Study also may have found relationship between atherosclerosis and cholesterol
Chinese scientists have developed a cutting-edge method for non-invasively monitoring blood cholesterol levels in humans. The innovative technology utilizes images of skin on hands and may eliminate the need for both invasive venipunctures and fasting for testing cholesterol. Given the large volumes of blood cholesterol tests currently performed by clinical laboratories, this new technology could have significant impact on cholesterol testing if further studies confirm its capabilities.
Notably, the Chinese researchers have apparently already developed a lab analyzer to perform the procedure and it is being used in clinical care. However, in the United States and other countries, this technology will require additional clinical studies and regulatory review before clinical laboratories would be able to use it in daily patient care.
The cholesterol sensing system consists of a detection reagent associated with a fluorescent group that binds to skin cholesterol, and a detection device. Cholesterol levels are easily obtained from the skin, according to the researchers, by analyzing the manner in which the skin absorbs and scatters light via a scanner.
Should this technology be validated for clinical care, it could replace other invasive clinical laboratory tests for cholesterol measurement.
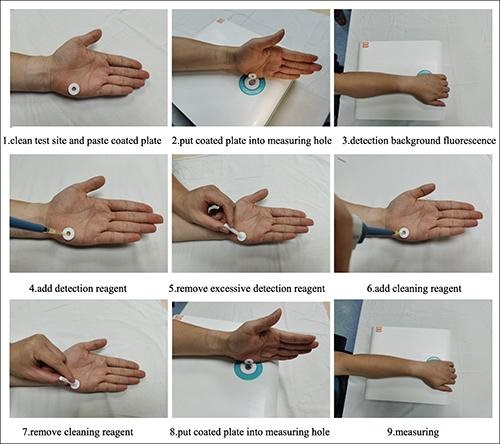
The series of images above, taken from the researchers’ Lipids in Health and Disease published study, demonstrates how their non-invasive clinical laboratory test for total blood cholesterol is performed. Non-invasive clinical laboratory tests for monitoring biomarkers in the blood are always preferred by patients over veinous punctures and fasting. (Photo copyright: Hefei Institutes of Physical Science, Chinese Academy of Sciences.)
First Evidence of Relationship between Cholesterol and Atherosclerosis
“Just put your hands on, and the system will tell you the cholesterol data,” Yikun Wang, PhD, Professor, Department of Physical Sciences, Hefei Institutes of Physical Science, Chinese Academy of Sciences, and leader of the research team, told Diagnostics World. “Cholesterol is one of several types of fats (lipids) that play an important role in human body, we can track your fats in this simple way.”
To perform the testing, clinicians first clean the test site located on the fleshy edge of the palm of the hand with an alcohol swab. A patient’s non-dominant hand is used for the test as the skin on that hand is typically less abrasive and contains fewer melanocytes, which allows for more stable results. A plastic-coated annulus is then applied to the test site and the examined portion is positioned on the measuring hole of the detection system to measure the background light spectrum of the skin.
Once the background signal is ascertained, the detection reagent is added to the annulus until it is full. After 60 seconds, any excess detection reagent is removed from the annulus. A cleaning reagent is then added to the annulus for 30 seconds and removed with a sterile cotton swab. The treated portion of the skin is then placed over the measuring hole of the detection system and two spectrums of light are compared to measure the skin cholesterol, which accurately correlates to the cholesterol in the bloodstream.
“Compared to in-situ detection used in the previous clinical research, our device may offer more accurate results for we can avoid the influence of pressure and skin background differences [person to person],” Wang said. “Study results offer the first evidence of a relationship between skin cholesterol and atherosclerotic disease in a Chinese population, which may be of great significance to researchers around the world.”
Initially, 154 patients diagnosed with acute coronary syndrome (ACS) between January 2020 and April 2021 were involved in the study. However, only 121 of those patients were included in the final study with the remaining being excluded due to at least one of the following criteria:
Severe hepatic (liver) or renal (kidney) insufficiency, and
Obesity.
Clinician Use Can Affect Accuracy of Test
Developed by researchers from the Hefei Institutes of Physical Science Chinese Academy of Sciences, and the University of Science and Technology of China, the researchers noted that how clinicians operate the device can have an impact on the accuracy of the test results.
“A critical step in the [testing] process that is subject to operator variability is blotting, which requires the operator to remove an unbound detector from the palm before adding the indicator,” Wang told Diagnostics World. “Excess residual indicator solution can result in falsely increased skin cholesterol levels. Considering this, we are planning to develop a simplified and standardized blotting procedure.”
Millions of people in the US live with illness that requires regular monitoring of blood cholesterol. Normal total cholesterol should be less than 200 milligrams per deciliter (mg/dL). According to the federal Centers for Disease Control and Prevention (CDC), nearly 94 million US adults over the age of 20 have total cholesterol levels higher than 200 mg/dL and 28 million adults have total cholesterol levels higher than 240 mg/dL. In addition, 7% of children and adolescents between the ages of six and 19 have high cholesterol. For these reasons, cholesterol testing represents a substantial portion of the clinical laboratory tests performed daily in this country.
This new non-invasive technology for monitoring total blood cholesterol in humans could greatly benefit patients, especially if it eliminates the need for venipunctures and fasting prior to testing. Clinical laboratory managers and pathologists may want to follow the progress of this new cholesterol testing technology as it demonstrates its value in China and is submitted for regulatory review in this country.
Clinical laboratories and pathology groups can benefit from knowing how genetic testing is being used for other than medical testing purposes
It is useful for pathologists and clinical laboratory managers to be aware of the different ways genetic testing and DNA sequencing is being conducted. That’s because a genetic test for one purpose—such as identifying an individual’s relatives and connection to a region or a cultural group—might generate data that could become part of that person’s medical care.
Thus, an ongoing genetic study in South Africa highlighting the issue of so-called “helicopter research” will be informative for Dark Daily’s readers.
Also known as “neo-colonial science,” helicopter research describes when scientists from wealthy countries perform research in lower-income countries in ways that may be deemed exploitative or disrespectful to local populations.
“Scientists conduct helicopter research when they collect data from developing countries and marginalized communities with little to no involvement from local researchers and community members,” wrote researchers Dana Al-Hindi, and Brenna Henn PhD, in an article for The Conversation. “Helicopter research also occurs when researchers take data out of the country they collected it from without either providing benefit to or sharing the results with the community.”
In an article for The Conversation, UC Davis researchers Brenna Henn, PhD (left), and Dana Al-Hindi (right), wrote, “While we have learned a great deal from these communities, we have been unable to fulfill a common request: providing them their individual genetic ancestry result. In our attempts to overcome the logistical challenges of providing this information, we’ve grappled with the common question of how to ensure an equitable balance of benefits between researchers and the community they study. What we’ve found is that there is no easy answer.” Clinical laboratories will want to remember the term “Helicopter Research” in relation to these types of studies. (Photos copyright: UC Davis/The Conversation.)
The South Africa study, conducted over the past 12 years, aims to use genetic data “to help unravel the history and prehistory of southern Africans and their relationship to populations around the world,” the authors wrote in The Conversation.
The researchers have been using the genetic data to trace the ancestry of indigenous Khoekhoe and San peoples in South Africa as well as other populations that self-identify as “Colored.”
“Early European colonizers initially used this term to refer to indigenous Khoekhoe and San groups long before it was codified by the apartheid government in 1948,” the researchers wrote. “It persists today as an ethnic category, broadly encompassing Khoe-San groups, various East African, Indian, and Southeast Asian populations brought by the slave trade, and people of mixed ancestry.”
Challenges Sharing Genetic Data with Study Participants
Participants in the study have asked to see their personal genetic ancestry results, but the researchers noted several challenges, including local restrictions and the difficulty of presenting complex data in “an accessible and digestible form.” So, the researchers partnered with consumer-focused genetic testing company 23andMe (NASDAQ:ME).
23andMe provided additional funding for the research, assisted the researchers in community outreach, and “expanded our ability to ‘capacity-build’—that is, to make sure that the knowledge and skills we gain are shared with local institutions,” Henn and Al-Hindi wrote in The Conversation. They added that they are still dealing with questions about whether their efforts to provide equitable benefits are sufficient.
“Our research team, local collaborators, and 23andMe are all concerned about how to best address the risk of helicopter research, coercion, and any unknown risks that may arise from disclosing personal ancestry results,” they wrote.
Cape Town Statement on Fostering Research Integrity
The issue of helicopter research was a major focus at the 7th World Conference on Research Integrity (WCRI), held May 29-June 1 in Cape Town, South Africa. It was the first WCRI to be held in Africa and adopted the theme “Fostering Research Integrity in an Unequal World.”
One outcome of the conference will be an effort to produce what is known as the Cape Town Statement on Fostering Research Integrity. The statement will “highlight the importance of fairness in international research partnerships,” noted Research Professional News.
The statement “compels institutions and researchers alike to act on their responsibilities to promote equity, diversity, and fairness in research partnerships,” conference speaker Retha Visagie, DCur, told the publication. She leads the Research Integrity Office at the University of South Africa.
Conference co-chair Lyn Horn, PhD, director the Office of Research Integrity at the University of Cape Town, told the publication that it could take up to a year before a draft of the statement is ready for comment.
One overarching goal will be to “demonstrate why inequity and unfair practices in research collaborations and contexts is a research integrity (RI) matter,” the authors wrote. “Second it must identify some key values or principles and action guides that will address the issue of equity and fairness in research within the context of the complete research life cycle from research agenda setting and call to proposal development, through grant application, allocation and management of funding, data production, analysis, management and sharing, to outputs, translation, and evaluation.”
Another conference speaker, Francis Kombe PhD, told attendees the statement will offer guidance specifically to institutions such as universities, journals, and funding organizations, the journal Science reported. That stands in contrast to earlier statements on helicopter research, which were geared more toward individuals and small groups.
How any of this will impact clinical laboratories and pathology groups remains unclear. Nevertheless, it is worthwhile knowing how gene sequencing is being used by researchers for purposes other than to guide diagnoses and treatment of patients.
End of social distancing, masking, and other COVID-19 pandemic mitigations may lead to more severe flu-like infections in northern hemisphere, experts say
Clinical laboratory professionals in the United States and Canada should prepare now for a severe flu season. That is according to infectious disease experts at Johns Hopkin’s Center for Health Security who predict the rise in influenza (flu) cases in Australia signals what will likely be higher than normal numbers of flu-like infections starting this fall in the Northern Hemisphere.
As a Southern Hemisphere nation, Australia experiences winter from June through August. The land down under just concluded its worst flu season in five years. The flu arrived earlier than usual and was severe. Surveillance reports from the Aussie government’s Department of Health and Aged Care noted that influenza-like illness (ILI) peaked in May and June, but that starting in mid-April 2022 the weekly number of flu cases exceeded the five-year average.
If the same increase in flu cases happens here, healthcare systems and clinical laboratories already burdened with continuing COVID-19 testing and increasing demand for monkeypox testing could find the strain unbearable.
Amesh Adalja, MD (above), Infectious Disease Expert and Senior Scholar at the Johns Hopkin’s Center for Health Security, told Prevention that Australia’s flu season is typically a harbinger of what will follow in the US, Canada, and other Northern Hemisphere countries. “The planet has two hemispheres which have opposite respiratory viral seasons,” he said. “Therefore, Australia’s flu season—which is just ending—is often predictive of what will happen in the Northern Hemisphere.” Clinical laboratories in the United States should review their preparations as North America enters its influenza season. (Photo copyright: Johns Hopkins Bloomberg School of Public Health.)
Consequences of Decline in Flu Vaccinations and Social Distancing, Masks
The New York Times noted that in 2017, when Australia suffered through its worst flu season since modern surveillance techniques were adopted, the US experienced a deadly 2017-2018 flu season a half-year later that took an estimated 79,000 lives.
While the number of flu cases in this country is currently low, according to the weekly US Centers for Disease Control and Prevention’s (CDC) “Flu View,” that is expected to change as temperatures cool.
During the height of the COVID-19 pandemic in the US, influenza was nearly nonexistent. Pandemic-mitigation efforts such as masking, social distancing, and quarantining slowed the spread of the annual respiratory illness. But pandemic mitigation efforts are no longer the norm.
“Many have stopped masking,” said Abinash Virk MD, an Infectious Diseases Specialist at Mayo Clinic College of Medicine and Science, in a Mayo Clinic news blog that urged patients to get vaccinated for flu. “For the large part, we will see the re-emergence of influenza in the winter. In comparison, in 2020 winter … there was literally no influenza. But now that has all changed.”
Diminished Immunity Will Lead to More Severe Flu Cases
A CDC report published in July also noted that last winter’s flu season broke from the traditional pattern of arrival of the flu in the fall followed by a peak in cases in February.
During the 2021-22 season, influenza activity began to increase in November and remained elevated until mid-June. It featured two distinct waves, with A(H3N2) viruses predominating for the entire season. But the overall case counts were the lowest in at least 25 years preceding the COVID-19 pandemic.
Thomas Russo, MD, Professor and Chief of Infectious Disease at the University at Buffalo in New York, said the past two mild flu seasons could set the stage for a difficult year in 2022-23.
“Immunity to respiratory viruses, including the flu, wanes over time,” Russo told Prevention. “People have not seen the virus naturally for a couple of years and many individuals don’t get the flu vaccine.” That, he says, raises the risk that people who are unvaccinated against the flu will develop more severe cases if they do happen to get infected.
“People are interacting closely again and there are very few mandates,” he added. “That’s a set-up for increased transmission of influenza and other respiratory viruses.”
“The Southern Hemisphere has had a pretty bad flu season, and it came on early,” Fauci, told Bloomberg in late August. “Influenza, as we all have experienced over many years, can be a serious disease, particularly when you have a bad season.”
CNN reported that US government modeling predicts flu will peak this year in early December.
CDC Advises Public to Get Flu Vaccine
Because COVID-19 and Influenza have many symptoms in common, such as fever, cough, shortness of breath, fatigue, sore throat, runny nose, headache, and muscle aches, the Mayo Clinic points out on its blog that testing is the only way to discern between the two when symptoms overlap.
According to the CDC, the best way to reduce risk from seasonal flu and its potentially serious complications is to get vaccinated every year. The best time to get vaccinated for the flu is in September and October before the flu starts spreading in communities, the CDC states. However, vaccination after October can still provide protection during the peak of flu season.
Yet, many people fail to get the flu vaccine even though it is recommended for everyone over the age of six months. CNN reported that just 45% of Americans got their flu shots last season. Flu vaccination rates fell for several at-risk groups, including pregnant women and children.
Though flu seasons are often unpredictable, clinical laboratories should prepare now for an influx of influenza test specimens and higher case rates than the past two pandemic-lightened flu seasons. Coupled with COVID-19 and monkeypox testing, already strained supply lines may be disrupted.
Though only in early stages, findings could lead to a ‘therapeutic against current and newly-arising variants,’ say researchers
As SARS-CoV-2 changes and mutates, some therapeutic antibodies that were once highly effective in fighting the virus have lost potency. But now, in a proof-of-concept study, researchers from Boston Children’s Hospital have identified one antibody that neutralizes all known variants of the coronavirus, including the omicron variant. Microbiologists and clinical laboratory managers will find this intriguing, as most medical labs perform serology testing for SARS-CoV-2 antibodies.
The new antibody appears to be robust. It triggers several other types of antibodies as part of the immune response. If validated by further research, this discovery, the researchers state, may lead to new vaccines, better therapies, and improved treatments for COVID-19.
“We hope that this humanized antibody will prove to be as effective at neutralizing SARS-CoV-2 in patients as it has proven to be thus far in preclinical evaluations,” said geneticist Frederick Alt, PhD, Director of the Program in Cellular and Molecular Medicine at Boston Children’s Hospital and one of the leaders of the research. Clinical laboratories that perform serology testing for COVID-19 will be intrigued by this new line of research. (Photo copyright: PR Newswire.)
SP1-77 Antibody Outperforms All Others at Neutralizing SARS-CoV-2
To conduct their research, the team used genetically modified mice that basically have built-in human immune systems. These mice were originally utilized for seeking out antibodies to HIV, another virus that tends to mutate. Their immune systems can mimic what human immune systems encounter when a viral invader attacks.
The scientists inserted two human gene segments into the mice, which quickly produced antibodies resembling those made by humans. The mice were then exposed to the SARS-CoV-2 spike protein from the original coronavirus strain. The scientists found that the mice produced nine different families of antibodies that could bind to the spike protein.
The researchers then tested the effectiveness of those antibodies and found that three of the nine antibody families strongly neutralized the original SARS-CoV-2 coronavirus. In addition, one of the antibody families—dubbed SP1-77—was much more powerful and could neutralize the Alpha, Beta, Gamma, Delta, and all known Omicron strains of the SARS-CoV-2 virus.
New Monoclonal Antibody Products and Vaccines
If their findings are validated through further research, SP1-77 “would have potential to be a therapeutic against current and newly-arising variants of concern” according to the Science Immunology study. It also could be useful as part of a cocktail containing other antibody treatments for COVID-19 variants.
“SP1-77 binds the spike protein at a site that so far has not been mutated in any variant, and it neutralizes these variants by a novel mechanism,” said Tomas Kirchhausen, PhD, Senior Investigator, Program in Cellular and Molecular Medicine at Boston Children’s Hospital and one of the authors of the study in a statement announcing the study findings. “These properties may contribute to its broad and potent activity,” he added.
“This is very early-stage proof-of-concept work to illustrate that broadly neutralizing antibodies can be generated using a mouse model,” Amesh Adalja, MD, an infectious disease expert and senior scholar at the Johns Hopkins Center for Health Security, told Prevention. “Such work, if replicated and expanded, could form the basis of new monoclonal antibody products as well as a vaccine.”
The researchers have applied for a patent for the SP1-77 antibody as well as the mouse model they used to create it. Studies on the antibody are ongoing and have only been performed on mice and not humans. The scientists intend to execute further research on the innovative antibody and hope it will someday be used to help fight the COVID-19 virus and all its variants.
“We’d love to have a vaccine that is active against all circulating variants, including those yet to come,” Thomas Russo, MD, Professor and Chief of Infectious Disease, Department of Medicine, University at Buffalo told Prevention. “It’s the holy grail of vaccines.”
Microbiologists and clinical laboratories working with monoclonal antibodies to treat for COVID-19 infections will no doubt want to follow the Boston Children’s Hospital research closely as it may lead to new treatments and vaccines.
Testing capacity has been boosted by inclusion of commercial laboratory companies and the fact that the virus spreads less easily than SARS-CoV-2
At the start of the SARS-CoV-2 pandemic, clinical laboratories were unprepared for unprecedented testing volumes. Fast forward to today, and the monkeypox outbreak has some clinical laboratory managers and pathologists wondering if they might again be faced with a surge in demand for monkeypox testing.
The good news is that so far the supply of tests appears adequate, especially compared to the early days of COVID-19.
“We’ve always had more capacity than we have had tests coming in,” Walensky noted. “To date, we’ve used about 14% to 20% of our capacity.”
During a hearing before the Senate Health, Education, Labor, and Pensions Committee on the current state of monkeypox testing capacity in the US, Rochelle Walensky, MD (above), Director at the CDC said, “We worked through commercial labs to expand testing across the country and simultaneously [offered] outreach and education to providers, clinicians, patients, and public health.” At the moment, access to clinical laboratory testing for monkeypox appears stable, but that could change as demand grows. (Photo copyright: CDC.)
Capacity Sits at 80,000 Tests Per Week in the US
When the monkeypox outbreak began, US medical laboratories could run 6,000 tests per week. At the time, this was more than sufficient, according to a White House press briefing.
However, since then, demand for testing has increased across the country to 80,000 tests per week. As part of that effort, the CDC partnered with five commercial laboratories to expand access to testing, according to the federal Department of Health and Human Services (HHS), Dark Daily reported in August.
Testing capacity also has kept up with demand thanks to biology. Monkeypox, which is in the same orthopoxvirus family of viruses as smallpox, has proven far less virulent than COVID-19, so fewer people are getting infected.
FDA Advises Against Monkeypox Saliva Test
Another boost to capacity in the future may come from new types of monkeypox tests.
Wired reported on Aug. 1 that Flow Health—a California company already distributing COVID-19 tests—has developed a monkeypox test that can detect the virus in saliva. This test would require patients to spit into a tube for a sample, and as such could be distributed for at-home use.
However, in a report released on July 15, the US Food and Drug Administration (FDA) advised providers to only take testing samples from lesions caused by the rash associated with monkeypox infection. The FDA stated that there is currently no clinical data to support the use of other monkeypox tests like Flow Health’s.
Monkeypox Testing Resources Scarce in Some Areas
At the moment, clinical laboratory testing capacity seems stable, however, roadblocks are appearing that may disrupt the availability of monkeypox tests for patients.
Although bringing on five commercial laboratories has increased US testing capacity, MedTech Dive reported on Aug. 10 that for some hospitals and laboratories, resources for monkeypox testing are scarce.
“Right now, there’s a lot of confusion in the community about where to get tested, where can people find treatment,” Robert Pitts, MD, an Infectious Diseases Specialist at Bellevue, told MedTech Dive. “There’s just no clear guidance because I think a lot of the different facilities and healthcare systems in New York are still trying to patch together pathways. … We’ve had to borrow space, borrow staff, which has been really, really challenging.”
During August, Bellevue took two primary care providers out of their normal clinical responsibilities to instead focus on monkeypox. And Pitts found himself dedicating four to five hours of his time to monkeypox-related issues, MedTech Dive reported.
“And so, I’m using my own time, because it’s a crisis, to respond to it,” he said.
The US healthcare system has been somewhat more efficient at getting monkeypox tests out to clinical laboratories than was the case with COVID-19. Moreover, new tests may be on the way. However, roadblocks exist that must be overcome to ensure monkeypox testing capability will meet growing demand.
Answers and effective solutions to the lab profession’s most urgent challenges will be front and center at the innovative ‘Lab Management Essentials Workshop’
Three powerful forces are slamming clinical laboratories today. One is the urgent need to cut costs. Second is the struggle to achieve and maintain full lab staffing. Third is the pressure to increase revenue and expand market share.
All of this is happening even as hospitals and health systems must deal with almost identical issues. Cost-cutting, recruiting more staff, and finding ways to increase revenue dominate the thoughts and actions of senior health administrators.
Most Hospitals and Health Systems Report Substantial Financial Losses
News reports about the financial losses at hospitals and health systems tell the story. For example, one report in Becker’s Healthcare described the financial damage at three major, multi-state health systems:
AdventHealth, a 48-hospital health system, reported a $417.7 million net loss in the first quarter of 2022. It reported that, because of inflation, costs had increased by 15% over prior year.
Kaiser Permanente, with 12.6 million members in seven regions of the United States, reported a net loss of $961 million in the first quarter of 2022. One major factor in these losses was the increase in expenses, which was 9.5%. For second quarter 2022, Kaiser Permanente showed a loss of $1.3 billion, most of that from a decline in the value of its investment portfolio.
Ascension Health, with 143 hospitals in 19 states, reported a net loss of $884.7 million in first quarter of 2022. It said its costs increased by 10.6% over the same period last year.
Most hospital-based clinical laboratory managers and pathologist are aware of these staggering financial losses. They also are watching how the shortage of nurses and other skilled personnel has hospitals scrambling to close that gap by paying more overtime, using temporary nurses who are paid at much higher rates, and increasing nurse salaries to prevent existing staff nurses from taking more lucrative offers from other hospitals in the community.
Clinical Laboratories Under Pressure to Cut Costs and Maintain Adequate Staff Levels
Hospital-based laboratories are on the frontline of these hurricane forces. Facing operating losses, hospitals ask their laboratories and other clinical service lines to cut costs below authorized budgets. Meanwhile, the labs themselves must deal with their own shortage of medical technologists (MTs) and clinical laboratory scientists (CLSs)—along with other skilled positions—that are required to provide the full menu of lab testing services.
This “perfect storm” of pressures to cut costs, keep staffing at authorized levels, and generate more revenue (that can offset rising costs of lab supplies and the higher salaries being paid to MTs and CLSs) is without precedent in the past four decades. To provide lab managers with the knowledge to resolve these challenges swiftly and confidently in their own laboratories, the team behind the Executive War College assembled experts to conduct a one-and-a-half-day interactive workshop.
Using Lab Case Studies to Teach Proven Solutions for Reducing Expenses
Each of the three important topics will be addressed in half-day learning modules. Following case study presentations on best practices, attendees at Lab Management Essentials will break out into smaller roundtable groups facilitated by lab industry experts. The groups will brainstorm how to apply these proven methods to cut costs, retain employees, and create revenue. They will then describe their findings to all participants.
Lab Management Essentials Workshop facilitators (clockwise from top left): Tafney Gunderson, Carlton Burgess, Dorothy Martin, Rick VanNess, Jane Hermansen, and Kim Zunker.
On the morning of day one, leaders of the lab cost-cutting module will be:
Carlton Burgess, Vice President of Laboratory Services at Prime Healthcare in Ontario, Calif.
Tafney Gunderson, Quality Systems Supervisor at Avera McKennan Laboratory in Sioux Falls, S.D.
On the afternoon of day one, leaders of the lab staff recruiting, hiring, and retention module will be:
Dorothy Martin, Regional Laboratory Manager at Dartmouth-Hitchcock Health in Lebanon, N.H.
Kim Zunker, MBA, MLS(ASCP), CAPM, Consulting Manager at Accumen in Scottsdale, Ariz.
On the morning of day two, leaders of the lab staff recruiting, hiring, and retention module will be:
Jane Hermansen, MBA, MT(ASCP), Manager of Outreach and Network Development at Mayo Clinic in Rochester, Minn.
Rick VanNess, Director of Product Management at Rhodes Group and TriCore Reference Laboratories in Albuquerque, N.M.
Delivering Essential Knowledge to Up-and-Coming Laboratory Managers
This Lab Management Essentials workshop is a first for the clinical laboratory profession. It brings together experienced, effective lab leaders to teach, guide, and coach your lab’s smartest up-and-coming lab managers. It accomplishes this in just one-and-a-half days, to minimize the time they are away from your lab.
To gain maximum benefits from this well-designed program, it is recommended that you send three or four of your front-line lab managers. Together, they will hear and learn at the same time, while working during the intimate sessions to identify the techniques and methods that will work best for your lab. This is important because, upon their return, they will have both enthusiasm and the knowledge to light the right fires under your lab staff and energize them into quickly deploying ways to slash expenses, attract top candidates to fill open positions, and even to tap new sources of revenue—all of which they learned during Lab Management Essentials.
Because the number of attendees to each workshop is limited, you are encouraged to click here to register yourself and your designated lab managers today.