Officials also worry about diminishing smallpox vaccinations, which offered people protection against the infectious disease
Monkeypox challenges from the current outbreak have dogged public health agencies even though the disease was first identified more than 50 years ago. That is because the virus has found new avenues of infection. These developments will be relevant for the nation’s clinical laboratories, which are often the first healthcare providers to confirm a suspected case is positive for monkeypox and notify a public health laboratory about the positive test result.
The latest monkeypox numbers from the federal Centers for Disease Control and Prevention (CDC) indicate that, as of September 6, the US has identified 19,962 cases in the 2022 outbreak, while worldwide the case number is 52,037.
In “When It Comes to Monkeypox Testing, Clinical Laboratories Should Be Aware of Five Significant Developments,” Dark Daily wrote about steps being taken to identify and control infections in America as well as trends in medical laboratory testing for monkeypox. This included reports of phlebotomists refusing to draw monkeypox blood samples and how social stigma surrounding the disease can affect who gets a medical laboratory test.
Workers at clinical laboratories and anatomic pathology groups will gain from understanding why monkeypox has spread beyond its traditional geography.
“Monkeypox symptoms include swollen lymph nodes, fever, and body aches that result in red bumps on hands, feet, mouth, and genitals,” Bodhraj Acharya, PhD (above), of the Laboratory Alliance of Central New York, told Dark Daily. “It spreads by close contact, respiratory droplets, lesions, and bodily fluids.” Clinical laboratories engaged in testing for monkeypox will want to stay alert to patients presenting with such symptoms. (Photo copyright: Laboratory Alliance of Central New York.)
African Public Health Officials Saw New Monkeypox Challenges Coming
Researchers and public health experts have been perplexed about how and why the latest monkeypox outbreak has occurred so aggressively beyond its origin in rural Central Africa.
“Monkeypox is caused by the pox virus, with a close resemblance to smallpox,” said Bodhraj Acharya, PhD, Manager of Chemistry and Referral Testing at the Laboratory Alliance of Central New York, in a conversation with Dark Daily. “Unlike COVID-19, this is an old enemy which has roots in the 1970s from Congo, when the disease was erratically endemic in Africa.”
According to the World Health Organization (WHO), most monkeypox cases since 1970 have been reported from rural rainforest regions in Central and Western Africa.
Thus, a monkeypox outbreak occurring in Europe and the United States in 2022 has puzzled virologists and microbiologists because it does not follow the historical pattern of the virus’ spread. For example, the first monkeypox case in the US arrived in May from a Massachusetts patient who had traveled to Canada, a state press release noted.
Before the Nigerian outbreak, the virus rose from rural areas where hunters came in close contact with animals. The illness resulted in lesions on the face, hands, and feet, Nature wrote of Yinka-Ogunleye’s recollections.
However, after 2017, she and other epidemiologists warned peers that the virus was spreading in new ways and in urban settings. For example, infected people sometimes had genital lesions, suggesting that the virus might spread through human sexual contact.
Now, in 2022, “the world is paying the price for not having responded adequately” in 2017, Yinka-Ogunleye told Nature.
Lack of Smallpox Vaccination Increases Monkeypox Challenges
The waning effects of smallpox vaccinations, which ended in 1980 after smallpox was basically eradicated from the world, may have opened the door for monkeypox to spread earlier this year. Smallpox vaccines provided some protection against monkeypox, but by now three generations of people have not received smallpox inoculations.
“Eyebrows were raised when multiple cases of monkeypox were reported from various non-endemic countries starting in May of 2022,” Acharya said. “Due to genetic similarity, smallpox vaccination provided some cross-protection, but the termination of smallpox vaccination could have provided ground for the recent insurgence and spread of monkeypox.”
Trying to jumpstart a new monkeypox vaccination campaign on the heels of COVID-19 shots may be met with resistance from a virus-weary public. But other options at preventing the current spread of monkeypox may present challenges as well, such as trying to curtail sexual activity among affected population, the BBC reported.
“The easiest way to prevent it is to close down all highly active sexual networks for a couple of months until it goes away, but I don’t think that will ever happen. Do you?” Paul Hunter, PhD, Professor of Medicine at the University of East Anglia in Norwich, England, told the BBC.
For medical laboratory workers and others who may find themselves testing for the disease in the future, the biggest lessons from current monkeypox challenges are twofold: The virus has invaded new geography, and discontinued smallpox vaccination campaigns may have left younger people exposed to monkeypox.
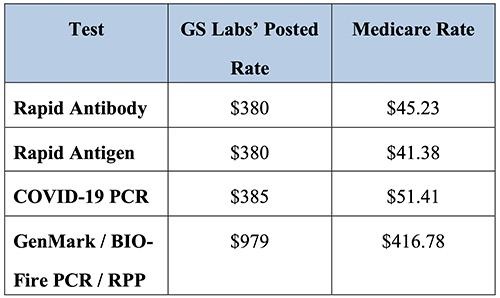
Insurers from three states claim pandemic start-up medical lab company charged as much as $979 for SARS-CoV-2 PCR test
In an unprecedented move, Blue Cross insurers in three states are suing a clinical laboratory company in Nebraska for test price gouging during the COVID-19 pandemic. The lawsuit claims that the lab company charged as much as 10 times more than other labs for similar tests.
The interesting twist to the pricing aspect of this story is that the Coronavirus Aid, Relief, and Economic Security Act (CARES Act) requires insurers to pay the full publicly-posted cost of COVID-19 testing. This means that, in many cases, the insurers may have no choice but to pay.
Is GS Labs, which was formed by an investment firm in the early months of the COVID-19 pandemic, yet another example of unscrupulous clinical laboratory operators taking advantage of the demand for COVID-19 testing during the early years of the coronavirus pandemic? GS Labs says no. The courts will decide.
Taken from the Premera Blue Cross court documents, the chart above shows GS Labs’ test prices compared with Medicare reimbursement rates. “As demonstrated by the following chart, the prices GS Labs charges insurers for COVID-19 testing well exceed the reimbursement rates set by Medicare Administrative Contractors, and in some cases are nearly ten times Medicare rates,” Premera states in the documents. Nevertheless, the federal CARES Act requires insurers to pay any COVID-19 test price a clinical laboratory posts publicly on its website. (Graphic copyright: Premera Blue Cross.)
Responding to Nationwide Demand for COVID-19 Testing
In October 2020, GS Labs began offering COVID-19 tests to provide Omaha residents with “convenient and quick testing options with same-day appointments and same-day results,” according to the company’s website. In response to nationwide demand, GS Labs quickly opened more than 20 testing COVID-19 testing sites across multiple states in its first three months of operations.
Today, GS Labs operates 14 rapid COVID testing locations in Iowa (1), Minnesota (6), Nebraska (1), Oregon (1) and Washington (5), but is under fire in several states for alleged price gouging.
Blue Cross Blue Shield of Kansas City was the first insurer to file suit in July 2021, alleging unreasonable reimbursement rates. The Kansas City Business Journal reported that GS Labs responded with a counter suit a month later accusing Blue KC of a “reckless disregard for the law” and attempting to bully its way out of paying for $9.7 million in COVID-19 testing fees.
The CARES Act states that, in the absence of a contractual payment agreement, insurers are required to pay the “cash prices” testing providers post on their public websites.
Christopher Erickson, a GS Labs Partner, told The New York Times (NYT), the law is on GS Labs’ side. “Insurers are obligated to pay cash price, unless we come to a negotiated rate,” he said.
In the fall of 2021, Premera Blue Cross also filed suit in Washington state alleging the lab routinely uses deceptive practices to run multiple unnecessary COVID tests on patients at an inflated cost. “In the words of one former employee, it ‘manipulates people into thinking they need all three COVID [sic] test’ that GS Labs offers, such that ‘[p]atients are being lied to just so th[e] company can make a profit,’” court documents state.
Premera also alleges in its lawsuit that GS Labs failed to report test results in a timely manner and returned hundreds of tests that were “by its own admission, tainted by “deviat[ions] from applicable laboratory standards for testing facilities.”
“This is fraud, and it’s fraud against Premera, it’s fraud against the industry, and more importantly, it’s fraud against the customers,” Courtney Wallace, DNP, Premera’s Director of Strategic Communications, told Washington State Wire.
And earlier this year, Blue Cross Blue Shield of Minnesota sued GS Labs to recover more than $10 million in over payments made since the start of the pandemic. A BCBS of Minnesota new release states that GS Labs “consistently charged more than five times the median market rate for its most commonly administered COVID-19 diagnostic test.”
CMS Inspection Finds GS Labs Site Posed “Immediate Jeopardy”
APM Reports spent nearly a year investigating the startup lab. Its team of journalists interviewed more than 65 GS Labs customers, former employees, and public health professionals, and reviewed thousands of pages of public documents. It concluded the lab “at times delivered inaccurate results, faced backlogs, charged high prices, and pushed customers into unnecessary tests.”
The APM Reports investigators found:
The company was slow to inform public health officials in several states about positive cases and in a few instances reported negative results to patients who had COVID-19. Other patients never received test results or received someone else’s results.
Overwhelmed by the number of tests it was processing, GS Labs at one point had a month-long backlog of untested samples.
Health officials in three states found GS Labs’ work was slower and less reliable than other labs.
According to APM Reports, in an email to colleagues about flaws in GS Labs’ operation in Washington state, Melissa Pond, [then] Program Manager for Clark County Washington’s COVID-19 Response Team, wrote, “[It] makes me so angry that they brought their greed to our community. They just popped up to make money knowing they would fly under the radar as long as possible and close their doors when someone caught them!”
Providing COVID-19 Testing During a Time of Need
APM Reports noted GS Labs’ founders formed the company in the early days of the pandemic after their friends and family could not find tests following a COVID exposure.
GS Labs is a subsidiary of City+Ventures, an Omaha investment and development company. Its portfolio includes an aviation investment company, car wash chain, car dealerships, restaurants, and other businesses.
City+Ventures’ co-founders, Erickson and Danny White had no healthcare investments prior to 2020, APM Reports noted. But early that year, the two men had joined with Gabe Sullivan and Darin Jackson, MD, who currently owns Prestige Medical Laser Solutions in Omaha, to create a men’s health and anti-aging company called 88MED. During the pandemic, that company transitioned to COVID-19 testing and was renamed GS Labs.
It is worth noting that GS Labs responded at length and in detail to the questions raised by the APM Reports investigation. It is useful reading for clinical laboratory leaders who wish to be fully informed on both sides of the controversy.
In its rebuttal, the company pointed out it had processed more than 2.1 million tests nationwide with less than 1.5% of its results being called into question. It maintained “GS Labs’ policy has never been to ‘push’ tests on anyone” and stated its cash prices “were higher than some testing providers,” but “lower than others” and reflected the company’s significant start-up costs.
GS Labs wrote, “At a time when our communities desperately needed increased COVID testing capacity, GS Labs took action to deliver that testing, investing more than $150 million in a business whose prospective success and lifespan were extremely uncertain. By filling a critical gap in COVID testing, GS Labs literally saved lives, and we are extremely proud of the service that we have provided to the communities we serve.”
GS Labs also has countersued BCBS of Minnesota, denying all prior allegations made by the insurer and alleging 21 counter claims.
Sabrina Corlette, JD, Research Professor and Project Director at Georgetown University Center on Health Insurance Reforms, has studied coronavirus testing prices. She told the NYT, “This is not like neurosurgery where you might want to pay a premium for someone to have years of experience.” She pointed out the CARES Act may provide GS Labs with the legal grounds to charge above market prices.
“Whatever price the lab puts on their public-facing website, that is what has to be paid,” she said.
GS Labs may have found a legal loophole to justify its sky-high COVID-19 testing prices, but consumers may view this behavior by a clinical laboratory company as unethical and yet another reason to be disillusioned with America’s healthcare system.
Viral reservoir could be behind persistence, says study, which also suggests a blood biomarker could be found for clinical laboratory testing
Microbiologists and virologists working closely with physicians treating long COVID-19 patients will gain new insights in a study that found coronavirus spike protein in COVID-19 patients’ blood up to 12 months after diagnosis. The researchers believe their findings could be used to develop a clinical laboratory biomarker for long COVID-19.
Researchers at Brigham and Women’s Hospital and Massachusetts General Hospital said medical experts are not sure why some people have unwelcome symptoms weeks and months after a positive COVID-19 diagnosis, while others clear the infection without lingering effects.
The scientists believe if this work is validated, clinical laboratories might gain an assay to use in the diagnosis of long COVID-19.
“The half-life of spike protein in the body is pretty short, so its presence indicates that there must be some kind of active viral reservoir,” said David Walt, PhD (above), Professor of Pathology, Brigham and Women’s Hospital, and lead author of the study that found coronavirus spike protein in long COVID patients. The study findings indicate a potential clinical laboratory biomarker for long COVID-19. (Photo copyright: Brigham and Women’s Hospital.)
Viral Reservoir Possibly Behind Long COVID-19
The study suggests that SARS-CoV-2 finds a home in the body, particularly the gastrointestinal tract, “through viral reservoirs, where it continues to release spike protein and trigger inflammation,” Medical News Today reported.
Lead author of the study David Walt, PhD, Professor of Pathology, Brigham and Women’s Hospital and the Hansjörg Wyss Professor Biologically Inspired Engineering at Harvard Medical School, told The Guardian he “was motivated to carry out the study after earlier research by his colleagues detected genetic material from the COVID virus (viral RNA) in stool samples from children with multisystem inflammatory syndrome (a rare but serious condition that often strikes around four weeks after catching COVID) as well as spike protein and a marker of gut leakiness in their blood.”
Long COVID—also known as long-haul COVID, post-COVID-19, or its technical name, post-acute sequelae of COVID-19 or PASC—can involve health problems continuing weeks, months, or even years after a positive diagnosis, according to the federal Centers for Disease Control and Prevention (CDC).
Symptoms of long COVID, according to the researchers, include:
fatigue,
loss of smell,
memory loss,
gastrointestinal distress, and
shortness of breath.
“If someone could somehow get to that viral load and eliminate it, it might lead to resolution of symptoms,” Walt told the Boston Globe, which noted that the researchers may explore a clinical trial involving antiviral drugs for treatment of long COVID-19.
Clues from Earlier Studies on Long COVID-19
Medical conditions that persisted following a COVID-19 infection have been studied for some time. In fact, in an earlier study, Walt and others found children who developed a multisystem inflammation syndrome weeks after being infected by SARS-CoV-2, according to their 2021 paper published in The Journal of Clinical Investigation, titled, “Multisystem Inflammatory Syndrome in Children Is Driven by Zonulin-Dependent Loss of Gut Mucosal Barrier.”
Although these earlier studies provided clues, the cause of PASC remains unclear, the researchers noted. They planned to take a more precise look at PASC biology by using appropriate sampling and patient recruitment.
“Disentangling the complex biology of PASC will rely on the identification of biomarkers that enable classification of patient phenotypes. Here, we analyze plasma samples collected from PASC and COVID-19 patients to determine the levels of SARS-CoV-2 antigens and cytokines and identify a blood biomarker that appears in the majority of PASC patients,” the researchers wrote.
Finding a Marker of a Persistent Infection
The researchers used plasma samples from 63 people with a previous SARS-CoV-2 diagnosis (37 also had PASC), Medical News Today reported. Over a 12-month period, the researchers’ findings included:
Detection in 65% of PASC samples of full-length spike, S1 spike, and nucleocapsid throughout the year of testing.
Spike detected in 60% of PASC patient samples, and not found in the COVID-19 samples.
In an interview with Scientific American, bioengineer Zoe Swank PhD, post-doctoral researcher, Brigham and Women’s Hospital, and co-author of the study, said, “Our main hypothesis is that the spike protein is not causing the symptoms, but it’s just a marker that is released because you still have infection of some cells with SARS-CoV-2.”
In that article, Swank shared the scientists’ intent to do more research involving hundreds of samples over the course of the COVID-19 pandemic from many hospitals and people.
COVID-19 Not the Only Virus That Hangs On
Having a long-haul COVID-19 marker is a “game-changer,” according to an infectious disease expert who was not involved in the study.
“There has not so far been a clear, objective marker that is measurable in the blood of people experiencing long COVID-19,” Michael Peluso, MD, Assistant Professor, Medicine, University of California San Francisco, told Scientific American. “I hope their findings will hold up. It really would make a difference for a lot of people if a marker like this could be validated,” he added.
However, COVID-19 is not the only virus that could persist. Ebola also may linger in areas that skirt the immune system, such as the eye interior and central nervous system, according to a World Health Organization fact sheet.
Thus, medical laboratory leaders may want to follow the Brigham and Women’s Hospital research to see if the scientists validate their finding, discover a biomarker for long-haul COVID-19, and pursue a clinical trial for antiviral drugs. Such discoveries could have implications for how diagnostic professionals work with physicians to care for long COVID patients.
There are reports of phlebotomists refusing to draw monkeypox blood samples and social stigma surrounding the disease can affect who gets a medical laboratory test
Cases of monkeypox are increasing in the US—14,115 as of Aug. 19, up 1,400 from the prior week—and clinical laboratories around the country are bracing for a potential increase in monkeypox testing orders.
Several factors, however, are affecting the testing. Chief among them:
Lab workers refusing to take blood draws from potential monkeypox patients, and
Community clinics in some cities having to delay other care to deal with an onslaught of monkeypox test orders.
Here are five trends clinical laboratory leaders should be aware of that are influencing the state of monkeypox testing in the country.
Trend 1: Some Phlebotomists Refuse to Draw Possible Monkeypox Specimens
CNN reported that phlebotomists at two of the largest commercial laboratories—Labcorp and Quest Diagnostics—were either refusing or being told not to draw blood samples from suspected monkeypox patients.
“Labcorp and Quest don’t dispute that, in many cases, their phlebotomists are not taking blood from possible monkeypox patients,” according to CNN. “What remains unclear, after company statements and follow-ups from CNN, is whether the phlebotomists are refusing on their own to take blood or if it is the company policy that prevents them. The two testing giants say they’re reviewing their safety policies and procedures for their employees.”
In “Medical Laboratories Respond to Monkeypox Outbreak Using CDC-Developed Diagnostic Test,” Dark Daily noted that skin lesion swabbing, such as that necessary to perform the OrthopoxvirusPCR test, is the preferred method to check for monkeypox because of higher viral counts in the lesions. However, physicians may order follow-up blood tests for confirmed monkeypox patients, and suspected patients may need bloodwork as part of other routine care.
In an update posted on its website, Quest noted it has been testing swab specimens of skin lesions for monkeypox, but those swabs are performed by providers and not Quest. However, the company was also preparing to take blood draws of possible monkeypox patients in its patient service centers.
“Given that monkeypox has been declared a national public health emergency and the most recent CDC guidance, we are now implementing procedures to safely enable patients with suspected or confirmed monkeypox infection into our patient service sites for phlebotomy blood draws and other non-swab specimen collections,” Quest stated. “This approach will enable patients with suspected or confirmed monkeypox infections to receive additional testing they may need.”
Trend 2: Guidance Is Available to Help Lab Workers Avoid Monkeypox Infection
The CDC has posted guidance to maintain infection control around suspected monkeypox specimens. Among the steps noted by the agency:
Lesion specimens from patients suspected of having monkeypox will carry the highest quantity of the virus. When possible, lab workers that have a smallpox vaccination from within the last three years should handle these specimens. Smallpox vaccination also protects from monkeypox in many cases. Unvaccinated workers who test suspected monkeypox specimens need to take extra precautions, such as wearing a buttoned lab coat, gloves, and face protection, and avoiding splashes, the CDC stated.
Blood specimens draw from suspected monkeypox patients will have a low quantity of the virus. Lab workers testing these specimens do not need to be vaccinated for monkeypox, but standard precautions should be followed.
Before using automated testing platforms with suspected monkeypox specimens, labs should conduct a risk assessment to identify potential hazards.
Trend 3: Monkeypox Testing Gains an Early Social Stigma
Some people who need to be tested for monkeypox may be hesitant to seek out a medical laboratory or patient service center because of a stigma being attached to the disease.
Although it does not match the early hysteria associated with HIV infections in the 1980s—in a 1987 poll, 60% of respondents said AIDS patients should carry a card identifying them as such, Gallup noted—there have been clear instances where people and agencies have associated monkeypox infection with men having sex with other men.
“The focus for all countries must be engaging and empowering communities of men who have sex with men to reduce the risk of infection and onward transmission, to provide care for those infected, and to safeguard human rights and dignity,” Tedros Adhanom Ghebreyesus, PhD, the Director-General at the World Health Organization, said in a July 27 media briefing.
Ghebreyesus added that while 98% of monkeypox infections have been among men who have sex with men, anyone can get the disease, including children.
“Stigma and discrimination can be as dangerous as any virus, and can fuel the outbreak,” said Tedros Adhanom Ghebreyesus, PhD (above), Director-General at the World Health Organization (WHO), in a media briefing. Clinical laboratories would be wise to prepare for a marked increase in demand for monkeypox testing. (Photo Copyright: WHO/Christopher Black.)
“Men who have sex with men have been hit the hardest by monkeypox to date, but LGBTQ+ health advocates say improper messaging risks branding monkeypox as a ‘gay disease,’ eroding effective preventive measures and allowing the virus to spread,” Bloomberg Law reported.
For example, 66% of respondents either were not sure or did not believe there is a vaccine for monkeypox.
Trend 4: Workers Who Refuse to Test Patients for Monkeypox Face Possible Backlash
Some medical professionals have raised concerns about healthcare workers being unwilling to test monkeypox patients.
“This is absolutely inexcusable. It’s a grave dereliction of duty,” David Harvey, Executive Director of the National Coalition of STD Directors, told CNN. The group represents sexually transmitted disease (STD) directors at public health departments in the US.
“For every single patient that walks [through] your door, you use universal precautions because every disease doesn’t have a phenotype or outward appearance, so you have to treat everyone exactly the same,” Garfield Clunie, MD, president of the National Medical Association and Assistant Professor of Obstetrics, Gynecology, and Reproductive Science at the Icahn School of Medicine at Mount Sinai, told Bloomberg Law. “You can’t treat someone differently because of their sexual orientation, or race, or gender, or for any other reason.”
Trend 5: Public Clinics Show Early Signs of Monkeypox Testing Pressure
A survey of 80 public health departments conducted by the National Coalition of STD Directors indicated that some sites may already be getting overwhelmed by demand for monkeypox testing.
According to the survey results, 79% of public health clinics saw an increased demand for monkeypox testing over the past four weeks. In a troubling aspect, 28% of clinics said they could not meet testing demand if it increases.
Further, 22% of clinics have reduced screenings for other STDs to prioritize monkeypox testing. Such moves likely delay patients from receiving other care they need.
Clinical laboratories may want to take note of the survey findings. The pressure public health clinics currently face could be a precursor to similar problems at labs if demand for monkeypox testing grows.
Experts say it is time ‘to restore our confidence in vaccines’ as many medical laboratories take steps to support testing for the polio virus
Clinical laboratories and microbiologists in the state of New York will want to know that, in July, a man in New York was diagnosed with polio and subsequently the virus was detected in the wastewater of two New York counties.
The area, Rockland County, N.Y., just north of New York City, was also at the forefront of a measles outbreak that occurred in 2018 and 2019. The outbreak was attributed to low vaccination rates within the community.
The unidentified, immunocompetent young man was admitted to a New York hospital after experiencing a low-grade fever, neck stiffness, back and abdominal pain, constipation, and lower extremity weakness. He eventually developed paralysis from the disease, which is irreversible.
Poliomyelitis, commonly known as polio, is a disabling and life-threatening disease that is caused by the poliovirus. Though it rarely surfaces in the United States, there is now confirmation of the first US case since 2013.
“The polio vaccine is safe and effective, protecting against this potentially debilitating disease, and it has been part of the backbone of required, routine childhood immunizations recommended by health officials and public health agencies nationwide,” said Mary T. Bassett, MD (left), Health Commissioner at the New York Department of Health, in a press release. Clinical laboratories and microbiologists in New York may want to prepare for an increase in vaccination requests. (Photo copyright: Time.)
Is Polio Back in America? Clinical Laboratories Will Want to Be Prepared
“I think it’s concerning because it can spread,” epidemiologist Walter Orenstein, MD, Professor, Department of Medicine, Division of Infectious Diseases at Emory University School of Medicine told STAT. “If there are unvaccinated communities, it can cause a polio outbreak.”
According to the federal Centers for Disease Control and Prevention (CDC), public health experts are working diligently to discover how and where the infected individual contracted polio. The CDC website states that the risk for people who have received the polio vaccine is very low, but there is concern for those who have not received the recommended doses of the vaccine.
“Most of the US population has protection against polio because they were vaccinated during childhood, but in some communities with low vaccine coverage, there are unvaccinated people at risk,” the CDC noted. “Polio and its neurologic effects cannot be cured but can be prevented through vaccination.”
The US uses an injectable polio vaccine for the poliovirus which contains killed viruses. The vaccine “instructs” the immune system to recognize and combat the virus. This inactivated polio vaccine (IPV) is administered to children as a shot in the arm or leg and is typically given in four separate doses.
“The inactivated polio vaccine we have is very effective and very safe and could have prevented this,” Orenstein told STAT. “We need to restore our confidence in vaccines.”
“Based on what we know about this case, and polio in general, the (New York) Department of Health strongly recommends that unvaccinated individuals get vaccinated or boosted with the FDA-approved IPV polio vaccine as soon as possible,” said Mary T. Bassett, MD, Health Commissioner at the New York Department of Health in a press release.
Poliovirus Found in Wastewater via Use of Gene Sequencing
Poliovirus is very contagious and is transmitted through person-to-person contact. The virus lives in an infected person’s throat and intestines and can contaminate food and water in unsanitary conditions. According to the CDC, typical symptoms of the illness include flu-like symptoms such as:
Sore throat
Fever
Tiredness
Nausea
Headache
Stomach pain
Most of these symptoms will disappear within five days, but polio can invade the nervous system and cause more serious complications, such as meningitis, paralysis, and even death.
After confirmation of the new case of polio, wastewater surveillance detected the presence of the poliovirus in Rockland and Orange counties, New York.
Wastewater analysis can uncover pathogens within a community and has been used in the fight against other infectious diseases, including:
“In some regards, wastewater is a public health dream scenario,” said Mark Siedner, MD, an infectious disease doctor at Massachusetts General Hospital and associate professor at Harvard Medical School, in an interview with Fortune. “Everyone poops, and most people poop every day. It provides real-time data on infection rates. In that regard, it’s an extremely powerful tool, particularly good at detecting early warning signs. Before people get sick, we might get a signal.”
Wastewater analysis can provide insights regarding the types of viruses that people within a community are shedding and if the volume of those viruses are increasing. This information can provide scientists with an early marker for an outbreak of an illness that is on the verge of spreading.
Microbiologists and clinical laboratories should be aware of the specific types of infectious agents public health authorities are detecting in wastewater, even as they perform screening and diagnostic tests on their patients for similar infectious diseases.
Polio is Appearing Worldwide
The Global Polio Eradication Initiative (GPEI) has announced that new cases of polio have been reported in Israel and the United Kingdom. These are countries where polio cases are extremely rare.
This indicates that microbiologists and clinical laboratories managers will want to be on constant alert for uncommon infectious diseases that may appear suddenly, even if those illnesses are rare. Accurate and immediate diagnoses of such infectious diseases could play a major role in triggering a public health response to control potential outbreaks while they are in their earlier stages.
Clinical laboratories continue to report positive COVID-19 tests for individuals that have been vaccinated and even previously infected with the same variant of the coronavirus
Researchers across the globe continue to study the SARS-CoV-2 coronavirus and its many variants. Their goals are to curb the spread of the disease and develop new therapies and treatments for optimal patient outcomes. Now, a study conducted by scientists at the University of Missouri (UM) provides deeper insight into the processes the virus uses to mutate and overpower the human immune system. These findings could lead to improved antivirals and clinical laboratory tests for COVID-19.
The UM team identified specific mutations occurring within the virus’ spike protein that help Omicron subvariants evade existing antibodies and create an infection. These mutations may explain why some people who have had previous COVID-19 infections and/or who are fully vaccinated continue to test positive for SARS-CoV-2, and why the virus continues to evolve.
“Omicron now has more than 130 sublineages and they have been here for quite a while. We are now just finally able to detect them and differentiate among them with this research,” said Kamlendra Singh, PhD, associate research professor in the Department of Veterinary Pathobiology at UM’s College of Veterinary Medicine, in a UM press release.
“Previous variants, including Alpha, Beta, Gamma, and Delta, contributed to many of the mutations occurring now with these Omicron variants. So, our research shows how the virus has evolved over time with new mutations,” he added.
“Throughout the pandemic, the [SARS-CoV-2] virus has continued to get smarter and smarter. Even with vaccines, it continues to find new ways to mutate and evade existing antibodies,” said Kamlendra Singh, PhD (above), Associate Research Professor, College of Veterinary Medicine at University of Missouri, in a UM press release. This research team’s findings may help clinical laboratories further develop their SARS-CoV-2 antibody tests. (Photo copyright: University of Missouri.)
Antibodies for One Variant, but Not for Another
The scientists began their investigation by researching online databases that track COVID-19 cases and analyzing the protein sequences from more than 10 million Omicron-related samples that were collected from around the world since November of last year.
They examined the available sequences, structures of spike/receptor and spike/antibody complexes of the samples, and then conducted molecular dynamics simulations. The team utilized 3D modeling to locate where mutations occur and created structures of the spike protein to determine how the mutations are affected by antibodies and vaccinations.
The researchers found that the Omicron variant continues to mutate and has become extremely efficient at adaptation. Reinfections are happening because many individuals do not possess the antibodies for the new subvariants that continue to develop.
“Vaccinated individuals, or those who have previously tested positive, may have the antibodies for one variant but not necessarily for any of the other variants,” Singh explained. “The various mutations may seem like only subtle differences, but they are very important.”
The UM scientists’ research shows it is possible to differentiate Omicron subvariants from each other and pinpoint how certain mutations might become problematic for patients. According to Singh, many people can be infected with multiple variants at the same time. He is hopeful that their work will make it possible for vaccines and other treatments to specifically target different strains of the virus.
Singh also believes that the coronavirus is most likely never going to disappear from society and that new variants and their sublineages will continue to appear and evolve.
“The ultimate solution going forward will likely be the development of small molecule, antiviral drugs that target parts of the virus that do not mutate,” Singh said. “While there is no vaccine for HIV, there are very effective antiviral drugs that help those infected live a healthy life, so hopefully the same can be true with COVID-19.”
Omicron Subvariants May Be Here to Stay
“I am proud of my team’s efforts, as we have identified specific mutations for various variants throughout the pandemic, and it feels good to be contributing to research that is assisting with the situation,” Singh said. “We will continue to help out, as there will surely be new variants in the future.”
Singh is also part of a team that developed a supplement called CoroQuil-Zn, which was designed to reduce a patient’s viral load after being infected with SARS-CoV-2. The drug is currently being used in parts of India and is awaiting approval from the US Food and Drug Administration (FDA).
Clinical laboratories that perform antibody testing for SARS-CoV-2 infections should be aware that the coronavirus will likely be moving among humans for many years to come. This recent research may aid in the development of new antivirals, treatments, and vaccines that target specific subvariants for the best patient outcomes.