Service uses ‘hub-and-spoke’ routing model to provide rapid delivery of time-and-temperature-sensitive clinical laboratory specimens and supplies
Drone delivery service in healthcare is beginning to take flight both here and abroad, with California-based Matternet launching medical drone delivery networks in Winston-Salem, North Carolina, and Berlin, Germany.
The successful use of unmanned aircraft to deliver patient specimens has major implications for clinical laboratories. When conditions allow them to fly, drones can significantly shorten delivery times of routine patient specimens such as blood and urine.
The drones will fly two routes and carry scheduled deliveries of specialty infusion medicines and personal protective equipment (PPE). Because infusion medicines are patient-specific, high cost, and have a short shelf life, delivery by drone within 10 minutes is an ideal solution, Matternet said in the news release. Individually compounded medicines also will be delivered on-demand for dispensing to patients who need real-time access to treatments.
“This partnership with UPSFF aligns strategically with our mission to improve the health of those in the communities that we serve as well as our Virtual Health sector in iQ Healthtech Labs,” said Jane Shen, PharmD (above), Chief Strategy Officer at the Wake Forest Institute for Regenerative Medicine, and Head of Sector Development for Innovation Quarter, a subsidiary of iQ Healthtech Labs, in the IQ Healthtech Labs news release. “We seek to leverage technology advances to make access to healthcare easier and more effective. Collaborating in innovative ways with a key logistics partner like UPS allows Wake Forest Baptist to deliver care in better and more efficient ways to patients and their families.” (Photo copyright: Triad Business Journal.)
Matternet has been operating in the US since August 2018. In, “WakeMed Uses Drone to Deliver Patient Specimens,” Dark Daily’s sister publication, The Dark Report, reported how—following a two-year trial period using a quadcopter to deliver patients’ samples from a physicians’ office satellite lab/draw station to the WakeMed Medical Center’s central lab—the North Carolina healthcare system, in partnership with UPSFF, completed the first successful revenue-generating commercial transport of lab supplies by drone in the US at WakeMed’s flagship hospital and campus in Raleigh, N.C.
Bala Ganesh, a Vice President of Engineering at UPS, said UPSFF, which was launched in July 2019, is focused on healthcare deliveries. To make drone deliveries commercially viable, both “criticality” and an industry’s “willingness to pay” are important, he said. “We never looked at delivering pizza,” he told Forbes. UPSFF is the first company to receive the FAA’s Part 135 certification (package delivery by drone).
The video above demonstrates Matternet’s “Easy-to-use interface for sending and receiving packages 24/7/365.” The Matternet Station (above) is “integrated with the Matternet Cloud [Matternet’s proprietary software platform for operating Matternet networks] and the M2 Drone for payload and battery exchange, and autonomous take-off and landing. The station “can store up to seven payloads and batteries and hold one Matternet M2 Drone in its hangar.” Hospital-based clinical laboratory managers will appreciate the ease at which the station can be accessed by lab personnel. Click here to watch the full video. (Video and caption copyright: Matternet.)
BVLOS Drone Delivery of Clinical Laboratory Specimens in Europe
Last year, Matternet launched the first beyond-visual-line-of-sight (BVLOS)-operated medical drone network in Europe. Its unmanned aircraft will be flown without the requirement that a pilot always maintain a visual line of sight on the aircraft.
Matternet launched its BVLOS operations at Labor Berlin, Europe’s largest hospital laboratory, which includes facilities in 13 hospitals across Berlin.
“We continue to expand drone delivery operations around the world with a focus on urban environments,” said Andreas Raptopoulos, Matternet Founder and CEO, in a press release. “Hospitals and laboratories in densely populated cities like Berlin need fast and predictable transportation methods that avoid urban congestion. We are thrilled to partner with Labor Berlin and look forward to streamlining their diagnostics work to the benefit of Berlin’s hospitals and residents.”
According to the press release, Matternet’s drone delivery network will transport samples from hospitals to Labor Berlin facilities up to 70% faster than ground courier services, as well as reducing vehicular traffic and emissions in Berlin’s urban core. Currently, more than 15,000 samples are transported daily across Labor Berlin’s healthcare system.
Will Drone Delivery of Clinical Laboratory Specimens Become the New Normal?
“I think that this is the wave of the future,” Atrium Health Senior Vice President Conrad Emmerich, who previously served as Senior Vice President, Business Services, at Wake Forest Baptist Health, told Fox 8 News.
It’s certainly beginning to look as if drone delivery as a viable alternative to traditional transport methods is taking off (pun intended). Since 2017, Dark Daily has published 10 ebriefings on drone delivery systems for healthcare being trailed worldwide.
Since the shortest distance between two points is a straight line, regular transporting of clinical laboratory specimens and supplies by drone could reduce transit times between hospitals and clinical laboratories and lower laboratory specimen transportation costs.
Hospital administrators and medical laboratory executives may want to keep tabs on the expansion of such services into their regions. There may be opportunities to improve clinical outcomes and patient satisfaction.
Studies into use of population-level genomic cancer screening show promising results while indicating that such testing to find evidence of increased cancer risk among non-symptomatic people may be beneficial
In another example of a government health system initiating a program designed to proactively identify people at risk for a serious disease to allow early clinical laboratory diagnosis and monitoring for the disease, cancer researchers at Monash University in Australia have receive a $2.97 million grant from the Medical Research Future Fund (MRFF) to study ways to “identifying people who are living with a heightened cancer risk who would ordinarily be informed only after a potentially incurable cancer is diagnosed.”
According to a Monash news release, the researchers, led by Associate Professor Paul Lacaze, PhD, Head of the Public Health Genomics Program at Monash University, plan to use the award to develop a “new low-cost DNA screening test which will be offered to 10,000 young Australians. The new approach, once scaled-up, has the potential to drastically improve access to preventive genetic testing in Australia, and could help make Australia the world’s first nation to offer preventive DNA screening through a public healthcare system.”
Called DNACancerScreen, the clinical genetic test will be offered to anyone between the ages of 18 and 40, rather than to a select group of people who have a family history of cancer or who present with symptoms. The Monash scientists hope to advance knowledge about the relationship of specific genes and how they cause or contribute to cancer. Such information, they believe, could lead to the development of new precision medicine diagnostic tests and anti-cancer drug therapies.
Gap in Current Cancer Screening Practices
The DNACancerScreen test will look for genes related to two specific cancer categories:
Hereditary Breast and Ovarian Cancer Syndrome is associated with an increased risk of developing breast, ovarian, prostate, and pancreatic cancers, as well as melanoma. Lynch Syndrome is associated with colorectal, endometrial, ovarian, and other cancers.
Currently, screening practices may miss as many as 50-90% of individuals who carry genetic mutations associated with hereditary breast and ovarian cancer, and as many as 95% of those at risk due to Lynch Syndrome, according to the Monash news release.
But currently, only those with a family history of these cancers, or those who present with symptoms, are screened. By targeting younger individuals for screening, Lacaze and his team hope to give those at risk a better chance at early detection.
“This will empower young Australians to take proactive steps to mitigate risk, for earlier detection, surveillance from a younger age, and prevention of cancer altogether,” Lacaze said in the news release.
Along with the possibility of saving lives, Associate Professor Paul Lacaze, PhD (above), Head of the Public Health Genomics Program at Monash University, expects that the screening program will have an economic impact as well. “This type of preventive DNA testing will not only save lives, but also save the Australian public healthcare system money by preventing thousands of cancers,” he said. There’s evidence to back up his statement. In 2019 he led a team that published a study, titled, “Population Genomic Screening of All Young Adults in a Healthcare System: A Cost Effectiveness Analysis.” That study concluded, “Preventive genomic screening in early adulthood would be highly cost-effective in a single-payer healthcare system, but ethical issues must be considered.” (Photo copyright: Monash University.)
Similar Genetic Studies Show Encouraging Results
Although the DNACancerScreen study in Australia is important, it is not the first to consider the impact of population-level screening for Tier 1 genetic mutations. The Healthy Nevada Project (HVN), a project that combined genetic, clinical, environmental, and social data, tested participants for those Tier 1 conditions. The project was launched in 2016 and currently has more than 50,000 participants, a Desert Research Institute (DRI) press release noted.
In 2018, HVN began informing participants who had increased risk for hereditary breast and ovarian cancer, Lynch Syndrome, and a third condition called Familial Hypercholesterolemia. There were 27,000 participants, and 90% of those who had genetic mutations associated with the three Tier 1 conditions had not been previously identified.
“Our first goal was to deliver actionable health data back to the participants of the study and understand whether or not broad population screening of CDC Tier 1 genomic conditions was a practical tool to identify at-risk individuals,” said Joseph Grzymski, PhD, lead author of the HVN study in the DRI press release.
Grzymski is Principal Investigator of the Healthy Nevada Project, Director of the Renown Institute for Health Innovation, Chief Scientific Officer for Renown Health, and a Research Professor in Computational Biology and Genetics at the Desert Research Institute.
“Now, two years into doing that it is clear that the clinical guidelines for detecting risk in individuals are too narrow and miss too many at risk individuals,” he added.
A total of 358, or 1.33% of the 26,906 participants in the Healthy Nevada Project were carriers for the Tier 1 conditions, but only 25% of them met the current guidelines for screening, and only 22 had any previous suspicion in their medical records of their genetic conditions.
Another project, the MyCode Community Health Initiative conducted at Geisinger Health System, found that 87% of participants with a Tier 1 gene variant did not have a prior diagnosis of a related condition. When the participants were notified of their increased risk, 70% chose to have a related, suggested procedure.
“This evidence suggests that genomic screening programs are an effective way to identify individuals who could benefit from early intervention and risk management—but [who] have not yet been diagnosed—and encourage these individuals to take measures to reduce their risk,” a Geisinger Health press release noted.
Realizing the Promise of Precision Medicine
Studies like these are an important step in realizing the potential of precision medicine in practical terms. The Tier 1 genetic conditions are just a few of the more than 22,000 recognized human genes of which scientists have a clear understanding. Focusing only on those few genetic conditions enables clinicians to better help patients decide how to manage their risk.
“Genomic screening can identify at-risk individuals more comprehensively than previous methods and start people on the path to managing that risk. The next step is figuring out the impact genomic screening has on improving population health,” said Adam Buchanan, MPH, MS, Director of Geisinger’s Genomic Medicine Institute.
These are positive developments for clinical laboratories and anatomic pathology group practices. The three examples cited above show that a proactive screening program using genetic tests can identify individuals at higher risk for certain cancers. Funding such programs will be the challenge.
At the current cost of genetic testing, screening 100 people to identify a few individuals at high risk for cancer would probably not be considered the highest and best use of the limited funds available to the healthcare system.
Microbiologists will want to take note of the CDC’s statement that the illness can masquerade as other diseases
It is the latest example of a bacterium uncommon in the United States that has infected patients in this country—one of whom has died. The three infected patients live in separate states, but genetic analysis indicates their cases may be related.
According to the health alert, “Based on genomic analysis, these three cases (one male, two females; two adults and one child) may share a potential common source of exposure. The first case, identified in March 2021, was fatal. Two other patients were identified in May 2021, one of whom is still hospitalized. One has been discharged to a transitional care unit. None of the patients’ families reported a history of traveling outside of the continental United States.”
The CDC warned, “Symptoms of melioidosis are varied and nonspecific and may include pneumonia, abscess formation, and/or blood infections. Due to its nonspecific symptoms, melioidosis can initially be mistaken for other diseases such as tuberculosis, and proper treatment may be delayed.”
Microbiology Laboratories Should Be on Alert
Melioidosis is typically only seen in subtropical and tropical regions and can be highly fatal. It is unknown how the trio of patients who contracted the illness became infected, but according to the CDC the cases do appear to be connected.
“Testing suggests a common source of infection, but that source has not yet been identified,” a CDC representative told Gizmodo. “CDC is working with states to assess exposures or products these individuals have in common, as well as environmental samples from the states where cases have been identified. Additionally, CDC experts are providing epidemiologic assistance to help investigate the cause of infection,” the CDC added.
“Melioidosis is a serious neglected tropical disease of Southeast Asia, India, and Australia where it is a major cause of pneumonia, abscesses, and sepsis. The fact that it may be gaining a foothold in the US is concerning,” pediatrician Peter Hotez, MD, PhD (above), Dean of the National School of Tropical Medicine, Professor of Pediatrics and Molecular Virology and Microbiology at Baylor College of Medicine, and Director of the Center for Vaccine Development at Texas Children’s Hospital, told Gizmodo. Clinical laboratories and microbiologists will want to monitor these cases for future developments. (Photo copyright: Baylor College of Medicine.)
Melioidosis, also called Whitmore’s disease, was first described by Alfred Whitmore, an English pathologist, in 1912 in what is now present-day Myanmar. The bacterium (Burkholderia pseudomallei) can be found in contaminated soil and water. It is predominately found in tropical climates in Southeast Asia and northern Australia and can affect humans and many species of animals.
Researchers believe the disease may be acquired through the inhalation of contaminated dust particles or water droplets, the ingestion of contaminated water or soil-contaminated food, or other contact with tainted soil, especially through skin abrasions. It is very rare to contract melioidosis from infected individuals.
Melioidosis Masquerades as Other Illnesses
The symptoms of melioidosis are wide-ranging and non-specific and can resemble those of other illnesses. In addition, there are several types of the illness, and they can each act differently depending on where the infection is in the body. The most common symptoms of melioidosis include:
Localized Infection:
Localized pain or swelling
Fever
Ulceration
Abscess
Pulmonary Infection:
Cough
Chest pain
High fever
Headache
Anorexia
Bloodstream Infection:
Fever
Headache
Respiratory distress
Abdominal discomfort
Joint pain
Disorientation
Disseminated Infection:
Fever
Weight loss
Stomach or chest pain
Muscle or joint pain
Headache
Central nervous system/brain infection
Seizures
According to the CDC, the time between an exposure to Burkholderia pseudomallei and the first emergence of Melioidosis symptoms is not clearly defined but could range from one day to many years. However, most infected individuals begin experiencing symptoms of melioidosis within two to four weeks after exposure.
Melioidosis is difficult to diagnose, and some automated bacterial reading instruments can mistake Burkholderia pseudomallei for other bacteria. It is estimated that the disease accounts for 89,000 deaths per year worldwide. Delays in diagnosis and treatment often lead to poor patient outcomes and the mortality rate can exceed 40% in some regions, Nature reported.
The illness is typically treated with appropriate drug therapies including intravenous antimicrobial medications, such as Ceftazidime or Meropenem, followed by an oral antimicrobial therapy such as Trimethoprim-sulfamethoxazole or Amoxicillin/Clavulanic Acid. It may take several months for a patient to be cured of melioidosis, depending on the extent of the infection.
Deadly Bacterium’s Countries of Origin and Spread to the US
According to CDC data, the greatest number of melioidosis cases are reported in Thailand, Malaysia, Singapore, and northern Australia. Cases also have been reported in other Asian countries as well as Mexico and Central America.
Burkholderia pseudomallei does not occur naturally in the US, and cases of melioidosis identified in the US are usually only seen in world travelers and immigrants who come from countries where the disease is widespread. The bacterium has been found in soil in Mexico, so it is possible that it could spread to parts of the US, which has led to concern among microbiologists.
“Due to changes in weather patterns, some pathogens that normally were not present in a particular area might start causing disease,” Alfredo Torres, PhD, Associate Provost, Department of Microbiology and Immunology, University of Texas Medical Branch, told Gizmodo. “Therefore, it is important to make the health professionals aware of this pathogen and the disease that it causes, so quick identification can be done, and treatment is properly used to save lives. Without that, it might be too late for the next melioidosis patient when the proper diagnosis is done.”
The CDC has suggested that healthcare workers consider melioidosis as a possible diagnosis for patients who have compatible symptoms, even if they have not recently traveled outside of the US.
CDC Suggests Rerunning Certain Clinical Laboratory Tests
Because Burkholderia pseudomallei can be mistaken for other bacteria, the CDC also urges the rerunning of clinical laboratory tests using automated identification, especially if another bacterium that is often mistaken for Burkholderia pseudomallei is present, Gizmodo noted.
“CDC encourages healthcare workers to be aware of the potential for more cases and to report cases to their state health departments,” the CDC stated.
The CDC considers the risk of melioidosis to the public in the US to be low, and that the chances of a potential outbreak are unlikely. However, the origins of these three cases remain a mystery and warrant further investigation.
Microbiologists and clinical laboratories should be aware of and remain alert about this potentially fatal illness. It is possible that more cases will arise in the future, especially in the three states where it has already been found.
Six-episode show is based on popular ABC Radio podcast “The Dropout,” which focused on the three-year investigation that brought down clinical laboratory test developer Theranos
While former Theranos CEO Elizabeth Holmes awaits the start of her August 31 criminal fraud trial in a federal court in Northern California, one streaming video service is lining up a star-studded cast to tell the story of the Silicon Valley executive’s fall from grace and the demise of her clinical laboratory blood-testing company.
This six-part series is being produced by Hulu, an on-demand video streaming service offering live and on-demand content. Back in 2019, it announced that it would produce the “The Dropout,” a limited series chronicling Holmes’ rise and fall from Founder and CEO of $9 billion tech company Theranos to criminal defendant.
Hulu says the series will launch this fall, so pathologists and medical laboratory managers have time to set their recorders to capture what may be a compelling story of hubris that took investors and the news media on a wild ride. The Theranos publicity machine was so effective that many hospital CEOs went to their clinical laboratory administrators and told them to delay equipment purchases because Theranos would be able to do the same medical laboratory tests at just pennies on the existing lab-cost dollar.
Holmes’ carefully-crafted public image as Theranos’ CEO drew comparisons to the late Apple CEO Steve Jobs, Business Insider noted. This has made her a popular topic not only among clinical laboratory scientists but also Hollywood moviemakers.
“The Dropout” took its inspiration from the ABC Audio podcast of the same name, hosted by ABC Chief Business, Technology and Economics correspondent Rebecca Jarvis. The ABC Audio podcast’s description provides a glimpse into the direction the miniseries will take.
“Money. Romance. Tragedy. Deception. The story of Elizabeth Holmes and Theranos is an unbelievable tale of ambition and fame gone terribly wrong. How did the world’s youngest self-made female billionaire lose it all in the blink of an eye? How did the woman once heralded as ‘the next Steve Jobs’ find herself facing criminal charges—to which she pleaded not guilty—and up to 20 years in jail? How did her technology, meant to revolutionize healthcare, potentially put millions of patients at risk? And how did so many smart people get it so wrong along the way?” the ABC Audio website states.
The Hulu series originally was to star “Saturday Night Live” cast member Kate McKinnon as Holmes but was recast with Amanda Seyfried in the starring role. According to Variety, the series will include a notable lineup of guest stars including:
Naveen Andrews will play former Theranos President and COO Ramesh Balwani, whose own criminal fraud trial is expected to begin early next year.
A release date for the limited series has not yet been announced, Town and Country reported.
Elizabeth Holmes (above), former CEO of now defunct company Theranos, faces 11 counts of fraud for alleged false claims that the clinical laboratory testing company had created a revolutionary finger-prick technology capable of performing a wide range of clinical laboratory tests. Among the charges are two counts of conspiracy to commit wire fraud and nine counts of wire fraud, for which Holmes could serve up to 20 years in jail if found guilty of all charges, according to court documents. She has pleaded not guilty. (Photo copyright: The Wall Street Journal.)
The ‘Real World’ Wall Street Journal Investigation of Theranos and Holmes
Dark Daily has reported extensively on the Holmes/Theranos saga, including the recent development that Holmes’ repeatedly-delayed trial would be pushed back from mid-July to August 31 because Holmes is due to give birth in July.
Theranos’ alleged deceptions first were brought to light in a series of 2015 investigative reports in The Wall Street Journal (WSJ). Then-WSJ investigative reporter John Carreyrou alleged Theranos had not disclosed publicly that the vast majority of its tests were not being done with proprietary technology, but instead with traditional machines purchased from Siemens AG and other companies.
And for those looking for even more drama centered around the Theranos saga, a feature film starring Jennifer Lawrence as Elizabeth Holmes, titled, “Bad Blood,” remains “in development” according to People magazine. Though the project was announced in 2016, filming has yet to begin.
Meanwhile, clinical laboratory scientists will soon get to watch the next “real world” chapter in the Holmes’ saga play out in federal court later this summer. They will also have multiple opportunities in the coming years to be “entertained” by the Theranos scandal on big and small screens.
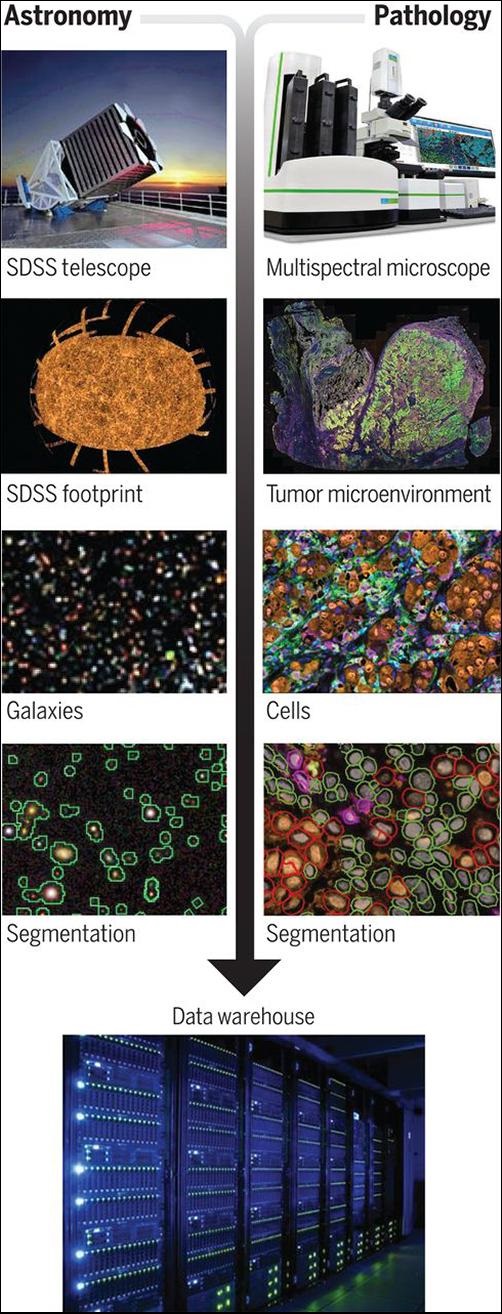
Using algorithmic technology designed for mapping the stars, the scientists have created an imaging/spatial location platform called AstroPath which may help oncologists develop immunotherapies that work best on specific cancers. Such a capability is key to effective precision medicine techniques.
Dark Daily has regularly pointed out that technologies developed in other fields of science will eventually be brought into anatomic pathology and clinical laboratory medicine. Use of the star-mapping technology in oncology and the diagnosis of cancer is one such example.
In “Analysis of Multispectral Imaging with the AstroPath Platform Informs Efficacy of PD-1 Blockade,” published in the journal Science, the multi-institution research team wrote, “Here, we present the AstroPath platform, an end-to-end pathology workflow with rigorous quality control for creating quantitative, spatially resolved mIF [multiplex immunofluorescence] datasets. Although the current effort focused on a six-plex mIF assay, the principles described here provide a general framework for the development of any multiplex assay with single-cell image resolution. Such approaches will vastly improve the standardization and scalability of these technologies, enabling cross-site and cross-study comparisons. This will be essential for multiplex imaging technologies to realize their potential as biomarker discovery platforms and ultimately as standard diagnostic tests for clinical therapeutic decision-making.
“Drawing from the field of astronomy, in which petabytes of imaging data are routinely analyzed across a wide spectral range, [the researchers] developed a platform for multispectral imaging of whole-tumor sections with high-fidelity single-cell resolution. The resultant AstroPath platform was used to develop a multiplex immunofluorescent assay highly predictive of responses and outcomes for melanoma patients receiving immunotherapy,” the researchers added.
Using Star Mapping Software to Fight Cancer
“The application of advanced mapping techniques from astronomy has the potential to identify predictive biomarkers that will help physicians design precise immunotherapy treatments for individual cancer patients,” said Michele Cleary, PhD, CEO of the Mark Foundation for Cancer Research, in a Johns Hopkins news release.
Although the universe we live in and the universe of a cancerous tumor may not seem related, the fact is the same visualization technology can be used to map them both.
“What should be pointed out is that astronomy is mapping the sky in three dimensions, so keeping the spatial relationships while also identify each heavenly body is the goal of these algorithms,” said Robert Michel, Publisher and Editor-in-Chief of Dark Daily and its sister publication The Dark Report.
“Both aspects of that information technology have value in surgical pathology, where the spatial relationship of different cells and cell structures is relevant and important while also having the ability to identify and characterize different types of cells and cell structures. This technology appears to also be capable of identifying multiple biomarkers,” he added.
The image above, taken from the researchers’ Science paper, illustrates the “strong parallels between multispectral analyses in astronomy and emerging multiplexing platforms for pathology.” The researchers wrote, “the next generation of tissue-based biomarkers are likely to be identified by use of large, well-curated datasets. To that end, image analysis approaches originally developed for astronomy were applied to pathology specimens to produce trillions of pixels of robust tissue imaging data and facilitate assay and atlas development.” Anatomic pathologists may be direct recipients of new cancer diagnostic tools based on the AstroPath platform. (Photo copyrights: Johns Hopkins University/Mark Foundation Center for Advanced Genomics/Bloomberg-Kimmel Institute.)
AstroPath Provides 1,000 Times the Information Content from A Single Biopsy
According to the news release, “[The researchers] characterized the immune microenvironment in melanoma biopsies by examining the immune cells in and around the cancer cells within the tumor mass and then identified a composite biomarker that includes six markers and is highly predictive of response to a specific type of an immunotherapy called Anti-PD-1 therapy.”
This is where the use of AstroPath is truly innovative. Previously, researchers could only identify those biomarkers one at a time, through a painstaking process.
“For the last 40 years, pathology analysis of cancer has examined one marker at a time, which provides limited information,” said Drew Pardoll, MD, PhD, Director of the Bloomberg-Kimmel Institute for Cancer Immunotherapy and a Johns Hopkins professor of oncology, in the news release. “Leveraging new technology, including instrumentation to image up to 12 markers simultaneously, the AstroPath imaging algorithms provide 1,000 times the information content from a single biopsy than is currently available through routine pathology,” he added.
More information about a cancerous tumor means clinicians have more tools to combat it. Treatment becomes less about finding the right immunotherapy and more about treating it immediately.
“This facilitates precision cancer immunotherapy—identifying the unique features of each patient’s cancer to predict who will respond to a given immunotherapy, such as anti-PD-1, and who will not. In doing so, it also advances diagnostic pathology from uniparameter to multiparameter assays,” Pardoll said.
Big Data and Data Analysis Is the Future of Precision Medicine
The use of data in science is changing how researchers, clinicians, pathologists, and others provide healthcare in the modern world. When it is properly collected and analyzed, data holds the key to precision medicine’s personalized and targeted patient care.
“Big data is changing science. There are applications everywhere, from astronomy to genomics to oceanography,” said Alexander S. Szalay, PhD, Bloomberg Distinguished Professor and Professor in the Department of Computer Science at Johns Hopkins University, and Director of the Institute for Data Intensive Engineering and Science (IDIES), in the news release.
“Data-intensive scientific discovery is a new paradigm. The technical challenge we face is how to get consistent, reproducible results when you collect data at scale. AstroPath is a step towards establishing a universal standard,” he added.
Should AstroPath prove to be a clinically safe and accurate method for developing precision medicine cancer therapies, anatomic pathologists can look forward to exciting new ways to diagnose cancer and determine the best courses of treatment based on each patient’s unique medical needs.
The rapid diagnostic test costs less than $5 per unit and can be adapted for other diseases, the developers say, which opens a slew of possibilities for clinical laboratories
Just as the SARS-CoV-2 coronavirus spurred deployment of new vaccine technology based on messenger RNA (mRNA), the COVID-19 pandemic also could prove to be a watershed for in vitro diagnostics (IVD) innovation in ways that benefit clinical laboratories.
A Penn Medicine news release noted that “The RAPID technology … transforms the binding event between the SARS-CoV-2 viral spike protein and its receptor in the human body, the protein ACE2 (which provides the entry point for the coronavirus to hook into and infect human cells), into an electrical signal that clinicians and technicians can detect. That signal allows the test to discriminate between infected and healthy human samples. The signal can be read through a desktop instrument or a smartphone.”
Though still in its early stages, the technique potentially offers dramatically lower costs and faster results than traditional RT-PCR (reverse transcription polymerase chain reaction) molecular tests. Moreover, the RAPID technology might be useful for identifying other types of biomarkers and could be the basis for diagnostic tests that help reduce the cost-per-test in medical laboratory testing while providing comparable sensitivity and specificity to existing methodologies.
Clinical trials began on January 5, 2021, and the Penn Medicine researchers say the IVD test technology can be applied to other infectious diseases, which, if proven accurate, would be a boon to clinical laboratory testing.
Diagnostic Test Results in Four Minutes for Less than $5/Test
According to the news release, the RAPID 1.0 (Real-time Accurate Portable Impedimetric Detection prototype 1.0) biosensor test costs less than $5 and can deliver results in four minutes. The researchers reported overall accuracy of 87.1% on (139) nasal swab samples and 90% on (50) saliva samples.
The technology uses electrodes that can be mass-produced at low cost on commercially-available screen printers, the researchers said. Results can be read on electronic devices connected to a PC or smartphone.
RAPID 1.0 (above) is a low-cost COVID-19 diagnostic test developed at the César de la Fuente clinical laboratory at the Perelman School of Medicine University of Pennsylvania in Philadelphia. At less than $5/test, plus the ability to be adapted to other diseases, clinical laboratories performing disease screenings in rural or remote locations may have a new tool in the fight against infections. (Photo copyright: University of Pennsylvania.)
Does Penn Medicine’s RAPID 1.0 Test Replace Traditional RT-PCR Testing?
In their published study, the Penn Medicine researchers cited the need for “fast, reliable, inexpensive, and scalable point-of-care diagnostics.”
RT-PCR tests, they said, “are limited by their requirement of a large laboratory space, high reagent costs, multistep sample preparation, and the potential for cross-contamination. Moreover, results usually take hours to days to become available.”
Researchers who have studied the SARS-CoV-2 coronavirus know that it uses a spike-like protein to bind to angiotensin-converting enzyme 2 (ACE2) receptors on the surfaces of human cells.
As described in Penn Medicine’s published study, the biosensor contains ACE2 and other biochemical agents anchored to an electrode. When the SARS-CoV-2 coronavirus attaches to the ACE2, the biosensor transforms the chemical reaction into an electrical signal that can be measured on a device known as a potentiostat.
The researchers tested their RAPID 1.0 technology with two commercially available potentiostat models:
The researchers initially developed the electrode as a printed circuit board, which is relatively expensive. To reduce costs, they constructed a version that uses filter paper as the main component. The researchers noted that one screen printer in a lab can produce 35,000 electrodes per day, including time needed to incorporate the chemical elements. “However, it must be noted that these steps can be fully automated into a production line for industrial purposes, drastically reducing time requirements,” they wrote.
The test can be performed at room temperature, they added, and total cost per unit is $4.67. Much of that—$4.50—is for functionalizing the ACE2 recognition agent. The cost for the bare electrode is just seven cents.
“The overall cost of RAPID may be further reduced through recombinant production of ACE2 and ACE2 variants,” the researchers said, adding that the RAPID 1.0 test can detect the SARS-CoV-2 coronavirus at low concentrations correlating to the earliest stages of the COVID-19 disease.
The Penn Medicine research team was led by César de la Fuente, PhD (above), an Assistant Professor in Psychiatry, Microbiology, Chemical and Biomolecular Engineering and Bioengineering at the Perelman School of Medicine. “Prior to the pandemic, our lab was working on diagnostics for bacterial infections,” he said in the Penn Medicine news release. “But then, COVID-19 hit. We felt a responsibility to use our expertise to help—and the diagnostic space was ripe for improvements.” (Photo copyright: University of Pennsylvania.)
Testing Penn Medicine’s RAPID 1.0 Test
The researchers evaluated the technology in blinded tests with clinical samples from the Hospital of the University of Pennsylvania. The evaluation included 139 nasal swab samples, of which 109 were determined to be COVID-19 positive by RT-PCR tests and clinical assessments. Among these, the RAPID test successfully detected the SARS-CoV-2 coronavirus in 91 samples, for a sensitivity rate of 83.5%. One sample was from a patient diagnosed with the highly contagious SARS-CoV-2 Alpha variant B.1.1.7, which the test correctly identified as positive.
Among the 30 samples determined to be COVID negative, the RAPID test scored a specificity rate of 100%, meaning no false positives. Overall accuracy, including sensitivity and specificity, was 87.1%.
The researchers also analyzed 50 saliva samples: 13 COVID-positive and 37 COVID-negative. The test correctly identified all 13 positive samples but produced five false-positives among the 37 negative samples, for a specificity rate of 86.5%. The researchers speculated that this could be due to interactions between ACE2 and other biomolecules in the saliva but suggested that performance “will improve when using fresh saliva samples at the point-of-care.”
Are There Other Applications for the RAPID Test?
The Penn Medicine news release said the RAPID technology can be adapted to detect other viruses, including those that cause Influenza and sexually-transmitted diseases.
Robert Michel, Editor-in-Chief of Dark Daily and its sister publication The Dark Report, said the test points to one silver lining in the COVID-19 pandemic. “Researchers around the world intensified their work to find ways to identify the SARS-CoV-2 virus that are faster, cheaper, and more accurate than the diagnostic technologies that existed at the time of the outbreak. In this regard, the COVID-19 pandemic may have accelerated the development and refinement of useful diagnostic technologies that will disrupt long-established methods of testing.”
Marcelo Der Torossian Torres, PhD, postdoctoral researcher at Penn Medicine and lead author of the study, said in the news release, “Quick and reliable tests like RAPID allow for high-frequency testing, which can help identify asymptomatic individuals who, once they learn they are infected, will stay home and decrease spread.
“We envision this type of test being able to be used at high-populated locations such as schools, airports, stadiums, companies—or even in one’s own home,” he added.
Clinical laboratory managers may want to stay current on the development and possible commercialization of the RAPID 1.0 (Real-time Accurate Portable Impedimetric Detection prototype 1.0) biosensor test by the research team at Penn Medicine.