Clinical laboratories should use this situation as an opportunity to ask questions about their own data privacy approaches
While the drama surrounding 23andMe’s bankruptcy announcement has taken the spotlight—cofounder Anne Wojcicki resigned as CEO so that she can attempt to be the top bidder for the company in bankruptcy court—the more interesting long-term debate for clinical laboratories may be about genetic data privacy.
The 20-year-old direct-to-consumer genetic testing company stated in an investor news release on March 23 that it would enter bankruptcy to get a better handle on operational and financial challenges.
In a post on LinkedIn, Wojcicki wrote, “If I am fortunate enough to secure the company’s assets through the restructuring process, I remain committed to our long-term vision of being a global leader in genetics and establishing genetics as a fundamental part of healthcare ecosystems worldwide.”
Wojcicki also heralded the 15 million people who sent in their samples and became customers. Many of them also agreed to clinical research based on those submissions. “What made so many of our innovations possible were the 85% of our customers who opted in to research,” she wrote.
“I have resigned as CEO of the company so I can be in the best position to pursue the company as an independent bidder,” said Anne Wojcicki (above), cofounder of 23andMe, wrote on LinkedIn. It remains to be seen how 23andMe’s bankruptcy will affect clinical laboratories. (Photo copyright: Wikimedia Commons.)
Customer Data Can Be Sold as an Asset During Bankruptcy
Those samples now find themselves in a murky area involving genetic data privacy. Will a court allow creditors to acquire that data as an asset to satisfy 23andMe’s financial obligations? And will people who gave samples to a company they presumably trusted be happy if that information ends up in other hands?
“Comprehensive data privacy legislation has been enacted across the United States and globally, including the California Consumer Privacy Act of 2018 and the European Union’s General Data Protection Regulation,” the Harvard Law Review noted in a March 2025 story about data assets during bankruptcy. “With this development has come a renewed focus on data privacy in bankruptcy, where a debtor is likely to sell its customer data to pay its debts.”
In fact, California Attorney General Rob Bonta, JD, urged residents in that state to consider the California law’s options in light of the bankruptcy announcement. “I remind Californians to consider invoking their rights and directing 23andMe to delete their data and destroy any samples of genetic material held by the company,” Bonta said in a statement.
The Harvard Law Review noted that federal law allows for the appointment of ombudsmen in bankruptcy cases to protect consumer data, but that approach “has been ineffective at meeting that goal.” There is no word at this early stage whether the 23andMe bankruptcy will involve an ombudsman.
How Did 23andMe End Up in Bankruptcy?
Business models and criminals helped push the once thriving 23andMe to the point of bankruptcy. The company in 2021 had a $6 billion market cap. As of close of business on March 24, 2025, the cap hovered just over $20 million.
One long-term issue: There was often no need for anyone to be a repeat customer of 23andMe once they purchased their initial direct-to-consumer genetic test. “It didn’t really have a continuing business model—once you’d paid for your DNA report, there was very little for you to return for,” the BBC reported on Nov. 2.
Clinical labs are clearly in a better position here, as in addition to one-off genetic tests, they offer many medical assays that need to happen dozens or more times over a patient’s life.
Also, 23andMe had a difficult time gaining momentum for its anonymized DNA database that clinical researchers could use, according to the BBC.
A year later, 23andMe agreed to pay $30 million to settle a lawsuit over the stolen data, Reuters reported. The hack accessed information for 6.9 million customers.
Clinical Laboratories Must Be Wary of Genetic Data Privacy
It’s not hard to imagine clinical laboratories that perform genetic testing finding themselves in a situation similar to 23andMe with genetic data privacy on the line because of a business transaction. Some clinical laboratories do go bankrupt, but a more common occurrence is for a lab to be bought out by a competitor or one of the large national laboratory companies.
Clinical lab leaders may want to ask themselves these questions about genetic data privacy:
If a lab’s genetic testing information changed owners, would that damage parties’ reputation in the community?
Is there a triage plan in place to deal with any customers who want their data erased prior to any acquisition or merger?
Watch for in-depth analysis about the implications to clinical labs from the 23andMe bankruptcy in an upcoming issue of The Dark Report. Not a subscriber? Try a 14-day free trial today.
Pathologists and clinical laboratories will play a key role in collecting the data needed to create a person’s digital twin
Digital twins is a promising new technology that is making a big impact in healthcare. This development is significant because clinical laboratory test results will be among the most important sets of data to go into the creation of a patient’s “digital twin.”
A digital twin is defined by IBM as “a virtual representation of an object or system designed to reflect a physical object accurately. It spans the object’s lifecycle, is updated from real-time data, and uses simulation, machine learning, and reasoning to help make decisions.”
“We define a digital twin for healthcare as a virtual representation of a person which allows dynamic simulation of potential treatment strategy, monitoring and prediction of health trajectory, and early intervention and prevention, based on multi-scale modeling of multi-modal data such as clinical, genetic, molecular, environmental, and social factors, etc.,” wrote the authors of a review article published in NPJ Digital Medicine titled, “Digital Twins for Health: A Scoping Review.”
“The concept of digital twin for health (DT4H) holds great promise to revolutionize the entire healthcare system, including management and delivery, disease treatment and prevention, and health well-being maintenance, ultimately improving human life,” wrote study lead Eva Katsoulakis, MD (above), clinical informaticist and radiation oncologist at Tampa General Hospital in Florida, et al, in a review article she and her team published in NPJ Digital Medicine. Clinical laboratory test data will be a key element in the creation of a patient’s digital twin. (Photo copyright: Tampa General Hospital.)
Development of Digital Twins
Something akin to digital twins was first used in 1960 at NASA when replicas of spacecrafts currently on a mission in space were duplicated and studied on Earth. In 1991, Michael Grieves introduced the concept to manufacturing while at University of Michigan’s College of Engineering. The technology was later coined “digital twins” by John Vickers, a principal technologist in advanced manufacturing at NASA in 2010, IBM noted.
The increased use of digital twins in healthcare has brought some brilliant advancements. Examples, as reported by Computer Weekly, include:
Surgery and treatment: Boston Children’s Hospital uses digital twins to examine the complexities of heart procedures in reference to oxygen, blood flow, and valve pressure. Real-time analysis helps with surgeries and treatments, allowing clear visualization at all angles.
Metabolic analysis to tackle kidney failures: Digital twins are being used in Singapore to “Replicate metabolic fluxes to predict chronic kidney disease in type 2 diabetes mellitus.” Doctors there hope to curb the spike of chronic kidney disease found in type 2 diabetes mellitus. Their country has seen cases double in the last 40 years.
Bacterial predictions, E. coli: Bacteria behavior is being analyzed in computational simulations as part of a Simulating Microbial Systems (SMS) program. Run by the US Defense Advanced Research Projects Agency, the “SMS seeks interdisciplinary, comprehensive, and integrated workflows to generate unknown parameters from new data to inform computational models that can predict E. coli.”
Full body data: Precisely personalized care is the goal of European Virtual Human Twins Initiative, a project from the European Commission. The group creates digital twins and updates them with an individual’s personal conditions and health information that shifts as they age, keeping prevention as a focal point.
Respiratory viral pathogens: The complexities and variety of causes behind respiratory infections makes it an ideal area for digital twins. Its use in hospital ICUs can help doctors consider pneumonia treatment outlooks and develop plans for spread of infection.
Pharmaceuticals: Many pharma companies are opting to use digital twins since drug development is highly expensive and animal testing does not always provide clear data compared to human testing. Examples include Orion Pharma, which paired with AstraZeneca and Bayer to create digital twins that “capture genetic and molecular interactions that causally drive clinical and physiological outcomes.” Immunology company, Sanofi, also is using digital twins as “an essential first step to improve efficacy and safety.”
Future of Digital Twins in Healthcare
While digital twin development within healthcare is still in early stages, it promises to pioneer much change.
“When you have this model, you can personalize with certain features, certain anatomy, then you can try things. In heart surgery, you can’t try 20 different things, you only have one shot,” Ellen Kuhl PhD, professor of engineering and bioengineering at Stanford University, told Computer Weekly.
As technology advances and personalized healthcare continues to trend, it is likely digital twins will have a long-term place in medical practices. Astute clinical laboratory professionals will watch the expansion of this trend, since lab data will play such a key role in its development.
Study shows clinical laboratories may one day use nanorobotic tests to help prevent spread of viral infections, cancer, and other diseases
Scientists from the University of Illinois Urbana-Champaign (U of I) have developed a tiny robotic “hand” made from structural DNA that “grabs” viruses—including the COVID-19 coronavirus—potentially preventing them from infecting cells. Such a nano-robotic antiviral technology could be used by anatomic pathologists and clinical laboratory managers in the future as a point-of-care type of test.
This is yet another example of out-of-the-box thinking by developers of diagnostic technology. Led by Xing Wang, PhD, professor of bioengineering and of chemistry at the U of I, the scientists dubbed their DNA device the NanoGripper.
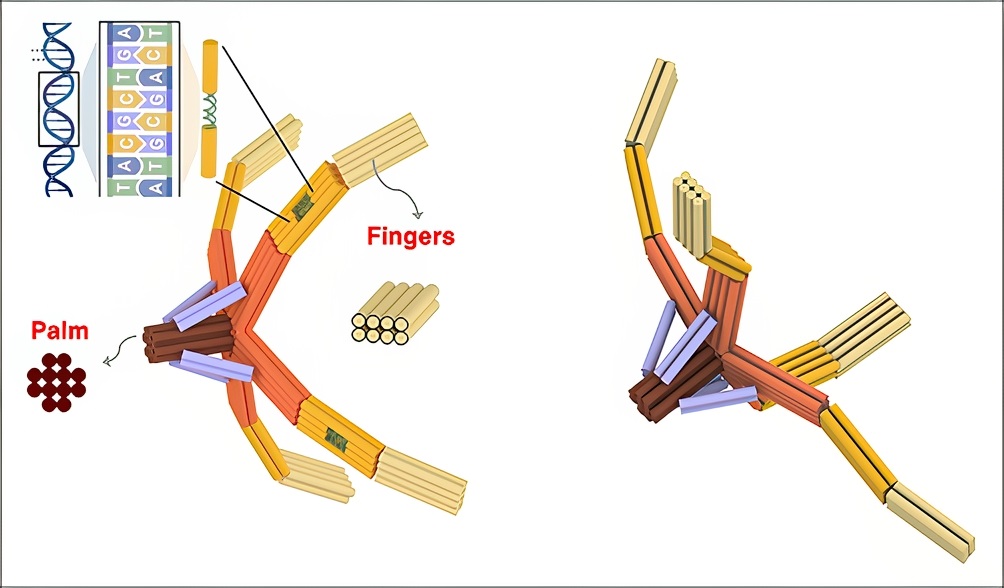
Similar to a piece of origami (Japanese art of folded paper), the so-called hand has “four bendable fingers and a palm, all in one nanostructure folded from a single piece of DNA,” according to a U of I news release. The scientists found in their study that the hand was capable of doing a rapid test to identify the (COVID-19) virus and “prevented the viral spike proteins from infecting the cells,” Gizmodo reported.
“We are using DNA for its structural properties. It is strong, flexible, and programmable. Yet even in the DNA origami field, this is novel in terms of the design principle. We fold one long strand of DNA back and forth to make all of the elements, both the static and moving pieces, in one step,” said Wang in the news release.
“It would be very difficult to apply it after a person is infected, but there’s a way we could use it as a preventive therapeutic,” said Xing Wang, PhD (above), associate professor, bioengineering and chemistry, University of Illinois Urbana-Champaign, in a news release. “We could make an anti-viral nasal spray compound. The nose is the hot spot for respiratory viruses, like COVID or influenza. A nasal spray with the NanoGripper could prevent inhaled viruses from interacting with the cells in the nose.” Clinical laboratories may one day perform antiviral testing that uses U of I’s NanoGripper technology. (Photo copyright: University of Illinois.)
How a DNA Nanorobot Grabs a Virus
The U of I researchers wanted to leverage what has been discovered about DNA as a “material for constructing versatile nanorobots for biomedical applications,” they wrote in Science Robotics. However, previous studies had not achieved the current origami design of a nanoscale mechanism, the authors added.
With robotic precision and its DNA structure, the researchers’ NanoGripper moves and enables fingers to bend for “customized interactions with target molecules,” Interesting Engineering reported, adding that the technology also:
Employed DNA aptamers on the fingers which act as “molecular locks” to find and bind to specific targets.
In a demonstration, wrapped its fingers around the target spike protein of the COVID-19 coronavirus, essentially “disabling its ability to infect cells.”
“The aptamers are arranged into a spatial pattern that specifically matches that of the trimeric spike protein on the virus outer surface. Such pattern recognition-enabled multivalent interaction—a principle developed by my group—has induced ultrahigh NanoGripper virus-binding avidity, resulting in enhanced virus diagnosis sensitivity,” Wang said.
Taken from the U of I news release, the image above shows how “Inspired by the gripping power of the human hand and bird claws, the researchers designed the NanoGripper with four bendable fingers and a palm, all in one nanostructure folded from a single piece of DNA. Each finger has three joints, like a human finger, and the angle and degree of bending are determined by the design on the DNA scaffold.” Such nano-robotic technology could become a new clinical laboratory test for diagnosing viral infections, or even a preventative treatment if caught prior to infection. (Photo and caption copyright: University of Illinois.)
Developing a Test for COVID-19
The scientists discovered that when equipped with a photonic crystal sensor, NanoGripper detected the SARS-CoV-2 coronavirus in 30 minutes with sensitivity equal to RTqPCR tests, Gizmodo reported.
“The NanoGripper functions as a highly sensitive biosensor that selectively detects intact SARS-CoV-2 virions in human saliva with a limit of detection of 100 copies per milliliter, providing a sensitivity equal to that of reverse transcription quantitative polymerase chain reaction [RTqPCR],” the authors wrote in Science Robotics.
In fact, the NanoGripper test is reportedly faster and easier than RTqPCR testing, which requires sophisticated instruments.
“Our test is very fast and simple since we detect the intact virus directly,” said study collaborator Brian Cunningham, PhD, professor, electrical and computer engineering and bioengineering at U of I, in the news release.
“When the virus is held in the NanoGripper’s hand, a fluorescent molecule is triggered to release light when illuminated by an LED or laser,” he said, adding, “When a large number of fluorescent molecules are concentrated upon a single virus, it becomes bright enough in our detection system to count each virus individually.”
More Research and Applications
Gizmodo compared the NanoGripper to a “true Swiss army knife,” able to change and detect other viruses such as HIV and influenza (Flu).
The U of I researchers have already studied the NanoGripper’s ability to detect hepatitis B and plan to publish findings soon, Wang told The Pathologist. He also noted it’s possible the NanoGripper “can be integrated with a lateral flow assay paper strip platform for development of a rapid, sensitive, and inexpensive at home or point-of-care virus detection.”
There is “power in soft nanorobotics,” said Wang, who envisions potential for the NanoGripper beyond viruses to include programming the fingers to detect cancer markers and enabling the grippers to deliver treatment to target cells.
Clinical pathologists and laboratory managers may want to follow this research coming out of the University of Illinois Urbana-Champaign. Once put through additional clinical studies, such nanorobotic diagnostic technology might eventually be used at the point-of-care to help prevent viral infection and spread of disease.
Strikes could lead to delays or cancelations of as many as 123,000 clinical laboratory test across the nation’s healthcare system
Once again, New Zealand medical laboratory workers are returning to the picket line. On March 6, APEX, a specialist union representing more than 4,000 allied, scientific, and technical health professionals throughout New Zealand, issued a strike notice to “three corporate laboratory companies—Awanui, Pathlab, and Medlab,” according to an APEX news release.
“Over 850 laboratory scientists and technicians across New Zealand will take rolling strike action over seven days beginning on 22 March, with at least 123,000 patient tests impacted. Over 70% of New Zealand towns and cities including Tauranga, Rotorua, Palmerston North, Gisborne, Wellington and Dunedin will lose access to medical laboratory testing for their public hospital, or primary care system, or both for a minimum of 72 hours,” the news release notes.
“Pathlab staff across Waikato, Bay of Plenty and Taupō will strike from March 24 until March 26, Awanui staff in Wellington and Canterbury will strike from March 25 until March 27, and Medlab workers in the MidCentral region will strike for a full week from March 22 until March 28. Auckland and the West Coast are the only regions where no labs are affected,” The Post reported.
“Those who use and rely on laboratory services need to brace for impact. We estimate that over 123,000 tests normally carried out as part of urgent or routine patient testing will not be performed during the week of strikes,” said Deborah Powell, MBChB, APEX National Secretary, in the news release.
“We are keen to work with the laboratory employers to resolve this dispute,” said Deborah Powell, MBChB (above), APEX National Secretary, in the news release. “Patients, clinicians, and laboratory workers are now stuck between the rock of underfunding and the hard place of corporate ownership of the medical laboratory sector. To avoid these rolling strikes, we need all parties to the dispute to work together to come up with a creative and sensible solution which works for everyone.” Clinical laboratories in the US may want to pay close attention to the struggles of their counterparts in New Zealand. (Photo copyright: New Zealand Doctor.)
Private Lab Ownership versus Public Funding
In February, more than 900 New Zealand medical laboratory workers nationwide walked off the job to protest “poor conditions and a lack of pay parity with the public sector,” according to the Otago Daily Times. Until now, that was the latest labor action in the ongoing struggle.
But those walkouts did not produce the results the union organizers had hoped.
“We didn’t get what we wanted at all,” Pathlab Tauranga senior medical laboratory scientist Steven Clements told NZ Herald. “We feel like there’s a lot of blame being passed between our employer and the government.”
Clements claimed the New Zealand government made its “standard statement” about it not being involved in private laboratory negotiations.
“They actually provide almost all of our funding, so we feel like the government hasn’t particularly listened. We also feel like our employer maybe isn’t really supporting us … so it’s led to another strike,” he said.
“We are in the weird situation where the employers agree with us,” said APEX National Secretary Powell, NZ Herald reported. “Pay parity between public and corporate employed lab scientists and technicians is the only fair, just, and sustainable solution to this dispute. Unfortunately, the lab triopoly are refusing pay parity without further government funding,” she added.
Disruptions in Care
As is the case with any strike, they are disruptive. During the February strikes, NZ Pathology Chairman, Peter Gootjes, DPH, director of the Awanui Group, told the New Zealand Doctor that they were trying to minimize any disruptions. The New Zealand Association of Pathology Practices (NZ Pathology), according to the organization’s website, is the “collective voice of New Zealand’s private sector laboratory providers, representing the views and aspirations of the funded pathology sector.”
“Our laboratories play an essential role in the provision of healthcare services, and we are working closely with the union, hospitals, and health professionals to ensure essential life-preserving services remain available and ongoing disruption to the community can be minimized,” Gootjes told New Zealand Doctor.
“Pathology sits at the heart of modern healthcare,” he continued. “Ensuring New Zealanders have access to quality, reliable, efficient and trusted pathology services is vital to patient care and public health. These services are a fundamental, yet often unseen, component of the clinical pathway for patients.
“We understand the concerns raised by APEX members and recognize the challenges posed by pay discrepancies following the previous government’s pay equity settlements for public sector employees. We are committed to working constructively with government and officials on this matter,” he said.
Pathlab, Health NZ Respond
In separate statements, Pathlab and Health NZ-Te Whatu Ora (New Zealand’s primary publicly funded healthcare system) attempted to address the APEX lab workers’ demands and assure the public.
“We value [APEX workers’] work and have engaged with APEX in good faith, doing everything we can within the funding we receive. … The problem is that private laboratories, including Pathlab, receive the vast majority of their funding through long-run bulk-funded contracts with Health NZ that pre-date the settlement and are inflexible when it comes to unforeseen cost increases, such as this one,” Pathlab’s chief executive Brian Millen stated, adding, “We remain committed to finding a workable solution while continuing to provide the high-quality services our communities rely on,” NZ Herald reported.
Health NZ, which, according to NZ Herald, “was aware Apex members were in collective bargaining … [but] not involved in this as they did not employ the private sector workforce,” sought to ensure that the strikes’ impact on hospitals and community healthcare services would be minimal.
“All our hospitals and emergency departments will remain open, and we are liaising with the private laboratories to ensure patients who require urgent and critical care receive the services they need, including testing carried out at hospitals and in the community,” said Health NZ, adding, “We respect the right of workers to take strike action and any questions about this matter should be directed to the employers or the union.”
Dark Daily has covered these ongoing strikes in many previous ebriefings. Clinical laboratory and pathology professionals in the United States should take note of their New Zealand counterparts’ recent and ongoing struggle for fair pay and safe working environments. America is no stranger to issues like these and our lab workers could find themselves in a similar situation.
Research could lead to new biomarkers for clinical laboratory tests that spot disease early in patients
As we have covered in previous Dark Daily ebriefs, there are ongoing efforts to develop diagnostic assays that use human breath as the specimen. One early example was the breath specimen for Helicobacter pylori (H. pylori) testing—the bacteria that causes peptic ulcers—in the 1990s. Thus, a new sensor developed by scientists at Zhejiang University in China that can detect the presence of lung cancer in human breath will be of interest to medical laboratory scientists and clinical laboratories working on such testing.
In a proof-of-concept study, the Zhejiang University researchers “developed ultrasensitive nanoscale sensors that in small-scale tests distinguished a key change in the chemistry of the breath of people with lung cancer,” according to an American Chemical Society (ACS) news release.
The new research exemplifies how instruments are becoming increasingly sensitive to detection of smaller specimen quantities, making it possible to even use exhaled breath to diagnose lung cancer, noted a review article published in Science Direct.
“This study presents a novel Pt@InNiOx [platinum (Pt), indium (In), nickel (Ni)] nanoflake isoprene sensor that achieves an exceptionally low limit of detection at two parts per billion (2ppb)—the lowest reported for isoprene sensor to date,” wrote study lead author, Pingwei Liu, PhD (above), distinguished research fellow, Zhejiang University, et al, in ACS Sensors. “Our work not only provides a breakthrough in low-cost, noninvasive cancer screening through breath analysis but also advances the rational design of cutting-edge gas sensing materials.” Clinical laboratories working with breath sample biomarkers will be intrigued by this new advancement in the technology. (Photo copyright: Zhejiang University.)
Finding the Breakthrough Sensor
The Zhejiang University researchers were motivated by the potential for rapid gas sensing in diagnostics. Many gases, including carbon dioxide, are exhaled. But one particular gas, isoprene, they found “can indicate the presence of lung cancer,” the news release states.
However, while breath is readily available, it is not easy to isolate breath biomarkers. That is because a detector needs to “differentiate between volatile chemicals, withstand the natural humidity of exhaled breath, and detect tiny quantities of specific chemicals,” New Atlas explained.
To detect small specimen quantities of isoprene, a highly sensitive sensor needed to be developed—one that would be a step up from standard indium oxide-based breath sensors.
The scientists experimented with a series of indium (III) oxide (In203)-based nanoflake sensors until they found the sensor that performed consistently in nine experiments. They called it Pt@InNiOx for the platinum (Pt), indium (In), and nickel (Ni) it contained.
According to the news release, the Pt@InNiOx sensor:
Had “sensitivity that far surpassed earlier sensors” as evidenced by detection of isoprene as low as 2ppb.
Emphasized isoprene attraction over other volatile compounds in breath.
Has advanced sensitivity due to “Pt nanoclusters uniformly anchored on the nanoflakes” activating the isoprene sensing.
Gadget Review described the innovation as a “significant advance in diagnostic capability” that uses nanoscale technology along with “indium oxide nanoflakes with platinum-based nanoclusters.”
Developing the Lung Cancer Diagnostic Device
The scientists put their Pt@InNiOx nanoflakes into a portable sensing device for breath analysis. They then inserted breath samples from 13 people including five who had lung cancer. They found that:
In samples from people with cancer, the device enabled detection of isoprene levels lower than 40 ppb.
In samples from cancer-free participants, the device found isoprene levels more than 60 ppb.
“We integrate these ultrasensitive Pt@InNiOx nanoflakes into a miniaturized portable electronic device that successfully distinguishes lung cancer patients with expiratory isoprene below 40ppb, from the healthy population with isoprene above 60 ppb, enabling an accurate diagnosis in clinics,” wrote study lead author, Pingwei Liu, PhD, distinguished research fellow, Zhejiang University, et al, in ACS Sensors.
“As the isoprene hits the nanoflakes, electron release is sparked in a way that can be measured,” MSN Health reported, adding that the nanoflakes were also able to find isoprene in other chemicals and operate even in humid conditions.
Breath as Lab Test Biomarker for Cancer
In the United States, more people die from lung cancer than any other form of cancer, according to US Centers for Disease Control and Prevention statistics. The CDC data show there were 209,500 new lung and bronchus cancer cases in 2022, the most recent year for available data.
The Zhejiang University scientists reportedly plan to continue their research on the sensing materials and link between isoprene and lung cancer.
Studies continue to show many components in human breath can be used as clinical laboratory test biomarkers. Assays that use the breath as specimen may one day play an important role in early diagnosis of lung cancer and other diseases.
Researchers find neanderthal blood did not evolve and may have contributed to their demise
Researchers out of France have identified a unique antigen in red blood cells that may have contributed to the downfall of Neanderthals, according to an article in Live Science. These findings will be of interest to clinical laboratorians in hospitals who operate blood banks and blood bankers who do daily testing for blood groups and specific antigens.
“We showed that all Neanderthal shared the same blood group profile,” Mazières told Discover magazine. “Such low diversity is the signal of small populations.” He added, “the study shows how different blood types can help fight against infectious disease,” and that, “it emphasizes the importance of monitoring blood during both transfusions and pregnancies. The presence of some rare subtypes that originated with the Neanderthals but outlived them can lead to complications,” Discover reported.
Clinical laboratories and pathologists will appreciate these new findings, as this unique look into Neanderthal physiology illustrates how the importance of proper blood typing has endured throughout time.
“For any case of inbreeding of a Neanderthal female with a Homo sapiens or Denisova male, there is a high risk of hemolytic disease of the newborn. The condition can lead to jaundice, severe anemia, brain damage and death. This could have contributed to the demise of the Neanderthal population,” Stéphane Mazières, PhD (above), a population geneticist at Aix-Marseille University who led the study into why Neanderthals did not survive, told Live Science. Clinical laboratories that run blood banks and perform blood type testing will find the study results interesting. (Photo copyright: X, formerly Twitter.)
‘Incompatible Blood Type
Mazières’ team studied ancient genomes to further understand the evolution from Neanderthals and Denisovans to Homo Sapiens. Genome sequencing was used to look at blood groups from “dozens of people who lived between 120,000 and 20,000 years ago.” This uncovered “a rare blood group that could have been fatal to their newborns,” Live Science reported.
The rare blood type discovered was not compatible with either Denisovans or early Homo Sapiens. Additionally, the more diverse blood found in Homo Sapiens may have attributed to a more robust immunity, Discover reported.
“Nowadays, certain blood groups confer an advantage against pathogens such as cholera, malaria, one of the gastroenteritis viruses and, as we’ve seen recently, COVID. We can therefore imagine that the blood groups found in the first Sapiens may have equipped them with a new arsenal to face the new environments encountered as they spread across the world,” Mazières told Discover.
“The contribution of this study is twofold. It enlightens the expansion patterns of Homo Sapiens and recalls the anthropological effectiveness of genetic polymorphisms currently being surveyed for transfusion safety and pregnancy monitoring,” the researchers wrote in Scientific Reports.
Knowing a patient’s blood type is key to ensure immune system acceptance of the blood, leading to successful blood transfusions and preventing fatalities. Focus is given to Rh (Resus) factor’s positive and negative typing and on the antigens responsible for segregating A, B, and O blood types. In the case of Neanderthals, a look at red blood cells was key, Live Science noted.
Modern-day Rh incompatibility, which can occur when an Rh-negative woman is pregnant with an Rh positive fetus, can be discovered during pregnancy and treated with prenatal administration of lab-made immunoglobulin to prevent hemolytic disease of the newborn, Live Science reported. It’s a whole system of healthcare that was certainly not available in Neanderthal times.
“Neanderthals have an Rh blood group that is very rare in modern humans. This Rh variant—a type of RhD, another red blood cell antigen—is not compatible with the variants the team found in the Denisovans or the early Homo Sapiens in their study,” Mazières told Live Science.
Looking Ahead
While this research may not change the way blood is handled today, the new findings serve as a reminder of just how important and varied antigens in human blood type can be and how significant the variances impact individuals. It also provides a window into how subtle differences shape the way civilization grows.
The complexity of red blood cells remains an area worthy of continued research, especially since many of these surface and internal antigens are passed down through generations, Live Science noted.
Also, study results may further the decades-long attempt to create artificial blood that has both an extensive shelf life and is accepted by the immune systems of many different patients. However, that will be a daunting challenge. Over the decades, blood bankers and clinical laboratory scientists have watched many attempts to develop artificial blood come close but fail to demonstrate safety while delivering benefits to patients.