Pathologists and clinical laboratory scientists may find one hospital’s use of a machine-learning platform to help improve utilization of lab tests both an opportunity and a threat
Variation in how individual physicians order, interpret, and act upon clinical laboratory test results is regularly shown by studies in peer-reviewed medical journals to be one reason why some patients get great outcomes and other patients get less-than-desirable outcomes. That is why many healthcare providers are initiating efforts to improve how physicians utilize clinical laboratory tests and other diagnostic procedures.
This effort came about after clinical and administrative leadership at Flagler Hospital realized that only about one-third of its physicians regularly followed certain medical decision-making guidelines or clinical order sets. Armed with these insights, staff members decided to find a solution that reduced or removed variability from their healthcare delivery.
Reducing Variability Improves Care, Lowers Cost
Variability in physician care has been linked to increased healthcare costs and lower quality outcomes, as studies published in JAMA and JAMA Internal Medicine indicate. Such results do not bode well for healthcare providers in today’s value-based reimbursement system, which rewards increased performance and lowered costs.
Clinical order sets are designed to be used as part of clinical decision support systems (CDSS) installed by hospitals for physicians to standardize care and support sound clinical decision making and patient safety.
However, when doctors don’t adhere to those pre-defined standards, the results can be disadvantageous, ranging from unnecessary services and tests being performed to preventable complications for patients, which may increase treatment costs.
“Over the past few decades we’ve come to realize clinical variation plays an important part in the overuse of medical care and the waste that occurs in healthcare, making it more expensive than it should be,” Michael Sanders, MD (above) Flagler’s Chief Medical Information Officer, told Modern Healthcare. “Every time we’re adding something that adds cost, we have to make sure that we’re adding value.” (Photo copyright: Modern Healthcare.)
Flagler’s AI project involved uploading clinical,
demographic, billing, and surgical information to the AyasdiAI platform, which then
employed machine learning to analyze the data and identify trends. Flagler’s
physicians are now provided with a fuller picture of their patients’ conditions,
which helps identify patients at highest risk, ensuring timely interventions that
produce positive outcomes and lower costs.
How Symphony AyasdiAI Works
The AyasdiAI application utilizes a category of mathematics called topological data analysis (TDA) to cluster similar patients together and locate parallels between those groups. “We then have the AI tools generate a carepath from this group, showing all events which should occur in the emergency department, at admission, and throughout the hospital stay,” Sanders told Healthcare IT News. “These events include all medications, diagnostic tests, vital signs, IVs, procedures and meals, and the ideal timing for the occurrence of each so as to replicate the results of this group.”
Caregivers then examine the data to determine the optimal
plan of care for each patient. Cost savings are figured into the overall
equation when choosing a treatment plan.
Flagler first used the AI program to examine trends among their pneumonia patients. They determined that nebulizer treatments should be started as soon as possible with pneumonia patients who also have chronic obstructive pulmonary disease (COPD).
“Once we have the data loaded, we use [an] unsupervised
learning AI algorithm to generate treatment groups,” Sanders told Healthcare
IT News. “In the case of our pneumonia patient data, Ayasdi produced nine
treatments groups. Each group was treated similarly, and statistics were given
to us to understand that group and how it differed from the other groups.”
Armed with this information, the hospital achieved an 80% greater physician adherence to order sets for pneumonia patients. This resulted in a savings of $1,350 per patient and reduced the readmission rates for pneumonia patients from 2.9% to 0.4%, reported Modern Healthcare.
The development of a machine-learning platform designed to
reduce variation in care (by helping physicians become more consistent at
following accepted clinical care guidelines) can be considered a warning shot
across the bow of the pathology profession.
This is a system that has the potential to become interposed
between the pathologist in the medical laboratory and the physicians who refer
specimens to the lab. Were that to happen, the deep experience and knowledge
that have long made pathologists the “doctor’s doctor” will be bypassed.
Physicians will stop making that first call to their pathologists, clinical
chemists, and laboratory scientists to discuss a patient’s condition and
consult on which test to order, how to interpret the results, and get guidance
on selecting therapies and monitoring the patient’s progress.
Instead, a “smart software solution” will be inserted into
the clinical workflow of physicians. This solution will automatically guide the
physician to follow the established care protocol. In turn, this will give the
medical laboratory the simple role of accepting a lab test order, performing
the analysis, and reporting the results.
If this were true, then it could be argued that a laboratory
test is a commodity and hospitals, physicians, and payers would argue that they
should buy these commodity lab tests at the cheapest price.
Many other healthcare systems also are partnering with private genetic testing companies to pursue research that drive precision medicine goals
It is certainly unusual when a major health network announces that it will give away free genetic tests to 10,000 of its patients as a way to lay the foundation to expand clinical services involving precision medicine. However, pathologists and clinical laboratory managers should consider this free genetic testing program to be the latest marketplace sign that acceptance of genetic medicine continues to move ahead.
Notably, it is community hospitals that are launching this
new program linked to clinical laboratory research that uses genetic tests for
specific, treatable conditions. The purpose of such genetic research is to
identify patients who would benefit from test results that identify the best
therapies for their specific conditions, a core goal of precision medicine.
Clinical laboratory leaders will be interested in this
initiative, as well other partnerships between healthcare systems and private
genetic testing companies aimed at identifying and enrolling patients in
research studies for disease treatment protocols and therapies.
The Future of Precision Medicine
Modern Healthcare reported that data from the WholeMe DNA study, which was funded through donations to the AdventHealth Foundation, also will be used by the healthcare network for research beyond FH, as AdventHealth develops its genomics services. The project’s cost is estimated to reach $2 million.
“Genomics is the future of medicine, and the field is rapidly evolving. As we began our internal discussions about genomics and how to best incorporate it at AdventHealth, we knew research would play a strong role,” Wes Walker MD, Director, Genomics and Personalized Health, and Associate CMIO at AdventHealth, told Becker’s Hospital Review.
“We decided to focus on familial hypercholesterolemia
screening initially because it’s a condition that is associated with
life-threatening cardiovascular events,” he continued. “FH is treatable once
identified and finding those who have the condition can lead to identifying
other family members who are subsequently identified who never knew they had
the disease.”
The AdventHealth Orlando website states that participants in the WholeMe study receive information stored in a confidential data repository that meets HIPAA security standards. The data covers ancestry and 22 other genetic traits, such as:
Asparagus Odor Detection
Bitter Taste
Caffeine Metabolism
Cilantro Taste Aversion
Circadian Rhythm
Coffee Consumption
Delayed Sleep
Earwax Type
Endurance vs Power
Exercise Impact on Weight
Eye Color
Freckling
Hair Curl and Texture
Hand Grip Strength
Height
Lactose Tolerance
Sleep Duration
Sleep Movement
Sleeplessness
Sweet Tooth
Tan vs. Sunburn
Waist Size
Those who test positive for a disease-causing FH variant will be referred by AdventHealth for medical laboratory blood testing, genetic counseling, and a cardiologist visit, reported the Ormond Beach Observer.
One in 250 people have FH, and 90% of them are undiagnosed,
according to the FH Foundation,
which also noted that children have a 50% chance of inheriting FH from parents
with the condition.
AdventHealth plans to expand the free testing beyond central
Florida to its 46 other hospitals located in nine states, Modern Healthcare
noted.
Other Genetics Data Company/Healthcare Provider Partnerships
Helix (above) is one of the world’s largest CLIA-certified, CAP-accredited next-generation sequencing labs. The partnership with AdventHealth offered study participants Exome+: a panel-grade medical exome enhanced by more than 300,000 informative non-coding regions; a co-branded ancestry + traits DNA product for all participants; secure storage of genomic data for the lifetime of the participant; infrastructure and data to facilitate research; and in-house clinical and scientific expertise, according to Helix’s website. (Photo copyright: Orlando Sentinel.)
Business Insider noted that Helix has focused on clinical partnerships for about a year and seems to be filling a niche in the genetic testing market.
“Helix is able to sidestep the costs of direct-to-consumer
marketing and clinical test development, while still expanding its customer
base through predefined hospital networks. And the company is in a prime
position to capitalize on providers’ interest in population health management,”
Business Insider reported.
Ochsner’s program is the first “fully digital population
health program” aimed at including clinical genomics data in primary care in an
effort to affect patients’ health, FierceHealthcare
reported.
Hereditary breast and ovarian cancer due to
mutations in BRCA1 and BRCA2 genes;
Lynch
syndrome, associated with colorectal and other cancers; and
FH.
Color also offers genetic testing and whole genome sequencing services to NorthShore’s DNA10K program, which plans to test 10,000 patients for risk for hereditary cancers and heart diseases, according to news release.
And, Jefferson Health offered Color’s genetic testing to the healthcare system’s 33,000 employees, 10,000 of which signed up to learn their health risks as well as ancestry, a Color blog post states.
“Understanding the genome warning signals of every patient will be an essential part of wellness planning and health management,” said Geisinger Chief Executive Officer David Feinberg, MD, when he announced the new initiative at the HLTH (Health) Conference in Las Vegas. “Geisinger patients will be able to work with their family physician to modify their lifestyle and minimize risks that may be revealed,” he explained. “This forecasting will allow us to provide truly anticipatory healthcare instead of the responsive sick care that has long been the industry default across the nation.”
It will be interesting to see how and if genetic tests—free
or otherwise—will advance precision medicine goals and population health
treatments. It’s important for medical laboratory leaders to be involved in health
network agreements with genetic testing companies. And clinical laboratories should
be informed whenever private companies share their test results data with
patients and primary care providers.
Researchers are discovering it’s possible to determine a person’s age based on the amount of protein in the blood, but the technology isn’t always correct
Mass spectrometry is increasingly finding its way into clinical laboratories and with it—proteomics—the study of proteins in the human body. And like the human genome, scientists are discovering that protein plays an integral part in the aging process.
This is a most interesting research finding. Might medical laboratories someday use proteomic biomarkers to help physicians gauge the aging progression in patients? Might this diagnostic capability give pathologists and laboratory leaders a new product line for direct-to-consumer testing that would be a cash-paying, fast-growing, profitable clinical laboratory testing service? If so, proteomics could be a boon to clinical laboratories worldwide.
When research into genomics was brand-new, virtually no one imagined that someday the direct-to-consumer lab testing model would offer genetic testing to the public and create a huge stream of revenue for clinical laboratories that process genetic tests. Now, research into protein and aging might point to a similar possibility for proteomics.
For example, through proteomics, researchers led by Benoit Lehallier, PhD, Biostatistician, Instructor of Neurology and Neurological Sciences, and senior author Tony Wyss-Coray, PhD, Professor of Neurology and Neurological Sciences and co-director of the Stanford Alzheimer’s Disease Research Center at Stanford University in California, gained an understanding of aging that suggest intriguing possibilities for clinical laboratories.
In their study, published in Nature, titled, “Undulating Changes in Human Plasma Proteome Profiles Across the Lifespan,” the scientists stated that aging doesn’t happen in a consistent process over time, reported Science Alert.
The Stanford researchers also found that they can accurately
determine a person’s age based on the levels of certain proteins in his or her
blood.
Additionally, the study of proteomics may finally explain why blood from young people can have a rejuvenating effect on elderly people’s brains, noted Scientific American.
Each of these findings is important on its own, but taken
together, they may have interesting implications for pathologists who follow
the research. And medical laboratory leaders may find opportunities in mass
spectrometry in the near future, rather than decades from now.
Three Distinct Stages in Aging and Other Findings
The Stanford study found that aging appears to happen at
three distinct points in a person’s life—around the ages 34, 60, and 78—rather
than being a slow, steady process.
The researchers measured and compared levels of nearly 3,000
specific proteins in blood plasma taken from healthy people between the ages of
18 and 95 years. In the published study, the authors wrote, “This new approach
to the study of aging led to the identification of unexpected signatures and
pathways that might offer potential targets for age-related diseases.”
Along with the findings regarding the timeline for aging, the researchers found that about two-thirds of the proteins that change with age differ significantly between men and women. “This supports the idea that men and women age differently and highlights the need to include both sexes in clinical studies for a wide range of diseases,” noted a National Institutes of Health (NIH) report.
“We’ve known for a long time that measuring certain proteins in the blood can give you information about a person’s health status—lipoproteins for cardiovascular health, for example,” stated Wyss-Coray in the NIH report. “But it hasn’t been appreciated that so many different proteins’ levels—roughly a third of all the ones we looked at—change markedly with advancing age.”
Tony Wyss-Coray, PhD (above), Professor of Neurology and Neurological Sciences at Stanford University, was senior author of the proteomics study that analyzed blood plasma from 4,263 people between the ages 18-95. “Proteins are the workhorses of the body’s constituent cells, and when their relative levels undergo substantial changes, it means you’ve changed, too,” he said in a Stanford Medicine news article. “Looking at thousands of them in plasma gives you a snapshot of what’s going on throughout the body.” (Photo copyright: Stanford University.)
Differentiating Aging from Disease
Previous research studies also found it is indeed possible
to measure a person’s age from his or her “proteomic signature.”
The researchers published their findings in Aging Cell, a peer-reviewed open-access journal of the Anatomical Society in the UK, titled, “Plasma Proteomic Signature of Age in Healthy Humans.” In it, the authors wrote, “Our results suggest that there are stereotypical biological changes that occur with aging that are reflected by circulating proteins.”
The fact that chronological age can be determined through a
person’s proteomic signature suggests researchers could separate aging from
various diseases. “Older age is the main risk factor for a myriad of chronic
diseases, and it is invariably associated with progressive loss of function in
multiple physiological systems,” wrote the researchers, adding, “A challenge in
the field is the need to differentiate between aging and diseases.”
Can Proteins Cause Aging?
Additionally, the Stanford study found that changes in protein levels might not simply be a characteristic of aging, but may actually cause it, a Stanford Medicine news article notes.
“Changes in the levels of numerous proteins that migrate
from the body’s tissues into circulating blood not only characterize, but quite
possibly cause, the phenomenon of aging,” Wyss-Coray said.
Can Proteins Accurately Predict Age? Not Always
There were, however, some instances where the protein levels inaccurately predicted a person’s age. Some of the samples the Stanford researchers used were from the LonGenity research study conducted by the Albert Einstein College of Medicine, which investigated “why some people enjoy extremely long life spans, with physical health and brain function far better than expected in the 9th and 10th decades of life,” the study’s website notes.
That study included a group of exceptionally long-lived Ashkenazi Jews, who have a “genetic proclivity toward exceptionally good health in what for most of us is advanced old age,” according to the Stanford Medicine news article.
“We had data on hand-grip strength and cognitive function
for that group of people. Those with stronger hand grips and better measured
cognition were estimated by our plasma-protein clock to be younger than they
actually were,” said Wyss-Coray. So, physical condition is a factor in
proteomics’ ability to accurately prediction age.
Although understanding the connections between protein in
the blood, aging, and disease is in early stages, it is clear additional
research is warranted. Not too long ago the idea of consumers having their DNA
sequenced from a home kit for fun seemed like fantasy.
However, after multiple FDA approvals, and the success of
companies like Ancestry, 23andMe, and the clinical laboratories that serve them,
the possibility that proteomics might go the same route does not seem so
far-fetched.
By offering DTC preventative gene sequencing, hospital leaders
hope to help physicians better predict cancer risk and provide more accurate
diagnoses
Two Boston health systems, Brigham and Women’s Hospital and Massachusetts General Hospital (MGH), are the latest to open preventative gene sequencing clinics and compete with consumer gene sequencing companies, such as 23andMe and Ancestry, as well as with other hospital systems that already provide similar services.
This may provide opportunities for clinical laboratories. However, some experts are concerned that genetic sequencing may not be equally available to patients of all socioeconomic classes. Nor is it clear how health systems plan to pay for the equipment and services, since health insurance companies continue to deny coverage for “elective” gene sequencing, or when there is not a “clear medical reason for it, such as for people with a long family history of cancer,” notes STAT.
Therefore, not everyone is convinced of the value of gene sequencing to either patients or hospitals, even though advocates tout gene sequencing as a key element of precision medicine.
Is Preventative Genetic Sequencing Ready for the Masses?
Brigham’s Preventive Genomics Clinic offers comprehensive DNA sequencing, interpretation, and risk reporting to both adults and children. And MGH “plans to launch its own clinic for adults that will offer elective sequencing at a similar price range as the Brigham,” STAT reported.
The Brigham and MGH already offer similar gene sequencing services as other large health systems, such as Mayo Clinic and University of California San Francisco (UCSF), which are primarily used for research and cancer diagnoses and range in price depending on the depth of the scan, interpretation of the results, and storage options.
However, some experts question whether offering the
technology to consumers for preventative purposes will benefit anyone other
than a small percentage of patients.
“It’s clearly not been demonstrated to be cost-effective to promote this on a societal basis,” Robert Green, MD, MPH, medical geneticist at Brigham and Women’s Hospital, and professor of genetics at Harvard, told STAT. “The question that’s hard to answer is whether there are long-term benefits that justify those healthcare costs—whether the sequencing itself, the physician visit, and any downstream testing that’s stimulated will be justified by the situations where you can find and prevent disease.”
Additionally, large medical centers typically charge more
for genomic scans than consumer companies such as 23andMe and Ancestry. Hospital-based
sequencing may be out of the reach of many consumers, and this concerns some
experts.
“The idea that genomic sequencing is only going to be
accessible by wealthy, well-educated patrons who can pay out of pocket is
anathema to the goals of the publicly funded Human Genome Project,” Jonathan
Berg, MD, PhD, Genetics Professor, University of North Carolina at Chapel
Hill, told Scientific
American.
And, according to the American Journal of Managed Care, “It’s estimated that by 2021, 100 million people will have used a direct-to-consumer (DTC) genetic test. As these tests continue to gain popularity, there is a need for educating consumers on their DTC testing results and validating these results with confirmatory testing in a medical-grade laboratory.”
This is why it’s critical that clinical laboratories and
anatomic pathology groups have a genetic testing and gene sequencing strategy,
as Dark
Daily reported.
David Bick, MD, Chief Medical Officer at the HudsonAlpha Institute for Biotechnology and Medical Director of the Smith Family Clinic for Genomic Medicine, told Scientific American, “there’s just more and more interest from patients and families not only because of 23andMe and the like, but because there’s just this understanding that if you can find out information about your health before you become sick, then really our opportunity as physicians to do something to help you is much greater.”
In an article he penned for Medium, Robert Green, MD, MPH (shown above counseling a patient), medical geneticist at Brigham and Women’s Hospital and professor of genetics at Harvard, wrote, “The ultimate aim of our Genomes2People Research Program is to contribute to the transformation of medicine from reactive to proactive, from treatment-oriented to preventive. We are trying to help build the evidence base that will justify societal decision to make these technologies and services accessible to anyone who wants them, regardless of means, education or race and ethnicity.” (Photo copyright: Wall Street Journal.)
Is Preventative Genomics Elitist?
As large medical centers penetrate the consumer genetic
testing market some experts express concerns. In a paper he wrote for Medium,
titled, “Is Preventive Genomics Elitist?” Green asked, “Is a service like this
further widening the inequities in our healthcare system?”
Green reported that while building the Preventive Genomics Clinic at Brigham, “we … struggled with the reality that there is no health insurance coverage for preventive genomic testing, and our patients must therefore pay out of pocket. This is a troubling feature for a clinic at Brigham and Women’s Hospital, which is known for its ties to communities in Boston with diverse ethnic and socioeconomic backgrounds.”
Most of Brigham’s early genetics patients would likely be “well-off,
well-educated, and largely white,” Green wrote. “This represents the profile of
typical early adopters in genetic medicine, and in technology writ large. It
does not, however, represent the Clinic’s ultimate target audience.”
More Data for Clinical Laboratories
Nevertheless, preventive genomics programs offered by large
health systems will likely grow as primary care doctors and others see evidence
of value.
Therefore, medical laboratories that process genetic
sequencing data may soon be working with growing data sets as more people reach
out to healthcare systems for comprehensive DNA sequencing and reporting.
Number of patients eligible for genome-driven oncology therapy is increasing, but the percentage who reportedly benefit from the therapy remains at less than 5%
Advances in precision medicine in oncology (precision oncology) are fueling the need for clinical laboratory companion diagnostic tests that help physicians choose the best treatment protocols. In fact, this is a fast-growing area of clinical diagnostics for the nation’s anatomic pathologists. However, some experts in the field of genome-based cancer treatments disagree over whether such treatments offer more hype than hope.
Prasad and his colleagues evaluated 31 US Food and Drug
Administration (FDA) approved drugs, which were “genome-targeted” or
“genome-informed” for 38 indications between 2006 and 2018. The researchers
sought to answer the question, “How many US patients with cancer are eligible
for and benefit annually from genome-targeted therapies approved by the US Food
and Drug Administration?”
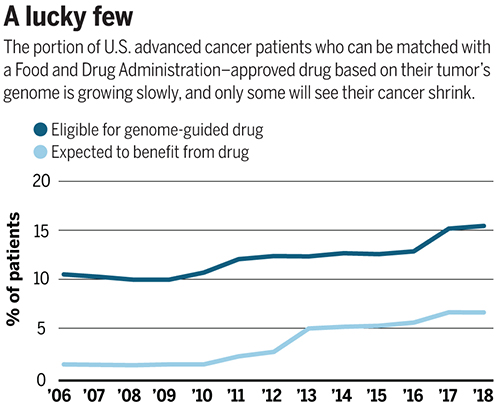
They found that in 2018 only 8.33% of 609,640 patients with
metastatic cancer were eligible for genome-targeted therapy—though this was an
increase from 5.09% in 2006.
Even more telling from Prasad’s view, his research team concluded
that only 4.9% had benefited from such treatments. Prasad’s study found the
percentage of patients estimated to have benefited from genome-informed therapy
rose from 1.3% in 2006 to 6.62% in 2018.
“Although the number of patients eligible for genome-driven treatment has increased over time, these drugs have helped a minority of patients with advanced cancer,” the researchers concluded. “To accelerate progress in precision oncology, novel trial designs of genomic therapies should be developed, and broad portfolios of drug development, including immunotherapeutic and cytotoxic approaches, should be pursued.”
The graph above is based on data from a study published in Science titled, “Estimation of the Percentage of US Patients With Cancer Who Benefit from Genome-Driven Oncology,” co-authored by Vinay Prasad, MD, MPH, et al. (Image copyright: Science.)
A Value versus Volume Argument?
Hyman, who leads a team of oncologists that conduct dozens
of clinical trials and molecularly selected “basket studies” each year,
countered Prasad’s assertions by noting the increase in the number of patients
who qualify for precision oncology treatments.
As reported in Science, Hyman said during his AACR
presentation that Sloan Kettering matched 15% of the 25,000 patients’ tumors it
tested with FDA-approved drugs and 10% with drugs in clinical trials.
“I think this is certainly not hype,” he said during the
conference.
Hyman added that another 10% to 15% of patient tumors have a
DNA change that matches a potential drug tested in animals. He expects “basket”
trials to further increase the patient pool by identifying drugs that can work
for multiple tumor types.
The US National Institute of Health (NIH) describes “basket studies” as “a new sort of clinical studies to identify patients with the same kind of mutations and treat them with the same drug, irrespective of their specific cancer type. In basket studies, depending on the mutation types, patients are classified into ‘baskets.’ Targeted therapies that block that mutation are then identified and assigned to baskets where patients are treated accordingly.”
Are Expectations of Precision Medicine Exaggerated?
A profile in MIT Technology Review, titled, “The Skeptic: What Precision Medicine Revolution?,” describes Prasad’s reputation as a “professional scold” noting the 36-year-old professor’s “sharp critiques of contemporary biomedical research, including personalized medicine.” Nevertheless, Prasad is not alone in arguing that precision oncology’s promise is often exaggerated.
“Like most ‘moonshot’ medical research initiatives,
precision medicine is likely to fall short of expectations,” Joyner wrote.
“Medical problems and their underlying biology are not linear engineering
exercises and solving them is more than a matter of vision, money, and will.”
“Although some niche applications have been found for
precision medicine—and gene therapy is now becoming a reality for a few rare
diseases—the effects on public health are miniscule while the costs are astronomical,”
they wrote.
Hope for Precision Medicine Remains High
However, optimism over precision oncology among some industry leaders has not waned. Cindy Perettie, CEO of molecular information company Foundation Medicine of Cambridge, Mass., argues genome-directed treatments have reached an “inflection point.”
“Personalized cancer treatment is a possibility for more patients than ever thanks to the advent of targeted therapies,” she told Genetic Engineering and Biotechnology News. “With a growing number of new treatments—including two pan-tumor approvals—the need for broad molecular diagnostic tools to match patients with these therapies has never been greater. We continue to advance our understanding of cancer as a disease of the genome—one in which treatment decisions can be informed by insight into the genomic changes that contribute to each patient’s unique cancer.”
Prasad acknowledges genome-driven therapies are beneficial for some cancers. However, he told MIT Technology Review the data doesn’t support the “rhetoric that we’re reaching exponential growth, or that is taking off, or there’s an inflection point” signaling rapid new advancements.
“Right now, we are investing heavily in immunotherapy and heavily in genomic therapy, but in other categories of drugs, such as cytotoxic drugs, we have stopped investigating in them,” he told Medscape Medical News. “But it’s foolish to do this—we need to have the vision to look beyond the fads we live by in cancer medicine and do things in a broader way,” he added.
“So, I support broader funding because you have to sustain
efforts even when things are not in vogue if you want to make progress,” Prasad
concluded.
Is precision oncology a fad? Dark Daily has covered the advancements in precision medicine extensively over the past decade, and with the launch of our new Precision Medicine Institute website, we plan to continue reporting on further advancements in personalized medicine.
Time will tell if precision oncology can fulfill its
promise. If it does, anatomic pathologists will play an important role in
pinpointing patients most likely to benefit from genome-driven treatments.
One thing that the debate between proponents of precision
medicine in oncology and their critics makes clear is that more and better
clinical studies are needed to document the true effectiveness of target
therapies for oncology patients. Such evidence will only reinforce the
essential role that anatomic pathologists play in diagnosis, guiding
therapeutic decisions, and monitoring the progress of cancer patients.