Researchers found evidence indicating that the virus has—under selection pressure—made itself more stable, giving it a “significant boost in infectivity”
While the COVID-19 pandemic continues to spread across the United States and throughout the world, new research suggests that a coming genetic mutation within the SARS-CoV-2 coronavirus may make it much more dangerous than it already is. This finding has significant implications for clinical laboratories that perform COVID-19 testing and the in vitro diagnostics (IVD) companies that develop and manufacture tests for COVID-19.
The mutation, called D614G, will provide the coronavirus with sturdier spikes that will increase its ability to latch onto and infect cells. That’s according to a study conducted at The Scripps Research Institute (Scripps) in Jupiter, Fla., which found that a mutated coronavirus may be up to 10 times more infectious than the original strain.
“Viruses with this mutation were much more infectious than those without the mutation in the cell culture system we used,” said Hyeryun Choe, PhD, Professor, Department of Immunology and Microbiology, Scripps Research, and senior author of the study, in a Scripps news release.
A More Flexible and Potent Coronavirus May Be Coming
The researchers found that coronavirus particles containing the mutation tend to have four to five times more functional spikes than particles without the mutation. The spikes enable the virus to bind to cells more easily. The research suggests that the greater the number of functional spikes on the viral surface the greater the flexibility and potency of the coronavirus.
In the Scripps news release, Farzan said, “more flexible spikes allow newly made viral particles to navigate the journey from producer cell to target cell fully intact, with less tendency to fall apart prematurely.
“Over time, it has figured out how to hold on better and not fall apart until it needs to,” he added. “The virus has, under selection pressure, made itself more stable.”
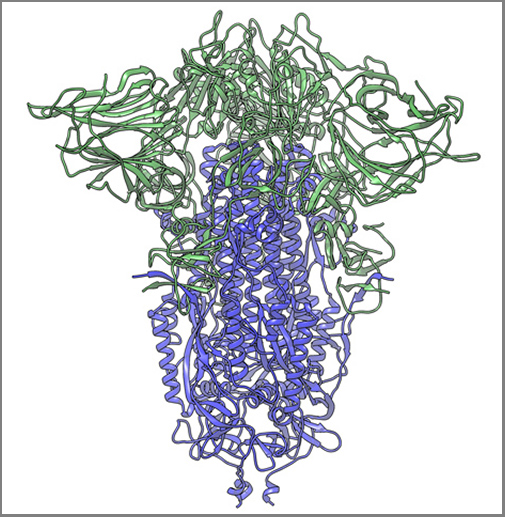
The image above, taken from the Scripps Research news release, shows “a cryogenic electron microscope image of a SARS-CoV-2 spike protein side view, the S1 section of the spike is shown in green and the S2 portion is shown in purple. This unique two-piece system has shown itself to be relatively unstable. A new mutation has appeared in the viral variant most common in New York and Italy that makes this spike both more stable and better able to infect cells.” (Graphic and caption copyright: Andrew Ward lab, Scripps Research.)
Mutation Makes SARS-CoV-2 Coronavirus ‘Much More Stable’
The two Scripps scientists have studied coronaviruses for nearly 20 years and performed extensive research on the Severe Acute Respiratory Syndrome (SARS) outbreak that occurred in 2003. They noted that there is a difference between spike proteins of SARS, an earlier strain of coronavirus, and the new SARS-CoV-2 strain.
The protein spikes of both strains were originally tripod shaped. However, the spikes of the SARS-CoV-2 coronavirus are divided into two different segments: S1 and S2. According to the published study: “The S1domain mediates receptor binding, and the S2 mediates downstream membrane fusion.”
This feature originally produced unstable spikes, but with the D614G mutation, the tripod breaks less frequently, which makes more of the spikes fully functional and the virus more infectious.
“Our data are very clear, the virus becomes much more stable with the mutation,” Choe said in the news release.
Is COVID-19 Spread Due to ‘Founder Effect’
The scientists also examined whether the spread of COVID-19 could have been the result of the “Founder Effect,” which is seen when a small number of variants fan out into a wide population by chance. Could the founder effect explain why COVID-19 outbreaks in some areas of the world were more severe than others? The researchers believe their data definitively answered that question.
“There have been at least a dozen scientific papers talking about the predominance of this mutation,” Farzan said. “Are we just seeing a founder effect? Our data nails it. It is not the founder effect.”
Hyeryun Choe, PhD (left), and Michael Farzan, PhD (right), scientists at Scripps Research explained that their research was performed using engineered viruses and that their observations of the virus and its mutation may not translate to increased transmissibility when a virus attaches to a host outside the lab. COVID-19 and its mutation appear to be relatively stable and are mutating at a rate slower than that of the seasonal flu, which may be critical factors in the development of a vaccine. (Photos copyright: Scripps Research.)
Findings Raise ‘Interesting’ Questions about the COVID-19 Coronavirus
Nevertheless, the two scientists are curious about some of their findings. “Our data raise interesting questions about the natural history of SARS-CoV-2 as it moved presumably from horseshoe bats to humans. At some point in this process, the virus acquired a furin-cleavage site, allowing its S1/S2 boundary to be cleaved in virus-producing cells. In contrast, the S1/S2 boundary of SARS-CoV-1, and indeed all SARS-like viruses isolated from bats, lack this polybasic site and are cleaved by TMPRSS2 or endosomalcathepsins in the target cells.
“In summary, we show that an S protein mutation that results in more transmissible SARS-CoV-2 also limits shedding of the S1 domain and increases S-protein incorporation into the virion. Further studies will be necessary to determine the impact of this change on the nature and severity of COVID-19,” the Scripps researchers concluded.
However, not all Scripps researchers agreed with the conclusions of Choe and Farzan’s research.
The Times of Israel reported that Kristian Andersen, PhD, a professor in the Department of Immunology and Microbiology, Scripps California Campus, told the New York Times that “other analyses of virus variants in labs had not found significant differences in infection rates.”
“That’s the main reason that I’m so hesitant at the moment,” Andersen said. “Because if one really was able to spread significantly better than the other, then we would expect to see a difference here, and we don’t.”
Times of Israel also reported that “In late May researchers in University College London said their studies of the genomes of more than 15,000 samples had not shown one strain being more infectious than others.”
So, the jury’s out. Nonetheless, clinical laboratory leaders will want to remain vigilant. A sudden increase in COVID-19 infection rates will put severe strain on already strained laboratory supply chains.
Genomics experts say this is a sign that clinical laboratory genetics testing is maturing into a powerful tool for population health
Faced with lagging sales and employee layoffs, genomics companies in the genealogy DNA testing market are shifting their focus to the healthcare aspects of the consumer genomics data they’ve compiled and aggregated.
Recent analysis of the sales of genetic tests from Ancestry and 23andMe show the market is definitely cooling, and the analysts speculate that—independent of the consequences of the COVID-19 pandemic on consumer behavior—the two clinical laboratory genetic testing companies may already have done testing for the majority of consumers who want to buy these tests.
“I think the consumer market is going to become more integrated into the healthcare experience,” Joe Grzymski, PhD, told GenomeWeb. “Whether that occurs through your primary care doctor, your large integrated health network, or your payor, I think there will be profound changes in society’s tolerance for using genetics for prevention.”
In February, Ancestry, the largest company in the home DNA testing space, announced it was laying off 6% of its workforce or approximately 100 people, across different departments due to a decline in sales, CNBC reported. Several weeks earlier, 23andMe, the second largest company in this market, also announced it was laying off about 100 people or 14% of its workforce due to declining sales.
“I wasn’t surprised by the news,” said Linda Avey, a 23andMe co-founder who is now co-founder and Chief Executive Officer at Precisely Inc., a genomics company headquartered in San Francisco. She was commenting to GenomeWeb on the recent restructuring at her former company. “The level of expensive advertising has been insane here in the US. Those [customer acquisition costs] are not a sustainable model.”
CNBC surmised that the lull in at-home genetic testing is due mainly to:
A drought of early adopters. Individuals who were interested in the testing for genealogical and health reasons, and who believed in the value of the tests, have already purchased the product.
Privacy concerns. Some potential customers may have reservations about having their DNA information collected and stored in a database due to concerns about how that data is safeguarded and its potential uses by outside companies, law enforcement, and governments.
COVID-19 May or May Not Be a Factor in Declining DNA Testing Sales
The COVID-19 pandemic may be playing a role in the decline in sales of at-home DNA testing kits. However, there are indications that the market was cooling before the virus occurred.
An article in MIT Technology Review reported that 26 million people had purchased at-home DNA testing kits by the beginning of 2019. The article also estimated that if the market continued at that pace, 100 million people were expected to purchase the tests by the end of 2020.
However, data released by research firm Second Measure, a company that analyzes credit and debit card purchases, may show a different story, reported Vox. The data showed a general decline in test kit sales in 2019. Ancestry’s sales were down 38% and 23andMe’s sales were down 54% in November 2019 compared to November 2018. The downward trend continued in December with Ancestry sales declining 15% and 23andMe sales declining 48% when compared to December 2018.
Second Measure, however, compiled data from the two companies’ websites only. They did not include testing kits that may have been purchased through other sources such as Amazon, or at brick and mortar locations.
Nevertheless, the measures being taken by genomics companies to shore up their market indicates the Second Measure data is accurate or very close.
Rise of Population-level Genomics
This decline in genealogical sales seems to be behind DNA-testing companies shifting focus to the healthcare aspects of consumer genomics. Companies like 23andMe and Ancestry are looking into developing health reports based on their customers’ data that can ascertain an individual’s risk for certain health conditions, or how they may react to prescription medications.
“We are seeing the next wave of maturity of the genetics market,” Othman Laraki, co-founder and CEO of Color Genomics, told CNBC. “If expensive diagnostic testing was genomics’ equivalent of mainframe computers, direct to consumer ancestry genetics was the hobbyist use. While the early adopter wave is petering out, we are seeing the real market (the equivalent of a PC in every home and a phone in every pocket), which is population-level use of genetics, taking hold.” (Photo copyright: San Francisco Business Times.)
For some genomics companies like 23andMe, the at-home DNA testing market was never specifically about selling testing kits. Rather, these companies envisioned a market where consumers would pay to have their DNA analyzed to obtain data on their ancestry and health, and in turn the testing companies would sell the aggregated consumer data to other organizations, such as pharmaceutical companies.
“Remember that 23andMe was never in the consumer genomics business, they were in the data aggregation business,” Spencer Wells, PhD, founder and Executive Director of the Insitome Institute, a US-based 501(c)3 nonprofit think tank focused on key areas in the field of personal genomics, told GenomeWeb. “They created a database that should in principle allow them to do what they promised, which is to improve people’s health through genomic testing.”
Even with clinical laboratory testing currently focused on COVID-19 testing, there remains an opportunity to sequence large numbers of people through at-home DNA testing and then incorporate those findings into the practice of medicine. The hope is that sales will again accelerate once consumers feel there is a compelling need for the tests.
Pathologists and clinical laboratory managers will want to watch to see if the companies that grew big by selling ancestry and genealogy tests to consumers will start to send sales reps into physicians’ offices to offer genetic tests that would be useful in diagnosing and treating patients.
In the absence of a “gold standard,” researchers are finding a high frequency of false negatives among SARS-CoV-2 RT-PCR tests
Serology tests designed to detect antibodies to the SARS-CoV-2 coronavirus that causes the COVID-19 illness have been dogged by well-publicized questions about accuracy. However, researchers also are raising concerns about the accuracy of molecular diagnostics which claim to detect the actual presence of the coronavirus itself.
“Diagnostic tests, typically involving a nasopharyngeal swab, can be inaccurate in two ways,” said Steven Woloshin, MD, MS, in a news release announcing a new report that “examines challenges and implications of false-negative COVID-19 tests.” Woloshin is an internist, a professor at Dartmouth Institute, and co-director of the Geisel School of Medicine at Dartmouth.
“A false-positive result mistakenly labels a person infected, with consequences including unnecessary quarantine and contact tracing,” he stated in the news release. “False-negative results are far more consequential, because infected persons who might be asymptomatic may not be isolated and can infect others.”
Woloshin led a team of Dartmouth researchers who analyzed two studies from Wuhan, China, and a literature review by researchers in Europe and South America that indicated diagnostic tests for COVID-19 are frequently generating false negatives. The team published their results in the June 5 New England Journal of Medicine (NEJM).
For example, one research team in Wuhan collected samples from 213 hospitalized COVID-19 patients and found that an approved RT-PCR test produced false negatives in 11% of sputum samples, 27% of nasal samples, and 40% of throat samples. Their research was published on the medRxiv preprint server and has not been peer-reviewed.
The literature review Woloshin’s team studied was also published on medRxiv, titled, “False-Negative Results of Initial Rt-PCR Assays for COVID-19: A Systematic Review.” It indicated that the rate of false negatives could be as high as 29%. The authors of the review looked at five studies that had enrolled a total of 957 patients. “The collected evidence has several limitations, including risk of bias issues, high heterogeneity, and concerns about its applicability,” they wrote. “Nonetheless, our findings reinforce the need for repeated testing in patients with suspicion of SARS-Cov-2 infection.”
Another literature review, published in the Annals of Internal Medicine, titled, “Variation in False-Negative Rate of Reverse Transcriptase Polymerase Chain Reaction–Based SARS-CoV-2 Tests by Time Since Exposure,” estimated the probability of false negatives in RT-PCR tests at varying intervals from the time of exposure and symptom onset. For example, the authors found that the median false-negative rate was 38% if a test was performed on the day of symptom onset, versus 20% three days after onset. Their analysis was based on seven studies, five of which were peer-reviewed, with a total of 1330 test samples.
Doctors also are seeing anecdotal evidence of false negatives. For example, clinicians at UC San Diego Health medical center treated a patient with obvious symptoms of COVID-19, but two tests performed on throat samples were negative. However, a third test, using a sample from a bronchial wash, identified the virus, reported Medscape.
Sensitivity and Specificity of COVID-19 Clinical Laboratory Tests
The key measures of test accuracy are sensitivity, which refers to the ability to detect the presence of the virus, and specificity, the ability to determine that the targeted pathogen is not present. “So, a sensitive test is less likely to provide a false-negative result and a specific test is less likely to provide a false-positive result,” wrote Kirsten Meek, PhD, medical writer and editor, in an article for ARUP Laboratories.
“Analytic” sensitivity and specificity “represent the accuracy of a test under ideal conditions in which specimens have been collected from patients with either high viral loads or a complete absence of exposure,” she wrote. However, “sensitivity and specificity under real-world conditions, in which patients are more variable and specimen collection may not be ideal, can often be lower than reported numbers.”
In a statement defending its ID Now molecular point-of-care test, which came under scrutiny during a study of COVID-19 molecular tests by NYU Langone Health, Northwell Health, and Cleveland Clinic, according to MedTech Dive, Abbott Laboratories blamed improper sample collection and handling for highly-publicized false negatives produced by its rapid test. An FDA issued alert about the test on May 14 noted that Abbott had agreed to conduct post-market studies to identify the cause of the false negatives and suggest remedial actions.
Issues with Emergency Use Authorizations
In their NEJM analysis, Woloshin et al point to issues with the FDA’s process for issuing Emergency Use Authorizations (EUAs). For example, they noted variations in how manufacturers are conducting clinical evaluations to determine test performance. “The FDA prefers the use of ‘natural clinical specimens’ but has permitted the use of ‘contrived specimens’ produced by adding viral RNA or inactivated virus to leftover clinical material,” they wrote.
When evaluating clinical performance, manufacturers ordinarily conduct an index test of patients and compare the results with reference-standard test, according to the Dartmouth researchers. For people showing symptoms, the reference standard should be a clinical diagnosis performed by an independent adjudication panel. However, they wrote, “it is unclear whether the sensitivity of any FDA-authorized commercial test has been assessed in this way.” Additionally, a reference standard for determining sensitivity in asymptomatic people “is an unsolved problem that needs urgent attention to increase confidence in test results for contact-tracing or screening purposes.”
“To truly determine false negatives, you need a gold standard test, which is essentially as close to perfect as we can get,” Stephen Rawlings, MD, PhD, (above), a resident physician of internal medicine and infectious diseases fellow at UC San Diego’s Center for AIDS Research (CFAR), who has been working on SARS-CoV-2 test validation since March. “But there just isn’t one yet for coronavirus,” he told Medscape. (Photo copyright: University of California, San Diego.)
Continued adherence to current measures, such as physical distancing and surface disinfection.
Development of highly sensitive and specific tests or combinations of tests to minimize the risk of false-negative results and ongoing transmission based on a false sense of security.
Improved RT-PCR tests and serological assays.
Development and communication of clear risk-stratified protocols for management of negative COVID-19 test results.
“These protocols must evolve as diagnostic test, transmission, and outcome statistics become more available,” they wrote.
Meanwhile, clinical laboratories remain somewhat on their own at selecting which COVID-19 molecular and serology tests they want to purchase and run in their labs. Complicating such decisions is the fact that many of the nation’s most reputable in vitro diagnostics manufacturers cannot produce enough of their COVID-19 tests to meet demand.
Consequently, when looking to purchase tests for SARS-CoV-2, smaller medical laboratory organizations find themselves evaluating COVID-19 kits developed by little-known or even brand-new companies.
Medical laboratories are already using gene sequencing as part of a global effort to identify new variants of the coronavirus and their genetic ancestors
Thanks to advances in genetic sequencing technology that enable medical laboratories to sequence organisms faster, more accurately, and at lower cost than ever before, clinical pathology laboratories worldwide are using that capability to analyze the SARS-CoV-2 coronavirus and identify variants as they emerge in different parts of the world.
The US Centers for Disease Control and Prevention (CDC) now plans to harness the power of gene sequencing through a new consortium called SPHERES (SARS-CoV-2 Sequencing for Public Health Emergency Response, Epidemiology, and Surveillance) to “coordinate SARS-CoV-2 sequencing across the United States,” states a CDC news release. The consortium is led by the CDC’s Advanced Molecular Detection (AMD) program and “aims to generate information about the virus that will strengthen COVID-19 mitigation strategies.”
The consortium is comprised of 11 federal agencies, 20 academic institutions, state public health laboratories in 21 states, nine non-profit research organizations, and 14 lab and IVD companies, including:
Abbott Diagnostics
bioMérieux
Color Genomics
Ginkgo Bioworks
IDbyDNA
Illumina
In-Q-Tel
LabCorp
One Codex
Oxford Nanopore Technologies
Pacific Biosciences
Qiagen
Quest Diagnostics
Verily Life Sciences
‘Fundamentally Changing How Public Health Responds’
Gene sequencing and related technologies have “fundamentally changed how public health responds in terms of surveillance and outbreak response,” said Duncan MacCannell, PhD, Chief Science Officer for the CDC’s Office of Advanced Molecular Detection (OAMD), in an April 30 New York Times (NYT) article, which stated that the CDC SPHERES program “will help trace patterns of transmission, investigate outbreaks, and map how the virus is evolving, which can affect a cure.”
The CDC says that rapid DNA sequencing of SARS-CoV-2 will help monitor significant changes in the virus, support contact tracing efforts, provide information for developers of diagnostics and therapies, and “advance public health research in the areas of transmission dynamics, host response, and evolution of the virus.”
The sequencing laboratories in the consortium have agreed to “release their information into the public domain quickly and in a standard way,” the NYT reported, adding that the project includes standards for what types of information medical laboratories should submit, including, “where and when a sample was taken,” and other critical details.
Even in its early phase, the CDC’s SPHERES project has “made a tangible impact in the number of sequences we’re able to deposit and make publicly available on a daily basis,” said Pavitra Roychoudhury, PhD (above), Acting Instructor and Senior Fellow at the University of Washington, and Research Associate at Fred Hutchinson Cancer Research Center, in an e-mail to the NYT. “What we’re essentially doing is reading these small fragments of viral material and trying to jigsaw puzzle the genome together,” said Roychoudhury in an April 28 New York Times article which covered in detail how experts are tracking the coronavirus since it arrived in the US. (Photo copyright: LinkedIn.)
Sharing Data Between Sequencing Laboratories and Biotech Companies
The CDC announced the SPHERES initiative on April 30, although it launched in early April, the NYT reported.
According to the CDC, SPHERES’ objectives include:
To bring together a network of sequencing laboratories, bioinformatics capacity and subject matter expertise under the umbrella of a massive and coordinated public health sequencing effort.
To identify and prioritize capabilities and resource needs across the network and to align sources of federal, non-governmental, and private sector funding and support with areas of greatest impact and need.
To improve coordination of genomic sequencing between institutions and jurisdictions and to enable more resilience across the network.
To champion concepts of openness, standards-based analysis, and rapid data sharing throughout the United States and worldwide during the COVID-19 pandemic response.
To provide a common forum for US public, private, and academic institutions to share protocols, methods, bioinformatics tools, standards, and best practices.
To establish consistent data and metadata standards, including streamlined repository submission processes, sample prioritization criteria, and a framework for shared, privacy-compliant unique case identifiers.
To align with other national sequencing and bioinformatics networks, and to support global efforts to advance the use of standards and open data in public health.
Implications for Developing a Vaccine
As the virus continues to mutate and evolve, one question is whether a vaccine developed for one variant will work on others. However, several experts told The Washington Post that the SARS-CoV-2 coronavirus is relatively stable compared to viruses that cause seasonal flu (influenza).
“At this point, the mutation rate of the virus would suggest that the vaccine developed for SARS-CoV-2 would be a single vaccine, rather than a new vaccine every year like the flu vaccine,” Peter Thielen, a molecular biologist at the Johns Hopkins University Applied Physics Laboratory, told the Washington Post.
Nor, he said, is one variant likely to cause worse clinical outcomes than others. “So far, we don’t have any evidence linking a specific virus [strain] to any disease severity score. Right now, disease severity is much more likely to be driven by other factors.”
Fast improvements in gene sequencing technology have made it faster, more accurate, and cheaper to sequence. Thus, as the COVID-19 outbreak happened, there were many clinical laboratories around the world with the equipment, the staff, and the expertise to sequence the novel coronavirus and watch it mutate from generation to generation and from region to region around the globe. This capability has never been available in outbreaks prior to the current SARS-CoV-2 outbreak.
Two major clinical laboratory conferences reschedule, as the SARS-CoV-2 pandemic continues to disrupt long-planned events; Many labs are losing money as fewer patients visit physicians
This week, the ongoing Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) pandemic was responsible for two important developments in the clinical laboratory industry. Both involved the rescheduling of major annual conferences. In both cases, conference organizers are placing different bets on when they think the COVID-19 outbreak, the illness caused by the SARS-CoV-2 coronavirus, will have passed and when they believe some semblance of normalcy will return to both social interaction and business activities.
On Monday, the American Association of Clinical Chemistry (AACC) announced that it would reschedule its 2020 AACC annual meeting and exhibition—originally scheduled for July 26-30, 2020, at McCormick Place in Chicago—to Dec. 13-17, 2020, also at McCormick Place.
On the same day, Dark Daily’s sister publication, The Dark Report, announced it had rescheduled the 25th annual Executive War College on Laboratory and Pathology Management to new dates and to a new hotel. This conference will now take place on July 14-15, 2020, at the Hyatt Regency Hotel in New Orleans. This is a change from the originally scheduled date of April 28-29, 2020, and from the original location, the Sheraton New Orleans Hotel.
On its website, AACC stated: “Based on input from all stakeholder groups, and in close collaboration with host city officials, the organization is pleased to announce that AACC will be able to preserve the complete Annual Scientific Meeting and Clinical Lab Expo experience to which its members, exhibitors, and the entire laboratory medicine community have been looking forward. The 2020 AACC Annual Scientific Meeting and Clinical Lab Expo will now be held December 13-17, 2020, at McCormick Place in Chicago, IL, USA.”
Each conference claims to be “the largest” in some
dimension. Each year, AACC’s annual conference attracts more than 20,000
attendees, as measured by clinical chemists and other visitors to its Expo,
which features more than 750 lab companies.
While the Executive War College claims to be the largest conference serving the business, management, operations, and financial health needs of clinical laboratories and pathology groups. Each year, it hosts almost 900 attendees—generally senior administrators, lab executives, pathologist-business leaders, consultants, and in vitro diagnostics (IVD) manufacturers. The conference is supported by more than 50 corporate benefactors and sponsors.
AACC’s rescheduling of its conference from July to December
will delay two important activities:
Many lab scientists planning to attend were hoping to participate in the first assessments of the novel coronavirus pandemic, assuming that the pandemic had passed by mid-summer.
During AACC is when the nation’s major IVD manufacturers and companies that sell lab automation, instruments, test kits, reagents, and other products introduce their latest-generation solutions. Now, many of those product launches will be pushed back to December.
Meanwhile, organizers of the Executive War College are betting that the novel coronavirus pandemic will taper down, possibly synchronized with the end of the annual influenza season in North America, which is typically sometime in April or early May.
If this proves true, then conducting the conference on July 14-15, 2020, will give lab leaders the opportunity to gather and share lessons learned during this COVID-19 outbreak in time to prepare for a possible second outbreak of COVID-19 when the next influenza season arrives in the fall. It will also be an important opportunity for lab managers and pathologists to learn ways to restore revenue lost during the pandemic.
Clinical Laboratories, Pathology Groups, Hospitals, at
Brink of Financial Ruin
“What has gone unrecognized by the national news media is how the novel coronavirus pandemic is causing financial devastation to the finances of the nation’s clinical laboratories and anatomic pathology groups,” stated Robert L. Michel, Editor-in-Chief of The Dark Report and Founder of the Executive War College. “In absolute terms, the pandemic is a growing financial disaster to the medical lab industry, and it will take years for many labs to rebuild the staff that they have laid off or terminated in recent months in order to stay operational.
“Why are all labs losing money at this time?” asked Michel.
“The answer is simple—beginning early in March, patients stopped visiting their
doctors. Hospitals ceased to admit patients for elective procedures. Fewer
patients per day means fewer lab test referrals per day and loss of the revenue
generated by those claims that pays the salaries and expenses of the labs
performing those tests. Laying off or furloughing staff is one way labs lower
costs in response to lower income.
“Many clinical labs, pathology groups, and the hospitals
they serve are steadily approaching financial ruin,” he continued. “Every week
the pandemic continues, and North American citizens are advised to shelter in
place, forces labs to draw down their dwindling financial reserves to keep
their doors open.”
Robert Michel (above), Editor-in-Chief of The Dark Report and Dark Daily and Founder of The Dark Intelligence Group, will host the 25th anniversary Executive War College on Lab and Pathology Management on July 14-15, 2020, in New Orleans. Attendees from clinical laboratories and pathology groups will gain critical insights from such learning opportunities as: “Preparing Your Lab for a Second Outbreak of COVID-19,” and “Rapidly Building Cash Flow and Restoring Your Lab’s Financial Stability Post-Pandemic.” (Photo copyright: The Dark Report.)
This crisis has created three big questions that labs need
to answer:
How much longer will the COVID-19 pandemic last
before some degree of normalcy is restored (meaning patient office visits resume
and physicians begin ordering lab tests every day)?
If there is a second outbreak of SARS-CoV-2 this
fall, what does every lab need to know to be ready?
As American society and business return to
normal, how can labs quickly build up cash flow, collect more revenue, and
restore financial stability?
“Given the unknown aspects of the SARS-CoV-2 coronavirus,
the answer to the first question is a crap-shoot. But to reschedule the
Executive War College to dates that are 14 weeks away seems a reasonable bet,”
noted Michel. “The pay-off to that bet is the ability to provide the owners and
leaders of the nation’s labs answers to the second and third questions.
“The 14 weeks between now and mid-July give us the
opportunity to organize sessions and invite speakers who can provide answers
and information to help labs with their two most pressing needs: to be prepared
for another COVID-19 outbreak later this year, and to restore cash flow and
financial health as soon as possible,” said Michel. “This will be the very
first opportunity for lab managers and pathologists to assemble, learn the
COVID-19 lessons from successful labs, gain financial insights, and network
with their peers.”
The Executive War College team is inviting suggestions for
speakers and session topics for the July 14-15 conference. The original agenda
that was taking shape for the planned dates of April 28-29 will be revised so
as to include presentations now directly relevant to the state of the clinical
lab and pathology professions for mid-year 2020. Send your suggestions for
topics and speakers to info@darkreport.com.
Information on registering for the 25th annual Executive War College, and on placing reservations at the Hyatt Regency Hotel in New Orleans, is available on the EWC website (or copy and paste this URL in your browser: https://www.executivewarcollege.com.)
People already registered for Executive War College 2020
will have their registrations automatically applied to the new July 14-15
dates.
Scientist described the speed at which SARS-CoV-2’s full sequence of genetic material was made public as ‘unprecedented’ and medical labs are rushing to validate tests for this new disease
In the United States, headlines scream about the lack of
testing for the novel Coronavirus
disease 2019 (COVID-19). News reporters ask daily why it is taking so long
for the US healthcare system to begin testing large numbers of patients for
SARS-CoV-2, the virus that causes COVID-19. Yet, pathologists
and clinical
laboratory scientists know that new technologies for gene sequencing
and diagnostic testing are helping public health laboratories bring up tests
for a previously unknown new disease faster than at any time in the past.
At the center of the effort to develop accurate new assays
to detect SARS-CoV-2 and help diagnose cases of the COVID-19 disease are medical laboratory
scientists working in public health
laboratories, in academic medical centers, and in research labs across the
United States. Their collective efforts are producing results on a faster
timeline than in any previous discovery of a new infectious disease.
For example, during the severe
acute respiratory syndrome (SARS) outbreak in 2003, five months passed
between the first recognized case of the disease in China and when a team of
Canadian scientists cracked the genetic code of the virus, which was needed to
definitively diagnose SARS patients, ABC
News reported.
In contrast, Chinese scientists sequenced this year’s
coronavirus (originally named 2019-nCoV) and made it available on Jan. 10,
2020, just weeks after public health officials in Wuhan, China, reported the
first case of pneumonia from the unknown virus to the World Health Organization
(WHO), STAT
reported.
Increases in sequencing speed enabled biotechnology
companies to quickly create synthetic copies of the virus needed for research. Roughly
two weeks later, scientists completed sequencing nearly two dozen more samples
from different patients diagnosed with COVID-19.
Molecular biologist Kristian Andersen, PhD (above right, with graduate students who helped sequence the Zika virus), an Associate Professor in the Department of Immunology and Microbiology at Scripps Research in California and Director of Infectious Disease Genomics at Scripps’ Translational Research Institute, worked on the team that sequenced the Ebola genome during the 2014 outbreak. He told STAT that the pace of sequencing of the SARS-CoV-2 coronavirus is “unprecedented.” (Photo copyright: Scripps Research.)
Lower Sequencing Costs Speed COVID-19 Diagnostics Research
Additionally, a significant decline in the cost of genetic synthesis is playing an equally important role in helping scientists slow the spread of COVID-19.In its coverage of the SARS-CoV-2 outbreak, The Verge noted that two decades ago “it cost $10 to create a synthetic copy of one single nucleotide, the building block of genetic material. Now, it’s under 10 cents.” Since the coronavirus gene is about 30,000 nucleotides long, that price reduction is significant.
Faster sequencing and cheaper access to synthetic copies is
contributing to the development of diagnostic tests for COVID-19, an important
step in slowing the disease.
“This continues to be an evolving situation and the ability to distribute this diagnostic test to qualified medical laboratories is a critical step forward in protecting the public health,” FDA Commissioner Stephen M. Hahn, MD, said in an FDA statement.
However, the Washington Post soon reported that the government-created coronavirus test kits contained a “faulty component,” which as of February 25 had limited testing in the US to only 426 people, not including passengers who returned to the US on evacuation flights. The Post noted that the nation’s public health laboratories took “the unusual step of appealing to the FDA for permission to develop and use their own [laboratory-developed] tests” for the coronavirus.
“This is an extraordinary request, but this is an extraordinary time,” Scott Becker,
Parallel efforts to develop and validate tests for COVID-19
are happening at the clinical laboratories of academic medical centers and in a
number of commercial laboratory companies. As these labs show their tests meet
FDA criteria, they become available for use by physicians and other healthcare
providers.
Dark Daily’s sister publication, The Dark Report just published an intelligence briefing about the urgent effort at the clinical laboratory of Northwell Health to develop both a manual COVID-19 assay and a test that can be run on the automated analyzers already in use in the labs at Northwell Health’s 23 hospitals. (See TDR, “Northwell Lab Team Validates COVID-19 Test on Fast Timeline,” March 9, 2020.)
Following the FDA’s March 13 EUA for the Thermo Fisher test,
Hahn said, “We have been engaging with test developers and encouraging them to
come to the FDA and work with us. Since the beginning of this outbreak, more
than 80 test developers have sought our assistance with development and
validation of tests they plan to bring through the Emergency Use Authorization
process. Additionally,” he continued, “more than 30 laboratories have notified
us they are testing or intend to begin testing soon under our new policy for
laboratory-developed tests for this emergency. The number of products in the
pipeline reflects the significant role diagnostics play in this outbreak and
the large number of organizations we are working with to bring tests to
market.”
Pharma Company Uses Sequencing Data to Develop Vaccine in
Record Time
Even as clinical laboratories work to develop and validate diagnostic tests for COVID-19, drug manufacturers are moving rapidly to develop a COVID-19 vaccine. In February, Massachusetts-based biotechnology company Moderna Therapeutics (NASDAQ:MRNA) announced it had shipped the first vials of its potential coronavirus vaccine (mRNA-1273) to the National Institute of Allergy and Infectious Disease (NIAID) for use in a Phase One clinical trial.
“The collaboration across Moderna, with NIAID, and with CEPI [Coalition for Epidemic Preparedness Innovations] has allowed us to deliver a clinical batch in 42 days from sequence identification,” Juan Andres, Chief Technical Operations and Quality Officer at Moderna, stated in a news release.
The Wall Street Journal (WSJ) reported that NIAID expects to start a clinical trial of about 20 to 25 healthy volunteers by the end of April, with results available as early as July or August.
“Going into a Phase One trial within three months of getting the sequence is unquestionably the world indoor record,” NIAID Director Anthony Fauci, MD, told the WSJ. “Nothing has ever gone that fast.”
There are no guarantees that Moderna’s coronavirus vaccine
will work. Furthermore, it will require further studies and regulatory
clearances that could delay widespread distribution until next year.
Nonetheless, Fauci told the WSJ, “The only way you
can completely suppress an emerging infectious disease is with a vaccine. If
you want to really get it quickly, you’re using technologies that are not as
time-honored as the standard, what I call antiquated, way of doing it.”
In many ways, the news media has overlooked all the important
differences in how fast useful diagnostic and therapeutic solutions for
COVID-19 are moving from research settings into clinical use, when compared to
early episodes of the emergence of a new infectious disease, such as SARS in
2003.
The story the American public has yet to learn is how new
genetic sequencing technologies, improved diagnostic methods, and enhanced
informatics capabilities are being used by researchers, pathologists, and
clinical laboratory professionals to understand this new disease and give
healthcare professionals the tools they need to diagnose, treat, and monitor
patients with COVID-19.