New report notes that variations in price for common clinical laboratory tests should not exist ‘regardless of clinical setting’ and yet they do
Hospital laboratory leaders may soon observe employers—especially those in seven particular states—shopping around a bit more when it comes to insurance coverage of clinical laboratory tests for their employees. That’s because a recent study by the Health Care Cost Institute (HCCI ) found that employer-sponsored insurance pays three to six times more for lab tests performed by hospital outpatient labs compared to lab tests done by physician offices and independent clinical laboratories.
In an issue brief it developed in conjunction with West Health, the HCCI revealed that standard clinical laboratory tests cost as much as six times more when performed through hospital outpatient lab outreach programs rather than physician offices in Colorado, Indiana, Nevada, New Mexico, North Carolina, Texas, and West Virginia.
“Among individuals with employer-sponsored insurance, we observe substantially higher prices paid for common lab tests when these tests were billed by hospital outpatient departments (including on- and off-campus locations) compared to when they were performed in physician offices and independent labs,” the report authors wrote.
HCCI is a Washington, DC-based non-profit research institute focused on issues impacting the US healthcare system. West Health, in Washington, DC, and San Diego, is a nonprofit group that works to lower healthcare costs for seniors.
“By their very nature, [clinical laboratory] tests are standardized to be the same regardless of clinical settings, yet our research finds that hospital outpatient departments are typically billing private insurance three times more for the same lab test compared to physician offices and independent laboratories,” wrote Cristina Boccuti, MA, MPP, Director of Health Policy at Health West in the HCCI report. (Photo copyright: West Health.)
Price Markups Vary by Clinical Laboratory Test Type
In their HCCI issue brief, Cristina Boccuti, MA, MPP, Director of Health Policy at Health West; Senior Researcher and doctoral candidate Jessica Chang; and Aditi P. Sen, PhD, Director of Research and Policy at Health Care Cost Institute, wrote, “In this brief, we compare prices (as determined by total payments on claims) for clinical lab tests between hospital outpatient departments (25% of tests in our study) and physician offices and independent labs (75% of tests in our study) among individuals with employer-based health insurance.
“This analysis,” they added, “uses HCCI’s unique commercial claims dataset, which contains claims for 55 million Americans annually. In addition to analysis of individual clinical lab tests, we also examined variation across five broader categories following previously established methods relying on [Current] Procedural Terminology (CPT) codes.”
Those five test categories and percentage of samples studied included:
Clinical Chemistry (54%)
Microbiology (24%)
Complete blood count (10%)
Urine (9%)
Toxicology (4%)
Price markups (a calculated ratio based on each setting’s median price) varied by type of medical laboratory test and were usually three to five times higher in a hospital outpatient setting as compared to the physician office or independent clinical lab site. Some urine tests were more than seven times higher.
“Variation should not exist among clinical lab tests,” the HCCI authors wrote. “Analysis of most non-emergent clinical lab tests on a specimen, such as a blood test or urine sample, is identical regardless of factors such as where the test is performed or patient risk.”
The most frequently ordered lab tests with the highest markup included:
Urinalysis (automated with microscopy): $2.72 office/independent lab; $21.39 hospital outpatient (more than seven times price markup).
Comprehensive metabolic panel: $8.85 office/independent lab; $47.13 hospital outpatient (more than five times markup).
General health panel: $22.97 office/independent lab; $127.97 hospital outpatient (more than five times markup).
“Under commercial insurance, some hospital outpatient departments are being paid over $200 for a metabolic panel, which has a medical office-based price of (about) $9,” the HCCI report noted.
Medical Laboratory Test Prices All Over the Map
When HCCI explored clinical laboratory test pricing throughout the US, the researchers found price markups in hospital outpatient settings ranging two to six times higher than the same lab tests performed in offices and independent labs. States with low markups were North Dakota, Arkansas, and Minnesota.
Markups varied within states as well. The HCCI analysts shared an example of lipid profile testing in Pennsylvania, where the average price difference between hospital outpatient and physician offices ranged from $34 in Philadelphia to just $17 in Pittsburgh.
Big Differences in Microbiology, Toxicology Lab Test Prices
As to clinical laboratory testing categories, the report found the greatest price markups were in blood count and urine testing. The biggest median price differences—more than $30 per test—was observed in microbiology and toxicology:
Blood count: $6.34 in office/independent lab versus $29.61 in hospital outpatient setting.
Urine: $4.33 office/independent lab versus $24.39 hospital outpatient.
Microbiology: $16.50 office/independent lab versus $47.80 hospital outpatient.
Toxicology: $12.15 office/independent lab versus $43.65 hospital outpatient.
While individual lab test prices may seem low, the overall investment is huge in the context of 232 million lab tests, and spending is increasing. Nearly $7 billion was spent on medical laboratory tests in 2019, as compared to $5.8 billion on 155 billion tests in 2012, HCCI data shows.
Bill Kerr, MD, co-founder and CEO at Avalon, noted in an article he penned for MedCity News that a hospital outpatient laboratory may receive $100 for a routine test, while a non-hospital lab will get on average $20 for the same test on the same instrument.
“Hospitals frequently argue that they need to charge more to support their specialty test innovation and development. That doesn’t hold true for routine testing though,” he wrote.
Kerr pointed out that physicians could order tests as part of incentives to use hospital-affiliated labs. “Plus,” he wrote, “payers are often hesitant to educate their members about lower-cost lab testing options because of various provisions in their contracts with hospitals.”
What could help, he added, are lab testing price transparency and “payment integrity programs,” that have science “at the core” and aim to flag unneeded and as well as needed tests, especially in oncology.
HCCI Advises Site Neutral Payment, Negotiation
HCCI also made recommendations in its report. They include:
Policymakers for states with the high hospital outpatient setting markups “should use site-neutral payment policies for insurance plans regulated at the state level.”
In negotiations, health insurers and self-insured employers can aim to limit site-based payment differentials for their enrollees and employees.
For hospital clinical laboratory leaders, the HCCI is calling attention to an issue that may eventually restrict the ability of hospitals to bill outpatient lab tests using inpatient pricing.
Study may lead to repurposing existing drugs that are proven to be safe for the treatment of related diseases as the interactome becomes the subject of more research efforts
Researchers from multiple scientific institutions working together have begun using the protein interactome to understand what combination of unique biomarkers is a reliable indicator that a specific drug would benefit a patient. Armed with that knowledge, pharmaceutical companies plan to develop a drug that benefits individuals who have that collection of biomarkers/interactome.
Of course, once the drug exists, the next step is to develop a clinical laboratory test that looks for those biomarkers so that patients can be diagnosed and identified as candidates for the new drug treatment.
Microbiologists and clinical laboratory scientists engaged in “omic” studies—such as genomics, proteomics, metabolomics, metagenomics, phenomics, and transcriptomics—know that scientists are increasingly working to use ever-larger numbers of biomarkers to collectively identify if an individual patient would benefit from a specific drug. This ongoing research is at the heart of precision medicine treatments.
“This work bridges many fields of biology, including statistical genetics, cell biology, and bioinformatics,” said Pedro Beltrão, PhD, Professor in the Department of Biology at ETH Zürich’s Institute of Molecular Systems Biology and former group leader at EMBL-EBI. Microbiologists and clinical laboratories engaged in “omic” studies will understand the significance of this study. (Photo copyright: Gulbenkian Science.)
Study Finds Biological Support for Repurposing Existing Drugs
According to Genetics Engineering and Biotechnology News (GEN), “A protein interactome—the network of all possible protein interactions—constitutes an important intermediary step that could bridge the often difficult to cross chasm between genotype [an organism’s complete set of genetic material] and phenotype [an organism’s observable characteristics or traits], and is key in identifying drug targets.”
The scientists discovered more than 1,000 human traits from 21 therapeutic areas, GEN reported. Their process identified drug targets and genes linked to diseases because it pinpoints the shared basis of diseases utilizing a map of interactive human proteins.
The more defined the links are between genetic mechanisms, human traits, and diseases, the more likely their methods can help pharmaceutical companies prioritize those targets for new drugs, and for potentially repurposing existing FDA-approved drugs, the scientists noted.
The study accessed multiple databases including Reactome, Signor, and the EMBL-EBI’s IntAct. The researchers used genome-wide association studies (GWAS) to identify interacting protein groups that were genetically linked.
“The interactome identified some known associations, such as cardiovascular diseases and lipoprotein or cholesterol measurements,” Inigo Barrio Hernandez, PhD, a postdoctoral fellow at Open Targets and EMBL-EBI, told GEN. “But we also found some unexpected associations. For example, the interactome highlighted three protein clusters shared by ten respiratory and skin immune-related diseases. This is hugely exciting because we now have some biological support to repurpose existing drugs that are proven to be safe to treat related diseases.”
The researchers also identified 73 protein clusters linked to more than one trait or disease. This is known as pleiotropy. Pleiotropic relationships are goldmines to drug companies because they show how a therapy for one disease could effectively treat another, and in addition, it provides insight on targets that could trigger side effects, GEN reported.
What Comes Next?
Pedro Beltrão, PhD—Biology Professor at ETH Zürich’s Institute of Molecular Systems Biology and former group leader at EMBL-EBI—noted the significance of this collaborative study. “It brought together groups from across Open Targets and EMBL-EBI and highlights the value of collaborations across disciplines,” he told GEN.
The study researchers plan to continue identifying, mapping, and utilizing their findings for drug development.
“This is an exciting showcase … that has generated an array of new insights for novel target discovery as well as drug repurposing, and informs our understanding of the connection between rare and common diseases through shared biological processes,” Ellen McDonagh, PhD, Director of Informatics Science at Open Targets, told GEN. “This is now being developed further to provide tissue and cell-type specific networks to help further prioritize targets for disease treatment.”
The term “interactome” was coined in 1999, but many microbiologists and clinical laboratory scientists may not be familiar with it. Considering the possibility of new drug therapies based on these newly discovered biomarkers—and the medical laboratory tests that will be needed to identify compatible patients—it’s a good idea to stay aware that protein interactome exists.
Researchers are working to identify the protein interactome, map it, and use it—both in drug discovery and development—as well as in clinical laboratory testing. More research and study is needed, so a medical lab test that advances patient care is a ways off. But the research is worth following.
Provider groups and members of Congress say the rules favor payers, federal judge agrees, but path forward in how providers bill patients remains unclear
Groups representing healthcare providers—including pathologists—are challenging the Biden administration’s implementation of the No Surprises Act, a bill passed in 2020 that aims to protect patients from surprise medical bills.
This will be of particular interest to pathologists who—as a study from the Health Care Cost Institute (HCCI) found—were second only to emergency room physicians among providers with the highest percentage of out-of-network billing.
The College of American Pathologists (CAP) and American Society for Clinical Pathology (ASCP), both of which supported the No Surprises Act, are now among numerous provider groups claiming that the bill’s rules for resolving payment disputes unfairly favor payers.
These groups have bipartisan support in Congress, Bloomberg Law reported, noting that some legislators are urging Health and Human Services (HHS) Secretary Xavier Becerra to change the rules. The lawmakers may seek to amend the law or turn to the courts if Becerra does not follow through on their requests.
“Either we legislate, we go to court, whatever it takes,” Rep. Brad Wenstrup (R-Ohio) told Bloomberg. Meanwhile, a federal district court judge has sided with the Texas Medical Association (TMA) in two lawsuits over the rules, Healthcare Dive reported.
“We need to make sure that the administration is implementing what we passed consistent with the legislative intent,” Sen. Michael Bennet (D-Colorado) told Bloomberg Law regarding the No Surprises Act. “We had a very complicated coalition of people to come together to support this legislation.” (Photo copyright: Senate.gov.)
Details of No Surprises Act
The No Surprises Act aims to protect patients from “balance billing,” in which they receive surprise bills for out-of-network medical services even when they use in-network providers. The bill was signed into law in December 2020, with most provisions taking effect on Jan. 1, 2022.
As Dark Daily reported in “ASCP and CAP Support New Legislation That Bars Surprise Medical Billing,” following passage of the bill, patients who unknowingly receive services from out-of-network providers are liable only for costs they would have incurred for in-network care. Providers and payers then have 30 days to negotiate a payment. If they can’t agree, an arbiter determines the payment as part of a federal independent dispute resolution (IDR) process.
Passage of the bill required the federal Department of Health and Human Services (HHS), Department of Treasury, and Department of Labor to craft regulations and guidance to implement the law—including the IDR process—according to the American Hospital Association (AHA).
Legal Pushback to Arbitration Rule
One contention was an interim rule that instructed arbiters to use the “qualifying payment amount” (QPA) as the primary basis for ruling in favor of either insurers or providers in payment disputes.
Writing in MedPage Today, pediatric radiologist Richard Heller, MD, National Subspecialty Lead for Pediatric Radiology at Radiology Partners in Chicago, and Radiological Society of North America (RSNA) Board Liaison for Public Information and Corporate Relations, described the QPA as “the insurer’s median in-network rate.”
Heller wrote that “the calculation methodology does not result in real world, market-based rates. Further, insurers calculate their own QPA, and may do so in a non-transparent fashion, raising questions about QPA integrity.”
He added, “The departments have repeatedly tried to establish the QPA as the primary factor arbiters should use in their decision making. These attempts have twice been rejected by a federal court. Recent guidance issued by the administration as a result of the second Texas Medical Association lawsuit more closely reflects the balance that Congress intended.”
In its first lawsuit, the TMA characterized the QPA as “an opaque and flawed insurer-calculated amount” that would result in reduced payments to providers. The lawsuit claimed that Congress, instead, intended for the dispute resolution process to look at “a range of factors.”
Federal Judge Jeremy Kernodle ruled in the TMA’s favor and ordered HHS to change the rule. He also sided with the TMA in another lawsuit, which alleged that a final rule issued in August 2022, while “formally abandoning the QPA rebuttable presumption,” unduly restricted use of non-QPA factors, according to a litigation update for certified IDR entities from Sidley Austin LLP.
The final rule “nevertheless continues to place a thumb on the scale for the QPA by requiring arbitrators to begin with the QPA and then imposing restrictions on the non-QPA factors that appear nowhere in the statute,” the judge stated in his ruling, the American Medical Association (AMA) reported.
In its latest lawsuit, the TMA is challenging a big hike in administrative fees for dispute resolution, which went from $50 initially to $350 beginning last January.
Another issue with the law has been the sheer volume of arbitration cases. The administration originally estimated that payers and providers would submit about 17,000 claims per year, but between April 15 and Sept. 30, 2022, about 90,000 disputes were initiated, according to a government report cited by RevCycleIntelligence.
The No Surprises Act reflected lawmaker compromises about arbitration, Sen. Michael Bennet (D-Colorado) told Bloomberg Law. Bennet indicated to the news outlet that he is not happy with the current arbitration process.
Pathology Groups Weigh In
The CAP and ASCP joined other physician organizations in raising early objections to the Biden Administration’s plans to implement the independent dispute process.
“The skewed IDR process outlined within the IFC [Interim Final Rule with Comment Period] will remove a critical incentive for insurers to negotiate reasonable contracts with physicians by establishing the QPA as a reasonable out-of-network payment,” the ASCP stated in a Dec. 6, 2021, letter to administration officials.
On Dec. 23, 2021, the CAP filed an amicus brief in a lawsuit brought by the AMA and AHA challenging an interim rule issued that September. The regulations “must support an equitable and balanced system for resolving out-of-network payment disputes,” said CAP President Emily Volk, MD, FCAP in a statement accompanying the filing. “As of today, the rules heavily favor the insurers when their power is already too great.”
The AMA and AHA later withdrew the lawsuit after the Biden administration revised the rule, Healthcare Finance News reported. However, the groups still contend that the rule favors payers.
High Stakes for Pathologists
When the law passed Congress, it appeared likely it would have a disproportionate impact on medical laboratories and pathology groups. The HCCI report ranked pathology number two among six specialties responsible for the highest percentage of out-of-network bills. And when the interim final rule was published in the Federal Register, the HCCI data was cited in an accompanying commentary.
However, the CAP told The Dark Report that the statistics about pathologists, though accurate, were “presented in a somewhat misleading manner.”
The No Surprises Act does permit balance billing when patients have given prior consent, but pathologists were among a group of specialties barred entirely from the practice, Dark Daily previously reported.
Study may also result in new clinical laboratory tools for determining antimicrobial resistance and efficacy of existing antibiotics
Researchers find it increasingly difficult to develop antibiotics that are effective against strains of bacteria that display antibiotic resistance—a subset of antimicrobial resistance (AMR). However, a new study provides a glimmer of hope and may spur clinical laboratories to look at this research in novel ways.
Conducted at the University of California Santa Barbara, the study looked at more than 500 antibiotic-bacteria combinations. The researchers discovered that several widely used, FDA-approved, antibiotics may be more useful than previously thought against a large range of bacterial infections, said infectious disease specialist Judy Stone, MD, in an article she penned for Forbes titled, “Why Antibiotics Fail—and How We Can Do Better.”
The researchers also discovered a common culture medium that enables a better assessment of the properties of various strains of bacteria to resist different antibiotics.
Clinical laboratories and microbiologists are tasked with plating and growing bugs to identify a specific bug, what strain of bug, and whether that strain has resistance to specific antibiotics. Thus, this research touches on what they do daily. It is something that may provide microbiologists with new approaches to detect AMR more accurately.
“We know there are a variety of reasons why antibiotics don’t work as predicted, from wrongly prescribed doses to infrequent administration, but another less noticeable reason is that lab testing can show a bacteria is susceptible to antibiotics when it’s actually not. You know, the whole in vitro (culture plate) versus in vivo (life) balance,” wrote Judy Stone, MD, infectious disease expert, in her Forbes article. Clinical laboratories may soon have a better way of identifying antibiotic resistance in deadly bacteria. (Photo: LinkedIn profile.)
UCSB Antimicrobial Study Details
Antibiotic-resistant infections are responsible for more than 32,000 deaths in the US and 1.27 million globally every year, Forbes reported. A study like this can have a far-reaching impact.
To conduct their study, Michael Mahan, PhD, Professor of Molecular, Cellular, and Developmental Biology at UCSB, and his team at the Mahan Lab on the UCSB campus, used Fisher Scientific’s Gibco Dulbecco’s Modified Eagle Medium (DMEM), a basal medium for supporting the growth of many different mammalian cells.
The DMEM predicted antibiotic effectiveness better than Mueller Hinton Broth (MHB), another growth medium from Thermo Fisher Scientific that has been used in clinical laboratories by World Health Organization (WHO) decree since 1968, Forbes reported.
Assays were run against 13 isolates from nine species of bacteria to determine the efficacy of 15 different antibiotics. Using DMEM, the team found different sensitivities in 15% of the bacterial isolates tested in vitro compared to MHB.
In Mahan’s follow-up tests, which looked at mice infected with different bacteria, MHB was accurate in 54% of test predictions while DMEM was accurate 77% of the time. Part of the reason, Mahan believes, is because DMEM is more physiologic and closer in conditions to people (in vivo), Forbes reported.
“People are not Petri plates—that is why antibiotics fail. Testing under conditions that mimic the body improves the accuracy by which lab tests predict drug potency,” said Mahan in a UCSB press release.
“I think it has merit. I think this study has been very well-designed … and showed that this makes clinical sense … If it bears out in humans, it will be clinically very significant,” pulmonologist Ken Yomer Yoneda, MD, Professor Emeritus, Department of Internal Medicine at UC Davis Health, told Forbes.
Though the major limitation of the study is that it was conducted on mice and not humans, Yoneda said it gives an indication of potential success with humans. “If it bears out in humans it will be clinically very significant,” he told Stone for her Forbes article.
Rodney Rohde, PhD, Professor and Chair of Clinical Lab Science Program at Texas State University also shared enthusiasm on the findings. According to Stone, “[Rohde] was ‘intrigued’ by the finding that using a physiologic media predicted ‘a change in susceptibility’ thresholds used to categorize patient isolates as susceptible or resistant.
“He was also ‘excited about the results of increasing diagnostic accuracy’ with especially difficult-to-treat organisms,” she noted.
“Rohde added that the issue of these clinical breakpoints—setting the level at which an organism is defined as ‘sensitive’ or ‘resistant’ to an antibiotic is a hot topic, undergoing considerable discussion in lab circles. Multiple agencies need to reach agreement for the standards that are used globally, both in the US and Europe,” Stone wrote.
Old Drug, New Tricks
According to the UCSB press release, “Physicians are aware of the flaws in the gold-standard test [MHB]. When recommended antibiotics do not work, they must rely on their experience to decide on the appropriate antibiotic(s) for their patients. This study provides a potential solution to address the disparity between antibiotics indicated by standard testing and actual patient outcomes.”
Infectious disease physician Lynn Fitzgibbons, MD, remarked in the UCSB press release, “Re-evaluation of FDA-approved antibiotics may be of far greater benefit than the time and cost of developing new drugs to combat antimicrobial resistance, potentially leading to significant life-savings and cost-savings.”
In her Forbes article, Stone wrote, “Pharmaceutical companies are abandoning the acute infectious disease market and few new antibiotics are in sight. Pharma is profit driven and antibiotics are simply not as lucrative as life-style drugs (like Viagra/Cialis or Rogaine for hair loss) or those for chronic diseases. So, Mahan et al.’s findings are welcome news indeed.”
Once further studies validate the UCSB study findings and allow their use in clinical settings for patient care, clinical laboratories and microbiologists may have new tools for accurately determining a bacterium’s ability to resist existing antibiotics or its susceptibility to antibiotics not currently used to treat certain infections.
From some adverse events, clinical laboratory tests may be integrally tied to delays in treatment and faulty care management events that cause patient harm and deaths
Adverse patient safety events are increasing according to The Joint Commission (TJC), a nonprofit US-based organization that accredits tens of thousands of US healthcare organizations and programs. Its 2023 annual report on “sentinel events”—patient safety breaches that can inflict serious harm or death—found that these events jumped by 78.1% from 2020 to 2021 and by 19.3% from 2021 to 2022. These are significant increases. What effect do they have on healthcare providers?
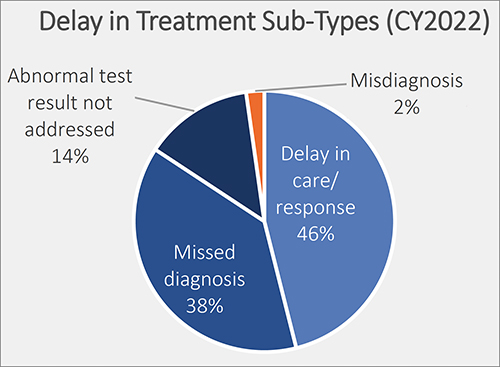
Of particular interest for clinical laboratory managers and pathologists is one finding by TJC involving “delay in treatment” as an adverse event. TJC determined that the cause of 38% of these episodes was due to “missed diagnoses.” It is likely that clinical laboratory test results have some role in this type of adverse event. Thus, this is a potential opportunity for medical lab leaders to add value by helping hospital administrators and physicians reduce the number adverse events tied to missed diagnoses.
Another consequence for hospitals and providers is lost revenue. Medicare will not reimburse care to providers when a medical error, fall, surgery on wrong site, or other “never event” happens, including misdiagnoses due to inaccurate clinical laboratory testing.
Thus, since patient safety is a priority and providers are tasked with reducing medical errors, The Joint Commission’s Office of Quality and Patient Safety has developed the Sentinel Event Database for tracking adverse patient safety events.
The de-identified and aggregate patient data includes “causes and outcomes of sentinel events, is analyzed yearly to help the nation in general—and accredited organizations in specific—gain insight into causes of sentinel events and develop mitigating strategies to prevent harm to individuals under their care,” according to The Joint Commission’s report, “Sentinel Event Data 2022 Annual Review.”
This graphic taken from The Joint Commission’s annual 2023 report on sentinel events shows the percentage of delays in treatment broken out by type. Delays in treatment is the second most common sentinel event, exceeding wrong surgery and medication management, according to The Joint Commission’s report. Only falls exceed delays in treatment, and since 80% of a patient’s health records are clinical laboratory test results, they could play a role in each of these adverse patient safety events. (Graphic copyright: The Joint Commission.)
Most Common Sentinel Events
According to The Joint Commission’s report, “Of reviewed sentinel events in 2022:
“20% resulted in patient death,
“6% in permanent harm or loss of function,
“44% in severe temporary harm, and
“13% in unexpected additional care/extended stay.
“Sentinel events resulting in death were most commonly associated with:
“patient suicide (24%),
“delays in treatment (21%), and
“patient falls (11%).
“Events resulting in severe temporary harm were most commonly associated with patient falls (62%).”
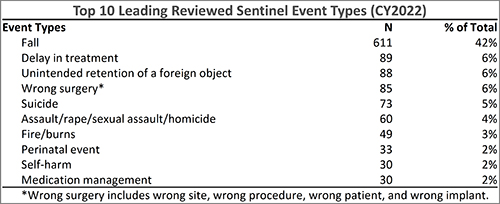
The Joint Commission’s annual 2023 report on sentinel events shows the top 10 sentinel event types in 2022. According to the report, delay in treatment, which could be caused by inaccurate clinical laboratory tests, moved from fourth place in 2018, to third place in 2021, and is now in second place. (Graphic copyright: The Joint Commission.)
National Quality Forum ‘Never Events’
In 2001, Ken Kizer, MD, founding President and CEO of the National Quality Forum (NQF), coined the phrase “never events” to describe often fatal and usually preventable medical errors. Since then, the list of never events, according to PSNet, a national web-based resource of the Agency for Healthcare Research and Quality (AHRQ), has grown to include 29 “serious reportable events” in seven categories:
Surgical or procedural events
Product or device events
Patient protection events
Care management events
Environmental events
Radiologic events
Criminal events
Listed under “Care management events” is “Patient death or serious injury resulting from failure to follow up or communicate laboratory, pathology, or radiology test results.”
In “Hospitals Take Steps to Drive Down Medical Errors in Their Emergency Departments,” Dark Daily wrote how one common source of errors in emergency rooms is lack of information that includes timely access to radiology or clinical laboratory test reports. Moreover, formal process improvement projects to identify and eliminate the sources of errors in emergency rooms can involve the hospital laboratory.
As medical laboratory managers know all too well, the fast-paced environment of a busy emergency room often contributes to errors such as hemolyzed specimens, a delay in transporting the specimen from the ER to the lab, or incomplete patient information on the laboratory test request form as it is received in the hospital laboratory.
‘Stuff of Nightmares‘
In an article he penned for Chicago-based thought leadership and advisory company 4Sight Health, longtime healthcare writer David Burda commented on The Joint Commission’s sentinel events report. He wrote: “Two things scared me from this eight-page report. First, The Joint Commission is publishing statistics and trends in reported sentinel events. How many go unreported? Second, surgeons still are performing the right procedure on the wrong patient or the wrong procedure on the right patient? Isn’t there a checklist to prevent this? The stuff of nightmares.”
Burda went on to note that “88% of the sentinel events in 2022 happened at accredited hospitals, and 90% were self-reported by accredited organizations. Patients, patients’ families, or current/former employees reported 10% of the sentinel events to The Joint Commission.”
The rapid rise of patient adverse safety events should be a concern for all sectors of the healthcare industry. Clinical laboratory managers should be especially concerned since nearly every medical decision precedes or follows a medical laboratory test.
Of 27 BSL-4 labs assessed, Global Biolabs ranked only seven as having ‘good’ biosafety management
In a new report, a research firm assessed the conditions at the handful of laboratories across the world that handle the most dangerous pathogens. In the wake of the SARS-CoV-2 global pandemic, there is heightened awareness of the risks of a lab accident that might release such pathogens into the environment, putting humans at risk.
Medical laboratory scientists working in clinical laboratories worldwide understand the critical nature of biosafety laboratory (BSL) criteria. Nearly all clinical laboratories that test for infectious disease agents are biosafety level-1 and -2 (BSL-1, BSL-2).
Other high-containment laboratories (HCL) that handle deadly, highly transmissible pathogens are typically government-run or university-affiliated. HCL labs have BSL-3 and BSL-4 levels and require rigorous adherence to protocols that ensure worker safety and prevent escape of dangerous pathogens.
Thus, the new report from Global Biolabs, which is critical of biorisk management protocols at existing and planned BSL-4 laboratories—especially given the increasing construction of new HCL labs worldwide—will be of interest to medical technologists, pathologists, and clinical scientists working with highly infectious diseases.
The biosafety experts who make up the Global Biolabs research team conduct risk-assessments and “provide key policy recommendations for strengthening biorisk management in BSL-4 labs,” according to the organization’s website.
“The more labs and people working with dangerous pathogens, the risks go up,” biosecurity expert Filippa Lentzos, PhD (above), Associate Professor, Science and International Security, King’s College London, told Science magazine. Lentzos was part of the team that created the Global Biolabs mapping project two years ago. Clinical laboratory managers may want to review the findings in the Global Biolabs report. (Photo copyright: King’s College London.)
Only Seven Out of 27 Countries Get ‘Good’ Overall Score
“The boom in BSL-4 lab construction appears, so far, not to have been accompanied by strengthened biorisk management oversight,” according to the Global Biolabs 2023 report from the Global Biolabs Initiative. “Additionally, most planned BSL-4 labs will be in countries with relatively low scores for governance and stability,” the report’s authors wrote.
The report included a ranking of countries by total biorisk management score, the Daily Mail noted, adding:
Of 27 countries analyzed, seven ranked as good (above 70%) for biorisk policies,
15 scored medium (above 30%),
five scored below.
Those with the best biorisk management scores (maximum 48):
Canada scored 46 (96%),
US scored 42 (88%),
Australia and the United Kingdom each scored 40 (83%).
Notably, China “scored zero on modifying pathogen rules.” According to the Daily Mail, “China’s overall management score (33) was in the middle of the pack, 69%.”
Associate Professor in Science and International Security, King’s College London, and Gregory Koblentz, PhD, Associate Professor and Director Biodefense Graduate Program, George Mason University, Fairfax, Virginia. The organization tracks maximum containment labs worldwide, noting trends that raise biosafety and biosecurity concerns.
According to the Daily Mail, Lentzos noted “that a particular worrying aspect of the BSL-4 boom was those countries looking to open their first lab were the bottom scorers in terms of good biorisk management.
“Many of the countries building new labs, some for the first time, score poorly on biorisk management. However, there is still time to strengthen national laws and regulations on biosafety, biosecurity, and dual-use research [biological research that could cause harm] to bring them up to international standards,” the Global Biolabs researchers wrote in their report.
Global Mapping of BSL-4 Labs
There are 51 BSL-4 labs operating worldwide, and 18 are planned or under construction, according to Global BioLab’s report. Here’s where they are located:
Europe: 24
North America: 12
Asia: 9
Oceania: 4
Africa: 2
South America: 0
Also, BSL-3+ labs total 55:
Europe: 21
North America: 18
Asia: 10
South America: 3
Africa: 2
Oceania: 1
The report also noted:
Of the 18 BSL-4 labs under construction, 11 are planned to open in Asia.
About half of BSL-4 labs are “less than the size of a tennis court.”
“Eighty percent (of BSL-4 labs) are located in urban areas, which heightens concerns about accidents at these facilities,” Koblentz told the Daily Mail.
According to Science, the number of BSL-4 labs has doubled since 2013. Growth in BLS-4 labs began around the time of the 2001 anthrax attacks and picked up speed in 2003 following the SARS outbreak, University World News reported.
Biosecurity and Biosafety Analyzed
Global Biolabs’ analysis included countries’ biosecurity and biosafety scores. Just 12 out of 27 countries with BSL-4 labs scored high on biosecurity, nine scored medium, and six scored low.
A high score for biosecurity—which US and France received—reflects laws for biosecurity, a national list of dangerous pathogens, and whistleblower protection.
Out of 27 countries, 21 with BSL-4 labs scored high on biosafety. However, two countries scored medium, and four scored low. The two countries that earned the highest scores for biosafety—Canada and Australia—have physical/engineering controls, occupational health, and transportation safety, among other areas reviewed.
Opportunities for Improvement
Global Biolabs made the following recommendations in their report:
Nations with BSL-4 and BSL-3 labs need to have in place biorisk management systems including comprehensive laws, regulations, and institutions that require safety and security risk assessments of proposed research.
Strengthening of biorisk management is called for by the World Health Organization and Biological Weapons Convention.
Labs, of all biosafety levels, are advised to aim toward safety, security, and responsible research.
The effort by Global BioLabs to create a public record of how each BSL-4 and BSL-3 laboratory adheres to strict standards of safety and operations demonstrates that some degree of risk exists in the operation of these labs. Whether government and world health authorities make it a priority to address known deficiencies in those labs is a question yet to be answered.