, McKinsey notes, but the pandemic has shined a spotlight on how lack of care increases risk for certain populations during a public health crisis.
3: Era of Exponential Improvement Unleashed
Some of the trends that appear to be accelerating as a result of the pandemic are good news. McKinsey cites several benefits, including:
Improved understanding of patients.
Delivery of more convenient and individualized care.
$350-$410 billion in annual revenue by 2025.
Through telehealth and other types of virtual care enabled by digital technology, “intuitive healthcare ecosystems” may arise and offer a more integrated experience for patients and their caregivers, McKinsey notes.
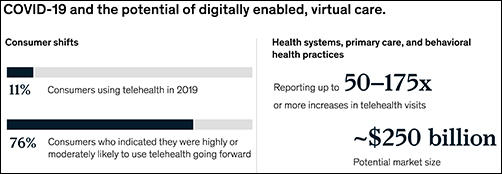
“While the pace of change in healthcare has lagged other industries in the past, potential for rapid improvement may accelerate due to COVID-19. An example is the exponential uptake of digitally enabled, virtual care,” McKinsey wrote. “Our analysis … showed that health systems, primary care, and behavioral health practices are reporting increases of more than 50–175 times in telehealth visits, and the potential market size for virtual care could reach around $250 billion.”
The graphic above is taken from the McKinsey and Co. report, which noted, “Proliferation of digitally enabled, virtual care could further contribute to the rise of personalized and intuitive healthcare ecosystems [that] have the potential to deliver an integrated experience to consumers, enhance productivity of providers, engage both formal and informal caregivers, and improve outcomes while lowering cost.” (Graphic copyright: McKinsey and Company.)
4: The Big Squeeze
The pandemic has caused an enormous outflow of cash from the healthcare system, and some experts don’t expect an injection of funding until 2022. “This outflow is expected to be primarily driven by coverage shifts out of employer-sponsored insurance and possible coverage reductions by employers as well as Medicaid rate pressures from states,” McKinsey states.
“We estimate that COVID-19 could depress healthcare industry earnings by between $35 billion and $75 billion compared with baseline expectations,” McKinsey predicted, adding, “Select high-growth segments will remain attractive (for example, virtual care, home health, software and platforms, specialty pharmacy) and will disproportionally drive growth. These high-growth areas are expected to increase more than 10% over the next five years, while other segments may stagnate or decline altogether.”
5: Fragmented, Integrated, Consolidated Care Delivery
McKinsey says, “The shift of care out of hospitals is not new but has been accelerated by COVID-19.” Rather than the hospital being the center of care delivery, patients are increasingly choosing to receive care at a range of sites across many healthcare ecosystems that are connected digitally and through analytics.
Early in the course of the pandemic, visits to ambulatory care facilities dropped nearly 60% by early April. But by mid-May, those visits were beginning to rebound.
In, “The Impact of the COVID-19 Pandemic on Outpatient Visits: A Rebound Emerges,” the Commonwealth Fund reported that “the relative decline in visits remains largest among surgical and procedural specialties and pediatrics” but is “smaller in other specialties, such as adult primary care and behavioral health.”
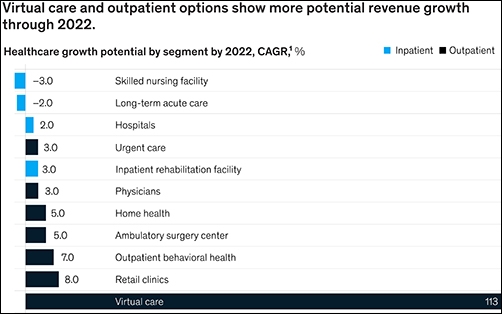
The McKinsey graphic above shows how “virtual care and outpatient options show more potential revenue growth through 2022.” Clinical laboratories that support those healthcare settings, especially ambulatory surgery, behavioral health, and retail clinics, should experience similar growth. (Graphic copyright: McKinsey and Company.)
6: Adoption of Next-Generation Managed Care Is Accelerating
How will COVID-19 affect the managed care industry? McKinsey says the “next generation” of managed care might use Medicare Advantage as a model.
“Payers pursuing the next generation of managed care model (through deep integration with care delivery) demonstrate better financial performance, capturing an additional 50 basis points of earnings before interest, taxes, depreciation, and amortization above expectation,” McKinsey noted, adding, “Employers and payers could consider fundamentally rethinking how employer-sponsored health coverage is structured. Learning from Medicare Advantage could provide inspiration for such a reimagination.”
What Should Clinical Laboratory Managers Do?
The McKinsey article concludes by stating, “While the challenges are numerous, leaders who seize the mindset that “disruptive change provides an opportunity to separate yourself from the pack” will build organizations meaningfully stronger than the ones they ran going into the crisis.”
The McKinsey article authors recommend that healthcare organizations take several proactive steps, including:
Launch a plan-ahead team.
Question your role and your future business model.
Prepare to transform your business.
Reimagine your organization to make faster decisions.
Take action to drive health equity.
Though the McKinsey and Company article covered healthcare in general, many of the authors’ observations and recommendations can apply to clinical laboratories and pathology groups as well and may be valuable in future planning.
CEOs of NorDx Laboratories, Sonora Quest Laboratories, and HealthPartners/Park Nicollet Laboratories expect demand for SARS-CoV-2 tests to only increase in coming months
The short answer is that large volumes of COVID-19 testing will be needed for the remaining weeks of 2020 and substantial COVID-19 testing will occur throughout 2021 and even into 2022. This has major implications for all clinical laboratories in the United States as they plan budgets for 2021 and attempt to manage their supply chain in coming weeks. The additional challenge in coming months is the surge in respiratory virus testing that is typical of an average influenza season.
Stan Schofield (above center), President of NorDx, a regional laboratory corporation that supports an integrated delivery system at MaineHealth in Portland, Maine.
Rick L. Panning (above right), MBA, MLS(ASCP)CM, retired as of Oct. 2 from the position of Senior Administrative Director of Laboratory Services for HealthPartners and Park Nicollet in Minneapolis-St. Paul, Minnesota.
Each panelist was asked how his parent health system and clinical laboratory was preparing to respond to the COVID-19 pandemic through the end of 2020 and into 2021.
First to answer was Panning, whose laboratory serves the Minneapolis-Saint Paul market.
A distinguishing feature of healthcare in the Twin Cities is that it is at the forefront of operational and clinical integration. Competition among health networks is intense and consumer-focused services are essential if a hospital or physician office is to retain its patients and expand market share.
Panning first explained how the pandemic is intensifying in Minnesota. “Our state has been on a two-week path of rising COVID-19 case numbers,” he said. “That rise is mirrored by increased hospitalizations for COVID-19 and ICU bed utilization is going up dramatically. The number of hospitalized COVID-19 patients has doubled during this time and Minnesota is surrounded by states that are even in worse shape than us.”
These trends are matched by the outpatient/outreach experience. “We are also seeing more patients use virtual visits to our clinics, compared to recent months,” noted Panning. “About 35% of clinical visits are virtual because people do not want to physically go into a clinic or doctor’s office.
“Given these recent developments, we’ve had to expand our network of specimen collection sites because of social distancing requirements,” explained Panning. “Each patient collection requires more space, along with more time to clean and sterilize that space before it can be used for the next patient. Our lab and our parent health system are focused on what we call crisis standards of care.
“For all these reasons, our planning points to an ongoing demand for COVID-19 testing,” he added. “Influenza season is arriving, and the pandemic is accelerating. Given that evidence, and the guidance from state and federal officials, we expect our clinical laboratory will be providing significant numbers of COVID-19 tests for the balance of this year and probably far into 2021.”
COVID-19 Vaccine Could Increase Antibody and Rapid Molecular Testing
Arizona is seeing comparable increases in new daily COVID-19 cases. “There’s been a strong uptick that coincides with the governor’s decision to loosen restrictions that allowed bars and exercise clubs to open,” stated Dexter. “We’ve gone from a 3.8% positivity rate up to 7% as of last night. By the end of this week, we could be a 10% positivity rate.”
Looking at the balance of 2020 and into 2021, Dexter said, “Our lab is in the midst of budget planning. We are budgeting to support an increase in COVID-19 PCR testing in both November and December. Arizona state officials believe that COVID-19 cases will peak at the end of January and we’ll start seeing the downside in February of 2021.”
The possible availability of a SARS-CoV-2 vaccine is another factor in planning at Dexter’s clinical laboratory. “If such a vaccine becomes available, we think there will be a significant increase in antibody testing, probably starting in second quarter and continuing for the balance of 2021. There will also be a need for rapid COVID-19 molecular tests. Today, such tests are simply unavailable. Because of supply chain difficulties, we predict that they won’t be available in sufficient quantities until probably late 2021.”
COVID-19 Testing Supply Shortages Predicted as Demand Increases
At NorDx Laboratories in Portland, Maine, the expectation is that the COVID-19 pandemic will continue even into 2022. “Our team believes that people will be wearing masks for 18 more months and that COVID-19 testing with influenza is going to be the big demand this winter,” observed Schofield. “The demand for both COVID-19 and influenza testing will press all of us up against the wall because there are not enough reagents, plastics, and plates to handle the demand that we see building even now.
“Our hospitals are already preparing for a second surge of COVID-19 cases,” he said.
COVID-19 patients will be concentrated in only three or four hospitals. The other hospitals will handle routine work. Administration does not want to have COVID-19 patients spread out over 12 or 14 hospitals, as happened last March and April.
“Administration of the health system and our clinical laboratory think that the COVID-19 test volume and demand for these tests will be tough on our lab for another 12 months. This will be particularly true for COVID-19 molecular tests.”
As described above, the CEOs of these three major clinical laboratories believe that the demand for COVID-19 testing will continue well into 2021, and possibly also into 2022. A recording of the full session was captured by the virtual Executive War College and, as a public service to the medical laboratory and pathology profession, access to this recording will be provided to any lab professional who contacts info@darkreport.com and provides their email address, name, title, and organization.
Robert L. Michel, Panelist—Publisher, Editor-in-Chief, The Dark Report and Dark Daily, Spicewood, Texas.
Given the importance of sound strategic planning for all clinical laboratories and pathology groups during their fall budget process, the virtual Executive War College is opening this session to all professionals in laboratory medicine, in vitro diagnostics, and lab informatics.
Pathologists and clinical laboratory scientists know that influenza vaccines typically produce short-lived protection and researchers have new clues as to why this is true
With so much interest in development of a COVID-19 vaccine, findings by researchers at Atlanta’s Emory Vaccine Center into why the vaccine for influenza (Flu) is so short-lived offer a new window on how the body’s immune system responds to invading viruses and what happens to the immunity over time.
Because the autumn influenza season is just weeks away, these insights into the body’s immune response to influenza will be of interest to clinical laboratories that provide testing for influenza, as well as SARS-CoV-2, the coronavirus that causes COVID-19.
Clinical laboratory managers recognize that an influenza vaccine is an annual imperative for people—especially the elderly and those with existing comorbidities—and medical laboratory tests are typically used to diagnose the illness and identify which strains of viruses are present. The flu vaccine is even more important amid the COVID-19 pandemic, infectious disease authorities say.
The scientists at the Emory Vaccine Center published their findings in the journal Science.
Not so with influenza vaccines. The immunity they impart generally only lasts for a single flu season and are “lost within one year,” the Emory study notes.
As Genetic Engineering and Biotechnology News (GEN) explains, the influenza genome has eight RNA segments which can change as the virus enters a cell. This antigenic shift creates new influenza strains that require updated vaccines, GEN noted.
However, the Emory researchers stated that “The fact that a small number did persist over one year raises prospects that the longevity of flu vaccines can be improved and provides key information for the development of universal vaccines against influenza.”
Bone Marrow Has Major Role in Producing New Flu Antibodies
The Emory study focused on the influenza vaccine’s role in how it affects the immune system and what needs to change to create a longer-lasting influenza vaccine. “Our results suggest that most bone marrow plasma cells (BMPC) generated by influenza vaccination in adults are short-lived. Designing strategies to enhance their persistence will be key,” the Emory researchers wrote in Science.
The scientists analyzed bone marrow from 53 healthy volunteers (age 20 to 45). An Emory news release states that bone marrow is the “home base for immune cells producing antibodies.”
Besides the bone marrow, the researchers also examined blood samples from the volunteers, all of which was collected between 2009 and 2018:
before influenza vaccination,
one month after influenza vaccination, and
one year post vaccination.
Through DNA sequencing the samples, the Emory researchers found the number of flu-specific cells increased from 0.8% to 1.9% after one month. They concluded that an annual vaccine does increase antibody-producing cells for influenza in bone marrow.
However, in follow-up visits one year after vaccination, they found that the number of cells present in the volunteers had fallen back to the starting point.
“Specific cells produced by the vaccine … produced unique antibodies that can be identified using sequencing techniques,” Carl Davis, PhD, postdoctoral fellow in the Rafi Ahmed Laboratory at Emory and first author of the paper, said in the news release, adding, “We could see that these new antibodies expanded in the bone marrow one month after vaccination and then contracted after one year.”
He continued, “On the other hand, antibodies against influenza that were in the bone marrow before the vaccine was given stayed at a constant level over one year.”
Vaccine Adjuvants Help Boost Immunity
A vaccine additive called an adjuvant could be the answer to extending the power of influenza vaccines, the Emory scientists noted.
“Just getting to the bone marrow is not enough. A plasma cell has to find a niche within the bone marrow and establish itself there and undergo gene expression and metabolism changes that promote longevity,” Rafi Ahmed, PhD, Director of the Emory Vaccine Center, said in the news release.
“It’s totally crazy (that the most commonly used influenza vaccines don’t include an adjuvant), Ahmed told Science. “I’m hoping that things will change in the influenza vaccine world, and 10 years from now, you will not be getting any nonadjuvanted vaccines.”
According to USA Today, about 20-million “essential” workers will likely be the first to receive the new COVID-19 vaccine and participate in check-in text messages with the Centers for Disease Control and Prevention (CDC) by the end of 2020.
In its COVID-19 vaccine testing, Novavax, a late-state biotechnology company, suggests that “an adjuvant is critical to its vaccine working well,” National Public Radio (NPR) reported in “The Special Sauce That Makes Some Vaccines Work.” However, vaccine developers may be reluctant to share their adjuvant research.
“Adjuvants end up being very proprietary. It’s kind of the secret sauce on how to make your protein vaccine work,” Barney Graham, MD, PhD, Deputy Director, Vaccine Research Center, National Institute of Allergy and Infectious Diseases, told NPR.
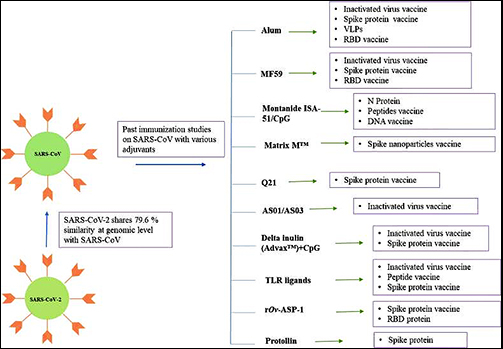
Still, a study published in Immunopharmacology revealed potential adjuvants for the COVID-19 vaccine based on vaccine studies of other coronaviruses. While there are many adjuvants available, not all have safety track records that can be leveraged to gain clearance from regulatory bodies, the researchers pointed out. But some do.
“CpG 1018, MF59, and AS03 are already approved for human vaccine and their inclusion may expedite the vaccine development process. Further, Protollin has shown promising results in pre-clinical studies,” the authors wrote.
Clinical laboratories that provide influenza testing will want to follow these types of research studies. Findings on immunity will affect development of vaccines that medical labs provide—including for COVID-19.