Although it is a non-specific procedure that does not identify specific health conditions, it could lead to new biomarkers that clinical laboratories could use for predictive healthcare
Researchers from the Mayo Clinic recently used artificial intelligence (AI) to develop a predictive computational tool that analyzes an individual’s gut microbiome to identify how a person may experience improvement or deterioration in health.
Dubbed the Gut Microbiome Wellness Index 2 (GMWI2), Mayo’s new tool does not identify the presence of specific health conditions but can detect even minor changes in overall gut health.
Built on an earlier prototype, GMWI2 “demonstrated at least 80% accuracy in differentiating healthy individuals from those with any disease,” according to a Mayo news release. “The researchers used bioinformatics and machine learning methods to analyze gut microbiome profiles in stool samples gathered from 54 published studies spanning 26 countries and six continents. This approach produced a diverse and comprehensive dataset.”
“Our tool is not intended to diagnose specific diseases but rather to serve as a proactive health indicator,” said senior study author Jaeyun Sung, PhD (above), a computational biologist at the Mayo Clinic Center for Individualized Medicine: Microbiomics Program in the news release ease. “By identifying adverse changes in gut health before serious symptoms arise, the tool could potentially inform dietary or lifestyle modifications to prevent mild issues from escalating into more severe health conditions, or prompt further diagnostic testing.” For microbiologists and clinical laboratory managers, this area of new knowledge about the human microbiome may lead to multiplex diagnostic assays. (Photo copyright: Mayo Clinic.)
Connecting Specific Diseases with Gut Microbiome
Gut bacteria that resides in the gastrointestinal tract consists of trillions of microbes that help regulate various bodily functions and may provide insights regarding the overall health of an individual. An imbalance in the gut microbiome is associated with an assortment of illnesses and chronic diseases, including cardiovascular issues, digestive problems, and some cancers and autoimmune diseases.
To develop GMWI2, the Mayo scientists provided the machine-learning algorithm with data on microbes found in stool samples from approximately 8,000 people collected from 54 published studies. They looked for the presence of 11 diseases, including colorectal cancer and inflammatory bowel disease (IBS). About 5,500 of the subjects had been previously diagnosed with one of the 11 diseases, and the remaining people did not have a diagnosis of the conditions.
The scientists then tested the efficacy of GMWI2 on an additional 1,140 stool samples from individuals who were diagnosed with conditions such as pancreatic cancer and Parkinson’s disease, compared with those who did not have those illnesses.
The algorithm gives subjects a score between -6 and +6. People with a higher GMWI2 score have a healthier microbiome that more closely resembles individuals who do not have certain diseases.
Likewise, a low GMWI2 score suggests the individual has a gut microbiome that is similar to those who have specific illnesses.
Highly Accurate Results
According to their study, the researchers determined that “GMWI2 achieves a cross-validation balanced accuracy of 80% in distinguishing healthy (no disease) from non-healthy (diseased) individuals and surpasses 90% accuracy for samples with higher confidence,” they wrote in Nature Communications.
Launched in 2020, the original GMWI (Gut Microbiome Wellness Index) was trained on a much smaller number of samples but still showed similar results.
The researchers tested the enhanced GMWI2 algorithm across various clinical schemes to determine if the results were similar. These scenarios included individuals who had previous fecal microbiota transplants and people who had made dietary changes or who had exposure to antibiotics. They found that their improved tool detected changes in gut health in those scenarios as well.
“By being able to answer whether a person’s gut is healthy or trending toward a diseased state, we ultimately aim to empower individuals to take proactive steps in managing their own health,” Sung said in the news release.
The Mayo Clinic team is developing the next version of their tool, which will be known as the Gut Microbiome Wellness Index 3. They plan to train it on at least 12,000 stool samples and use more sophisticated algorithms to decipher the data.
More research and studies are needed to determine the overall usefulness of Mayo’s Gut Microbiome Wellness Index and its marketability. Here is a world-class health institution disclosing a pathway/tool that analyzes the human microbiome to identify how an individual may be experiencing either an improvement in health or a deterioration in health.
The developers believe it will eventually help physicians determine how patients’ conditions are improving or worsening by comparing the patients’ microbiomes to the profiles of other healthy and unhealthy microbiomes. As this happens, it would create a new opportunity for clinical laboratories to perform the studies on the microbiomes of patients being assayed in this way by their physicians.
Though the cost of clinical laboratory testing is not highlighted in KFF’s annual survey, it is a component in how much employers pay for healthcare plans for their employees
Employers now pay higher health insurance premiums than ever for family coverage. However, because of the current tight labor market, they are generally absorbing much of that increase rather than passing the higher costs on to their workers. That’s one key takeaway from KFF’s 26th annual Employer Health Benefits Survey, which the non-profit published on Oct. 9, 2024. While the report does not comment specifically about the cost of clinical laboratory testing or genetic testing and how they may contribute to rising insurance costs, it stands to reason they are part of growing healthcare costs for corporate health benefits.
The KFF survey found that premiums for family coverage increased 7% in 2024, reaching an average of $25,572. That follows a 7% increase in 2023. “Over the past five years—a period of high inflation (23%) and wage growth (28%)—the cumulative increase in premiums has been similar (24%),” KFF stated in a press release.
However, the amount paid by workers has gone up by less than $300 since 2019. It now stands at an average of $6,296, a total increase of 5% over five years. On average, workers covered 25% of family premium costs in 2024, down from 29% in 2023. Workers with single coverage paid an average of $1,368—16% of the annual premium cost—compared with 17% in 2023.
“Employers are shelling out the equivalent of buying an economy car for every worker every year to pay for family coverage,” KFF President and CEO Drew Altman, PhD (above), said in a press release. “In the tight labor market in recent years, they have not been able to continue offloading costs onto workers who are already struggling with healthcare bills.” Rising costs of clinical laboratory testing is always part of the mix contributing to increased worker insurance premiums for employers. (Photo copyright: KFF.)
HDHP/SO plans, as defined by KFF, “have a deductible of at least $1,000 for single coverage and $2,000 for family coverage and are offered with an HRA [Health Reimbursement Arrangement] or are HSA [health savings account]-qualified.” Point-of-service plans “have lower cost sharing for in-network provider services and do not require a primary care gatekeeper to screen for specialist and hospital visits,” the report states.
Cost Sharing via Deductibles
Average deductible amounts—which KFF identified as another form of cost-sharing—varied depending on the type of plan, employer size, and whether the worker had family or single coverage.
For workers with single coverage, average deductibles across all plan types rose from $1,655 in 2019 to $1,787 in 2024, a total five-year increase of about 8%. The average in 2023 was $1,735. These numbers were for in-network providers.
The report noted that some family plans calculate deductibles using an aggregate structure, “in which all family members’ out-of-pocket expenses count toward the deductible,” whereas others use a separate per-person structure. The report includes breakdowns of average deductibles across all types.
Who Offers the Best Benefits?
In general, the KFF report found that large companies—defined as those with 200 or more workers—tend to offer more generous health benefits than smaller ones. Virtually all large companies (98%) offered health benefits, while slightly more than half of small companies (53%) do so.
Among companies that do offer health benefits, the average deductible at a small firm was $2,575 compared to $1,538 at large firms. Among workers with family coverage, the average contribution toward overall premium costs was $7,947 (33%) at small firms compared to $5,697 (23%) at large firms. Among workers with single coverage, the numbers were $1,429 (16%) at small firms compared to $1,204 (14%) at large firms.
The report also found variations in overall premiums and health benefits across nine different industries. For example, healthcare firms paid the highest premiums for family coverage—an average of $26,864—followed by transportation/communications/utilities at $26,601. Companies in agriculture, mining, and construction paid the lowest premiums, an average of $22,654.
There were wide variations by industry in terms of how many firms offer any health benefits. Among state and local government entities, 83% offered health benefits, followed by transportation/communications/utilities (69%), manufacturing (65%), wholesale (62%), healthcare (58%), and finance (56%). Just 40% of retail businesses and 49% of agriculture/mining/construction businesses offered health benefits.
Health Screening Coverage
The KFF report did not include data about insurance coverage for clinical laboratory services. However, one section did address employer willingness to provide opportunities for health screening.
Among large businesses, 56% offered health risk assessments, in which individuals answer questions about their medical history, lifestyle, and other areas relevant to their health risks. A smaller number (44%) offer biometric screening, which “could include meeting a target body mass index (BMI) or cholesterol level, but not goals related to smoking,” the report said. Only 9% of small businesses offered biometric screening, the report found.
KFF conducted its survey between January and July 2024 among a random selection of public and private employers with at least three workers. The survey excluded federal government entities but included state and local government. A total of 2,142 employers responded.
Inflation during this current administration definitely hit consumers in the health insurance premium pocketbook. At the same time providers raised their own prices making it more expensive for people with HDHPs to come up with the cash required by their annual deductible. While clinical laboratory and genetic testing are not highlighted in KFF’s survey, they certainly play a role in increasing costs to healthcare consumers and are worth considering.
New clinical laboratory test could replace conventional spinal tap for diagnosing neurodegenerative disease
In a proof-of-concept study, University of Pittsburgh (Pitt) scientists validated a clinical laboratory test that measures more than 100 different genetic sequences associated with Alzheimer’s disease. The Pitt researchers believe the new diagnostic platform could help clinicians “capture the multifaceted nature of Alzheimer’s pathology and streamline early disease diagnostics,” according to a news release.
Clinical laboratory blood tests that detect biomarkers such as phosphorylated tau protein (pTau) have emerged in studies as diagnostic possibilities for Alzheimer’s disease, which is traditionally diagnosed using a lumbar puncture (spinal tap) procedure.
In their paper, neuroscientist Thomas Karikari, PhD, Assistant Professor of Psychiatry at University of Pittsburgh, lead author of the study, and his research team acknowledged that progress has been made in detecting Alzheimer’s disease with blood-based biomarkers. However, they note that “two key obstacles remain: the lack of methods for multi-analyte assessments and the need for biomarkers for related pathophysiological processes like neuroinflammation, vascular, and synaptic dysfunction.”
The Pitt scientists believe the focus on so-called “classical Alzheimer’s blood biomarkers” limits exploration of neurodegenerative disease.
“Alzheimer’s disease should not be looked at through one single lens. Capturing aspects of Alzheimer’s pathology in a panel of clinically validated biomarkers would increase the likelihood of stopping the disease before any cognitive symptoms emerge,” said neuroscientist Thomas Karikari, PhD (above), Assistant Professor of Psychiatry, University of Pittsburgh, and lead author of the study in a news release. Should further studies prove Pitt’s research sound, clinical laboratories may have a replacement test for diagnosing neurodegenerative disease. (Photo copyright: University of Pittsburgh.)
On its website, Alamar Biosciences explains that the disease panel offers neurological researchers:
“Multiplexed analysis of 120 neuro-specific and inflammatory proteins from 10 µl of plasma or CSF (cerebrospinal fluid).
Detection of “critical biomarkers—including pTau-217, GFAP (glial fibrillary acidic protein), NEFL (neurofilament light polypeptide) and alpha-synuclein.”
The NULISAseq test works with “a proprietary sequential immunocomplex capture and release mechanism and the latest advances in next-generation sequencing,” according to the company.
Inside Precision Medicine noted that the Alamar Biosciences assay enabled Pitt scientists to detect:
Biomarkers (usually found in CSF) “correlating with patients’ amyloid positivity status and changes in amyloid burden over time,” and,
Biomarkers including “neuroinflammation, synaptic function, and vascular health, which had not previously been validated in blood samples.”
“The performance of the NULISA platform was independently validated against conventional assays for classic Alzheimer’s biomarkers for each sample. Biomarker profiles over two years were also compared with imaging-based measures of amyloid, tau, and neurodegeneration,” LabMedica reported.
Opportunity to Track Alzheimer’s
Karikari sees the diagnostic platform being used to track individuals’ blood biomarker changes over time.
In their Molecular Neurodegeneration paper, the Pitt researchers wrote, “These (results) were not limited to markers such as pTau217, p-Tau231, p-Tau181, and GFAP, the elevation of which have consistently shown strong associations with brain Aβ [amyloid beta] and/or tau load, but included novel protein targets that inform about the disease state of the individual in different pathological stages across the biological Alzheimer’s disease continuum.”
About seven million Americans are affected by Alzheimer’s disease, according to the Alzheimer’s Association, which estimated that figure will grow to 13 billion by 2050.
Further studies by Karikari may include larger samples and greater diversity among the people studied, Inside Precision Medicine noted.
“[Karikari’s] lab is developing a predictive model that correlates biomarker changes detected using NULISAseq with brain autopsy data and cognitive assessments collected over the course of several years. Their goal is to identify blood biomarkers that can help stage the disease and predict its progression, both for decision-making around clinical management and treatment plans,” the Pitt news release states.
The Pitt scientists have developed a multiplex test that works with 100 different genetic sequences associated with Alzheimer’s. Such advances in the understanding of the human genome are giving scientists the opportunity to combine newly identified gene sequences that have a role in specific disease states.
In turn, as further studies validate the value of these biomarkers for diagnosing disease and guiding treatment decisions, clinical laboratories will have new assays that deliver more value to referring physicians and their patients.
Small handheld device uses sound waves to detect certain clinical laboratory biomarkers in blood samples
University of Colorado Boulder researchers have developed a novel technology that uses sound waves to test for biomarkers in blood samples. In addition to being very easy to use, the handheld device is portable, highly sensitive, and delivers results in minutes. Though not ready for clinical use, this is yet another example of how researchers are developing faster diagnostic tests that can be performed in near-patient settings, and which do not have to be done in core laboratories, shortening time to answer.
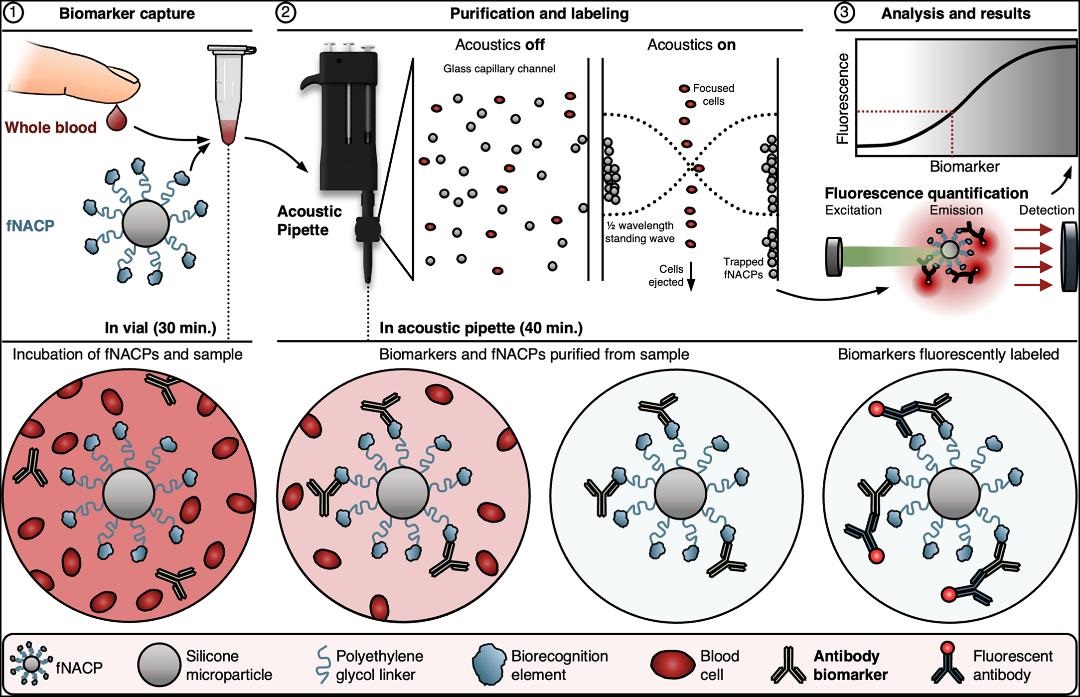
The small instrument—referred to as an “acoustic pipette”—delivers sound waves to tiny particles within the device called “functional negative acoustic contrast particles” (fNACPs). These particles are cell-sized balls that can be customized with different coatings to identify specific biomarkers—such as viruses or proteins—in tiny blood samples, according to a news release.
To operate the device, the custom fNACPs are mixed with a drop of blood and then placed inside the acoustic pipette. The mixture is then blasted with sound waves, which forces particles carrying certain biomarkers to one side of the chamber where they are trapped while the rest of the blood is expelled. The captured biomarkers are then labeled with fluorescent tags and examined with lasers to determine how much of a specific biomarker is present.
“We’re basically using sound waves to manipulate particles to rapidly isolate them from a really small volume of fluid,” said Cooper Thome (above), PhD candidate in Chemical and Biological Engineering at UC Boulder and first author of the study in a news release. “It’s a whole new way of measuring blood biomarkers,” he added. Should further studies validate this approach, clinical laboratories may be able to use this technology to perform diagnostic tests with smaller volumes of patient samples. (Photo copyright: University of Colorado Boulder.)
Blood Testing Quickly and in Multiple Settings
To test their invention, the UC Boulder researchers examined antibodies against a protein called ovalbumin, which is found in egg whites and often used in the development of various vaccines. The scientists discovered that their device could detect the antibodies even in low amounts.
Current rapid tests known as lateral-flow assays can detect specific biomarkers in blood or urine samples but cannot determine how much of the biomarker is present. Enzyme-linked immunotherapy assays (ELISA), the leading clinical laboratory blood test, requires expensive equipment and can take hours to days for results to be received.
With UC Boulder’s new handheld device, tiny blood samples collected from a single finger prick could ensure accurate test results are available quickly at the point of care as well as outside of traditional healthcare settings. This would greatly benefit people in developing nations and underserved communities and may help ease test anxiety for individuals who are apprehensive about traditional blood tests.
“We’ve developed a technology that is very user friendly, can be deployed in various settings, and provides valuable diagnostic information in a short time frame,” said Wyatt Shields IV, PhD, Assistant Professor, Department of Chemical and Biological Engineering, UC Boulder, and senior author of the research in the news release.
“In our paper, we demonstrate that this pipette and particle system can offer the same sensitivity and specificity as a gold-standard clinical test can but within an instrument which radically simplifies workflows,” he added. “It gives us the potential to perform blood diagnostics right at the patient’s bedside.”
The graphic above, taken from UC Boulder’s published paper, illustrates how “fNACPs capture target biomarkers from whole blood samples. fNACPs are purified from blood components by acoustic trapping and captured biomarkers are labeled with a fluorescent antibody within the acoustic pipette. fNACP fluorescence is then measured to determine biomarker presence and concentration.” (Graphic/caption copyright: University of Colorado Boulder.)
Not Like Theranos
The authors of the UC Boulder study are cognizant of some skepticism surrounding the field of biosensing, especially after the downfall of Theranos. The scientists insist their technology is different and based on systematic experiments and peer-reviewed research.
“While what they (Theranos) claimed to do isn’t possible right now, a lot of researchers are hoping something similar will be possible one day,” said Thome in the news release. “This work could be a step toward that goal—but one that is backed by science that anybody can access.”
The device is still in its initial proof-of-concept stage, but the UC Boulder scientists have applied for patents for the apparatus and are searching for ways to scale its use and expand its capabilities.
“We think this has a lot of potential to address some of the longstanding challenges that have come from having to take a blood sample from a patient, haul it off to a lab, and wait to get results back,” Shields noted.
More research, studies, and regulatory reviews will be needed before this technology becomes available for regular, widespread use. But UC Boulder’s new blood testing device is another example of a research team using novel technology to test for known biomarkers in ways that could improve standard clinical laboratory testing.
Clinical laboratory executives and pathology leaders may want to develop strategies for supporting the growing numbers of at-home screening and diagnostic test users
Findings of a national poll conducted by the University of Michigan (U-M) exploring consumers’ purchases suggests seniors are becoming more comfortable with ordering and using at-home medical testing. Their choice of tests and opinions may be of interest to clinical laboratory executives, pathologists, and primary care physicians considering programs to support self-test purchasers.
The researchers found that 48% of adults, ages 50 to 80, purchased at least one at-home medical test, and that 91% of the buyers indicated intentions to purchase another test in the future, according to a U-M news release.
In their paper, they note that “validity, reliability, and utility of at-home tests is often uncertain.” Further, understanding and responding to test results—especially since caregivers may not have ordered them—could lead to “a range of unintended consequences,” they wrote.
“As a primary care doctor, I would want to know why my patient chose to take an at-home test that I didn’t order for them. We also need to understand in greater detail why folks use at-home tests instead of traditional means, beyond convenience,” said the U-M study’s lead author Joshua Rager, MD, a research scientist at William M. Tierney Center for Health Services Research at Regenstrief Institute, who is now an assistant professor of medicine, Indiana University, in a news release. The findings of the U-M study will be of interest to clinical laboratory executives and pathology leaders. (Photo copyright: Regenstrief Institute.)
Free COVID-19 Tests Ignite At-Home Testing
In their Journal of Health Care paper, the U-M researchers speculate that curiosity in at-home testing may have been propelled by the offer of free COVID-19 tests by the US government starting in 2021 during the pandemic.
They also noted the different ways at-home test kits are performed by healthcare consumers. Some, such as COVID-19 rapid antigen tests, return results to users in a few moments similar to pregnancy tests. Others involve self-collecting specimens, such as a stool sample, then sending the specimen to a clinical laboratory for analysis and results reporting to physicians.
Of those older adults who participated in U-M’s National Poll on Healthy Aging study, the following bought at-home medical tests online or from pharmacies and supermarkets, according to U-M’s paper:
As to perceptions of at-home medical testing by users, when polled on their test experience, the surveyed seniors reported the following:
75.1% perceived at-home medical tests to be more convenient than conventional medical tests.
59.9% believe the tests “can be trusted to give reliable results.”
54.8% believe the tests “are regulated by government.”
66% called them a “good value.”
93.6% indicated results “should be discussed with my doctor.”
Inconsistency in how people shared test results with their healthcare providers was a concern voiced by the researchers.
“While nearly all patients who had bought an at-home cancer screening test shared the results with their primary care provider, only about half of those who tested for an infection other than COVID-19 had. This could have important clinical implications,” the researchers wrote in their paper.
Confusion over Government Regulation
The U-M study also revealed consumer misunderstanding about government regulation of at-home clinical laboratory tests purchased over-the-counter.
The US Food and Drug Administration (FDA) cleared “some diagnostic at-home tests for over-the counter use. But many tests on the market are unregulated or under-regulated,” the authors wrote, adding, “Our results suggest, however, that patients generally believe at-home tests are regulated by government, but a substantial minority did not, which may reflect public confusion in how at-home testing is regulated.”
Women, College-Educated Buy More At-Home Tests
Purchase of at-home tests varies among groups, as follows, the news release noted:
56% and 61% of older adults with a college degree or household income above $100,000, respectively, were “much more likely” to buy at-home tests than people in other income and education brackets.
87% of women would buy at-home tests again compared with 76% of men.
89% of college-educated people would purchase the tests again, compared with 78% of people with high school educations or less.
Future U-M research may explore consumers’ awareness/understanding concerning federal regulations of at-home testing, Rager noted.
“At-home tests could be used to address disparities in access to care. We hope these findings will inform regulators and policymakers and spark future research on this topic,” he said in the news release.
The U-M Institute for Healthcare Policy and Innovation survey results confirm that the country’s senior generations are becoming comfortable with at-home and self-testing options. As Dark Daily has previously suggested, clinical laboratories may want to develop service offerings and a strategy for supporting patients who want to perform their own lab tests at home.
“Previously … CDC developed tests for emerging pathogens and then shared those tests with others, and then after that, commercial labs would develop their own tests,” Shah told CNN. “That process took time. Now with these new arrangements, commercial labs will be developing new tests for public health responses alongside CDC, not after CDC.”
In a news release announcing the contract, ARUP Laboratories also characterized the move as a shift for the agency.
“The new contract formalizes ARUP’s relationship with the CDC,” said Benjamin Bradley, MD, PhD, medical director of the ARUP Institute for Research and Innovation in Infectious Disease Genomic Technologies, High Consequence Pathogen Response, Virology, and Molecular Infectious Diseases. “We continue to expand our capabilities to address public health crises and are prepared to scale up testing for H5N1, or develop other tests quickly, should the need arise.”
“To be clear, we have no evidence so far that this [bird flu] virus can easily infect human beings or that it can spread between human beings easily in a sustained fashion,” Jennifer Nuzzo, DrPH (above), Director of the Pandemic Center and Professor of Epidemiology at Brown University School of Public Health, told CNN. “If it did have those abilities, we would be in a pandemic.” Clinical laboratory leaders will recall the challenges at the CDC as it developed its SARS-CoV-2 test early in the COVID-19 pandemic. (Photo copyright: Brown University.)
Missouri Case Raises Concerns
The first human infection of HPAI was reported in late March following a farmer’s “exposure to dairy cows presumably infected with bird flu,” the CDC stated in its June 3, 2024, bird flu Situation Summary. That followed confirmation by the USDA’s Animal and Plant Health Inspection Service (APHIS) of an HPAI outbreak in commercial poultry flocks in February 2022, and the CDC’s confirmation of the first known infections in dairy herds reported on March 25, 2024.
Concerns about the outbreak were heightened in September following news that a person in Missouri had been infected with the virus despite having no known contact with infected animals. CNN reported that it was the 14th human case in the US this year, but all previous cases were in farm workers known to be exposed to infected dairy cattle or poultry.
In a news release, the Missouri Department of Health and Senior Services (DHSS) revealed that the patient, who was not identified, was hospitalized on Aug. 22. This person had “underlying medical conditions,” DHSS reported, and has since recovered and was sent home. Both DHSS and the CDC conducted tests to determine that the virus was the H5 subtype, the news release states.
At present, the CDC states that the public health risk from the virus is low. However, public health experts are concerned that risks could rise as the weather gets cooler, creating opportunities for the virus to mutate “since both cows and other flu viruses will be on the move,” CNN reported.
Concerns over CDC Testing and FDA Oversight
In the months immediately following the first human case of the bird flu virus, Nuzzo was among several public health experts sounding an alarm about the country’s ability to ramp up testing in the face of new pathogens.
“We’re flying blind,” she told KFF Health News in June, due to an inability to track infections in farmworkers. At that time, tests had been distributed to approximately 100 public health labs, but Nuzzo and other experts noted that doctors typically order tests from commercial laboratories and universities.
KFF reported that one diagnostics company, Neelyx Labs, ran into obstacles as it tried to license the CDC’s bird flu test. Founder, CEO, and lead scientist Shyam Saladi, PhD, told KFF that the federal agency had promised to cooperate by facilitating a license and a “right to reference” CDC data when applying for FDA authorization but was slow to come through.
While acknowledging the need for testing accuracy, Greninger contended that the CDC was prioritizing caution over speed, as it did in the early days of the COVID-19 pandemic. “The CDC should be trying to open this up to labs with national reach and a good reputation,” he told KFF.
Another problem, KFF reported, related to the FDA’s new oversight of laboratory developed tests (LDTs), which is causing labs to move cautiously in developing their own tests.
Jennifer Nuzzo, DrPH (above), Director of the Pandemic Center and Professor of Epidemiology at the Brown University School of Public Health co-authored a June 2024 analysis in Health Affairs that called on the CDC to develop “a better testing playbook for biological emergencies.” The authors’ analysis cited earlier problems with the responses to the COVID-19 and mpox (formerly known as monkeypox) outbreaks.
If global surveillance networks have detected a novel pathogen, the authors advise, the US should gather information and “begin examining the existing testing landscape” within the first 48 hours.
Once the pathogen is detected in the US, they continued, FDA-authorized tests should be distributed to public health laboratories and the CDC’s Laboratory Response Network (LRN) laboratories within 48 hours.
Advocates of this approach suggest that within the first week diagnostics manufacturers should begin developing their own tests and the federal government should begin working with commercial labs. Then, within the first month, commercial laboratories should be using FDA-authorized tests to provide “high throughput capacity.”
This may be good advice. Experts in the clinical laboratory and healthcare professions believe there needs to be improvement in how novel tests are developed and made available as novel infectious agents are identified.