This is the first of a three-part series on revenue cycle management for molecular testing laboratories and pathology practices, produced in collaboration with XiFin, Inc.
Setting Your Organization Up for Success: Maximizing Revenue for Molecular Diagnostics and Pathology Testing Starts Well Before Billing
What progressive revenue cycle management technology reveals about revenue levers, test clearances, and strategic planning for molecular and pathology testing.
CFOs and other leaders of molecular testing laboratories and pathology groups need to raise their awareness of the most vulnerable aspects of revenue. To this end, this article outlines three specific areas of potential revenue cycle management (RCM) improvement so molecular diagnostic and pathology organizations can better identify and adapt to localized market dynamics and individual patient needs.
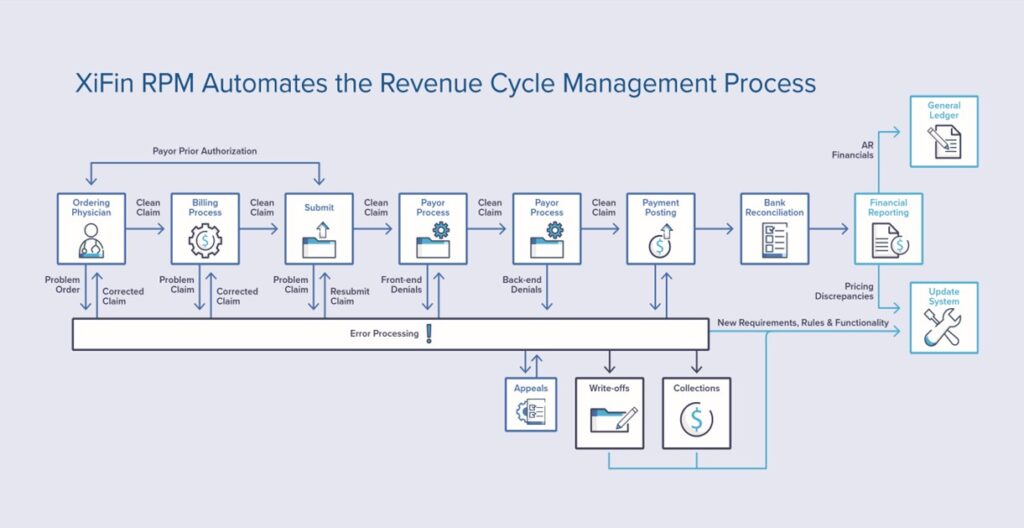
“Many people look at RCM as just billing or getting a clean billing process, but laboratory testing is getting more complex; consequently, reimbursement is getting more complicated, and continually changing payer policies are also making it more challenging for labs to keep up. It is important for business executives, revenue cycle leaders, and CFOs to look more broadly at the revenue cycle,” explained Clarisa Blattner, XiFin Senior Director of Revenue and Payor Optimization. XiFin recommends lab and pathology leaders consider revenue cycle within the broader context of the patient journey, which generally includes, among other things, three key revenue-impacting patient engagement stages.
The first of the three stages, patient access and financial clearance, begins when patient demographics and insurance information are captured. Following demographics and insurance details is a determination of benefits coverage and verification of eligibility. Financial information on any required copay and deductibles are determined, and pre-payment is collected. Finally, the patient receives a financial responsibility estimate for any out-of-pocket expenses.
In stage 2, clinical/medical clearance requires ordering physician engagement to address medical necessity questions and obtain supporting documentation. Clinical assessment and diagnostic testing are conducted. The encounter document is completed. Results are shared via secure, seamless, connected communication between the ordering physician’s office, the lab of the diagnostic provider, and the patient. Finally, the claim is submitted for reimbursement with all relevant supporting documentation.
The third stage is when payer management activities are essential to maximizing reimbursement by ensuring claim submissions include prior authorizations, clinical documentation, proprietary payer forms and comply with payer policies and requirements. Through this stage, patient engagement ensures all the correct data is in place, and insurance information or coverage hasn’t changed or is appropriately updated. Anticipating payer responses and subsequent actions is critical to collecting the full amount payers are responsible for to minimize patient financial impact. Once all payer activities are exhausted, the patient must be sent their statement for the remaining balance in their preferred communication method (paper, text, email, portal, etc.). Additionally, payment collection is accelerated when a diagnostic provider makes it easy and convenient to make payments, manage payment plans, and change payment methods.
These three stages in the patient journey encompass important revenue levers that cannot be overlooked. They are foundational to automating the financial performance engine needed for molecular diagnostics and pathology practices, Blattner continued. Whereas specialty diagnostics are rapidly coming to market and localized with varying reach, availability, and insurance coverage assurance, activating specific “clearance” functions or “engagement” opportunities within these levers will be key to smooth claims processing, timely filing, and optimizing all payment avenues.
Blattner stresses that when not built into automatic administrative functions, these three types of stages (i.e., patient access, physician engagement, and payer management) will slow or indefinitely stall payment for molecular diagnostics and pathology providers.
Market Expansion and Shift in at-Home Testing Stresses Traditional Administrative Approaches
Novel diagnostics are being introduced in record numbers as physicians and diagnostic business leaders seek to address and fulfill unmet diagnostic and medical needs to support better health outcomes. Along with these new medical breakthroughs comes the demand for traditional administrative approaches to reinvent themselves – including RCM. This major operational shift and frequent payer policy changes with advanced diagnostics have strained traditional administrative practices. According to Blattner, when executives realize that manual processes and inadequate electronic billing functions have reached a breaking point, specialized automation is the natural next step. The items corresponding to the highest value revenue cycle activities may sound surprising within the three revenue levers—patient access, medical clearance, and payer management.
Patient Access, Engagement, and Financial Clearance
“Making it easy for physicians to order molecular diagnostics and pathology tests is so important for success in today’s market,” Blattner continued. Ordering physicians and lab teams must have accurate and timely information regarding a patient’s ‘financial clearance’ (the likelihood a test will be covered, what the patient is likely to be charged out-of-pocket, and whether prior authorization is required). Patient portals and multi-channel communications are important parts of effective RCM functionality that facilitate patient access and financial clearance.
“It used to be that a patient went to the lab, and a phlebotomist saw the patient, but now more tests involve specimen collection at home. A kit is distributed at the physician’s office or ordered online and shipped to the patient,” Blattner said. “There is more follow-through needed to make sure not only did the test get done, but did it get returned, because while there are upfront costs to serve the patient, the lab doesn’t get paid until the test is completed, returned, processed and the diagnosis is determined for the claim to be processed. That is an evolution as these tests leave the laboratory or the business and enter the home environment.”
Patient access and engagement tools provide various benefits, including offering a cost-effective alternative to traditional customer service calls and supporting patients’ communication preferences. Effective physician access and engagement programs and technology help diagnostic providers offer self-service tools that enable patients to securely log in, anytime, to:
View statements
Make credit card payments
Set up payment plans (using lab-specified rules and parameters)
Establish paperless billing
View patient responsibility estimates
View test results
Another critical aspect of patient financial clearance for diagnostic testing is the ability to provide patients with an accurate estimation of their out-of-pocket costs associated with a test. Practical patient communication tools enable ordering physicians’ staff members to assist patients in preparing for out-of-pocket expenses, which increases test completion rates and has been proven to reduce write-offs.
To accurately assess a patient’s financial responsibility, the estimation tool must consider relevant provider and plan specific pricing and test or procedure information, as well as provide access to real-time eligibility data. A proper estimation of a patient’s out-of-pocket expenses is also predicated on receiving complete and accurate information from the payer. Examining payer behavior can uncover responses that create inaccurate patient responsibility estimates.
Physician engagement programs help diagnostic providers integrate communication and data exchange more deeply with ordering physicians and complete clinical clearance. Clinical clearance involves things like medical necessity, familial history, and social determinants of health. Robust RCM also requires diagnostic providers, laboratories, and pathology practices to be able to seamlessly communicate with patients to ensure that samples, devices, or readings are collected and returned to the diagnostic provider so that services/tests can be completed.
Effective physician engagement and clinical clearance increase ordering volume, maximize clean claims and automate denials and appeals management. Physician engagement technology, including electronic communication tools such as portals, helps physicians and their teams streamline the online correction of missing information and errors. This improves satisfaction, expedites reimbursement, and provides cost savings. With effective physician engagement programs and technology tools, physicians and their staff can more effectively:
Perform order entry
Access clinical decision support
Examine statements at the line-item level
View test information and pricing
Correct billing errors upfront to expedite reimbursement
Provide patients with an estimate of their out-of-pocket cost
Payer Management
Molecular diagnostic and genetic tests are famously complex and present many unique operational and financial challenges for laboratories. Payer policies and behavior are constantly changing, and labs (and their billing partners) must stay abreast of changes to avoid lengthy delays that denials and subsequent appeals can cause. Intelligent automation of prior authorizations, insurance discovery, and benefits determination are especially important for these tests.
Unfortunately, it is common for diagnostic providers to only learn about a change in reimbursement after the month-end close. These changes manifest in billing as:
New denials
Changes in denial rate
Changes in reimbursement rate
Change in time to payment
Failure to quickly recognize and adapt workflows to payer reimbursement changes can result in costly appeals and write-offs. XiFin recommends that providers adopt a proactive strategy to identify changes in reimbursement earlier. It is essential to understand the impacts and risks of price discrepancies and changes in pricing to patients. Staying abreast of policy changes for Medicare and commercial payers enables molecular diagnostic laboratories and pathology groups to proactively employ front-end billing system edits to avoid denials.
Keys to Success
For molecular diagnostic providers and pathology groups to maximize reimbursement, CFOs, and revenue cycle leaders must take a broader view of RCM. The RCM process starts well before billing and runs parallel to the patient journey in many respects. This means that effective RCM technology and tools also stretch beyond the billing system to incorporate seamless communication between systems and parties throughout the patient journey.
Adaptive RCM approaches require automation, intelligence, and real-time communication for the three key revenue-impacting stages discussed in this article: patient access, medical clearance, and payer management. This involves seamless integration with various tools that enable insurance discovery, patent demographic and eligibility verifications, patient financial responsibility estimation, and reporting and analytics that allow early identification of and response to changes in payer behavior.
Molecular diagnostic labs and pathology practices must have tools and technology to align with payers on evidence requirements, including clinical utility evidence, current billing policies, and preferred coding approaches. They must have seamless connectivity to ordering physicians to order tests and ensure the completeness of medical necessity and medical record documentation.
Finally, XiFin recommends that diagnostic organizations use analytics to enable early insight into changes in payer behavior, address root causes, and be able to adjust to changes in ordering patterns and client data quality. Be sure to consider an RCM platform that has embedded artificial intelligence (AI) to drive efficient automation of workflow adaptation to payer changes and future-proof your RCM investment.
Financial executives seeking to maximize market access and capitalize on growth opportunities in key markets will want to explore how successfully their administrative teams are navigating the unique revenue cycle landscape specific to molecular testing and pathology.
Part 2 of this three-part series is coming soon. Watch for updates here at DarkDaily.
If validated, study findings may result in new biomarkers for clinical laboratory cholesterol tests and for diagnosing dementia
Researchers continue to find new associations between biomarkers commonly tested by clinical laboratories and certain health conditions and diseases. One recent example comes from research conducted by the University of California San Francisco. The UCSF study connected cholesterol biomarkers generally used for managing cardiovascular disease with an increased risk for dementia as well.
The researchers found that both high and low levels of high-density lipoprotein (HDL)—often referred to as “good” cholesterol—was associated with dementia in older adults, according to a news release from the American Academy of Neurology (AAN).
UCSF’s large, longitudinal study incorporated data from 184,367 people in the Kaiser Permanente Northern California health plan. How the findings may alter cholesterol biomarker use in future diagnostics has not been determined.
“The elevation in dementia risk with both high and low levels of HDL cholesterol was unexpected, but these increases are small, and their clinical significance is uncertain,” said epidemiologist Maria Glymour, ScD (above), study author and Professor of Epidemiology and Biostatistics at UCSF School of Medicine, in a news release. This is another example of how researchers are associating common biomarkers tested regularly by clinical laboratories with additional health conditions and disease states. (Photo copyright: University of California San Francisco.)
HDL Levels Link to Dementia Risk
The UCSF researchers used cholesterol measurements and health behavior questions as they tracked Kaiser Permanente Northern California health plan members who were at least 55 years old between 2002 and 2007, and who did not have dementia at the time of the study’s launch.
The researchers then followed up with the study participants through December 2020 to find out if they had developed dementia, Medical News Today reported.
“Previous studies on this topic have been inconclusive, and this study is especially informative because of the large number of participants and long follow-up,” said epidemiologist Maria Glymour, ScD, study author and Professor of Epidemiology and Biostatistics at UCSF School of Medicine, in the AAN news release. “This information allowed us to study the links with dementia across the range of cholesterol levels and achieve precise estimates even for people with cholesterol levels that are quite high or quite low.”
According to HealthDay, UCSF’s study findings included the following:
More than 25,000 people developed dementia over about nine years. They were divided into five groups.
53.7 milligrams per deciliter (mg/dL) was the average HDL cholesterol level, amid an optimal range of above 40 mg/dL for men and above 50 mg/dL for women.
A 15% rate of dementia was found in participants with HDL of 65 mg/dL or above.
A 7% rate of dementia was found in participants with HDL of 11 mg/dL to 41 mg/dL.
“We found a U-shaped relationship between HDL and dementia risk, such that people with either lower or higher HDL had a slightly elevated risk of dementia,” Erin Ferguson, PhD student of Epidemiology at UCSF, the study’s lead study author, told Medical News Today.
What about LDL?
The UCSF researchers found no correlation between low-density lipoprotein (LDL)—often referred to as “bad” cholesterol”—and increased risk for dementia. But the risk did increase slightly when use of statin lipid-lowering medications were included in the analysis.
“Higher LDL was not associated with dementia risk overall, but statin use qualitatively modified the association. Higher LDL was associated with a slightly greater risk of Alzheimer’s disease-related dementia for statin users,” the researchers wrote in Neurology.
“We found no association between LDL cholesterol and dementia risk in the overall study cohort. Our results add to evidence that HDL cholesterol has similarly complex associations with dementia as with heart disease and cancer,” Glymour noted in the AAN news release.
Australian Study also Links High HDL to Dementia
A separate study from Monash University in Melbourne, Victoria, Australia, found that “abnormally high levels” of HDL was also associated with increased risk for dementia, according to a Monash news release.
The Monash study—which was part of the ASPREE (ASPpirin in Reducing Events in the Elderly) trial of people taking daily aspirin—involved 16,703 Australians and 2,411 Americans during the years 2010 to 2014. The researchers found:
850 participants had developed dementia over about six years.
A 27% increased risk of dementia among people with HDL above 80 mg/dL and a 42% higher dementia risk for people 75 years and older with high HDL levels.
These findings, Newsweek pointed out, do not necessarily mean that high levels of HDL cause dementia.
“There might be additional factors that affect both these findings, such as a genetic link that we are currently unaware of,” Andrew Doig, PhD, Professor, Division of Neuroscience at University of Manchester, told Newsweek. Doig was not involved in the in the Monash University research.
Follow-up research could explore the possibility of diagnosing dementia earlier using blood tests and new biomarkers, Newsweek noted.
Cholesterol Lab Test Results of Value to Clinical Labs
If further studies validate new biomarkers for testing and diagnosis, a medical laboratory’s longitudinal record of cholesterol test results over many years may be useful in identifying people with an increased risk for dementia.
Clinical pathologists and laboratory managers will want to stay tuned as additional study insights and findings are validated and published. Existing laboratory testing reference ranges may need to be revised as well.
As well, the findings of this UCSF research demonstrate that, in this age of information, there will be plenty of opportunities for clinical lab scientists and pathologists to take their labs’ patient data and combine it with other sets of data. Digital tools like artificial intelligence (AI) and machine learning would then be used to assess that large pool of data and produce clinically actionable insights. In turn, that positions labs to add more value and be paid for that value.
One goal of these new functions is to streamline physician workflows. However, these new EHRs may interface differently with clinical laboratory information systems
Artificial intelligence (AI) developers are making great contributions in clinical laboratory, pathology, radiology, and other areas of healthcare. Now, Electronic Health Record (EHR) developers are looking into ways to incorporate a new type of AI—called “Generative AI”—into their EHR products to assist physicians with time-consuming and repetitive administrative tasks and help them focus on patient-centered care.
Generative AI uses complex algorithms and statistical models to learn patterns from collected data. It then generates new content, including text, images, and audio/video information.
According to the federal Government Accountability Office (GAO), generative AI “has potential applications across a wide range of fields, including education, government, medicine, and law” and that “a research hospital is piloting a generative AI program to create responses to patient questions and reduce the administrative workload of healthcare providers.”
Reducing the workload on doctors and other medical personnel is a key goal of the EHR developers.
Generative AI uses deep learning neural networks modeled after the human brain comprised of layers of connected nodes that process data. It employs two neural networks: a generator [generative network] which creates new content, and a discriminator [discriminative network] which evaluates the quality of that content.
The collected information is entered into the network where each individual node processes the data and passes it on to the next layer. The last layer in the process produces the final output.
Many EHR companies are working toward adding generative AI into their platforms, including:
As our sister publication The Dark Report points out in its December 26 “Top 10 Biggest Lab Stories for 2023,” almost every product or service presented to a clinical laboratory or pathology group will soon include an AI-powered solution.
“We believe that generative AI has the potential of being a personal assistant for every doctor, and that’s what we’re working on,” Girish Navani (above), co-founder and CEO of eClinicalWorks, told EHRIntelligence. “It could save hours. You capture the essence of the entire conversation without touching a keyboard. It is transformational in how it works and how well it presents the information back to the provider.” Clinical laboratory information systems may also benefit from connecting with generative AI-based EHRs. (Photo copyright: eClinicalWorks.)
Generative AI Can Help with Physician Burnout
One of the beneficial features of generative AI is that it has the ability to “listen” to a doctor’s conversation with a patient while recording it and then produce clinical notes. The physician can then review, edit, and approve those notes to enter into the patient’s EHR record, thus streamlining administrative workflows.
“The clinician or support team essentially has to take all of the data points that they’ve got in their head and turn that into a narrative human response,” Phil Lindemann, Vice President of Data and Analytics at Epic, told EHRIntelligence. “Generative AI can draft a response that the clinician can then review, make changes as necessary, and then send to the patient.”
By streamlining and reducing workloads, EHRs that incorporate generative AI may help reduce physician burnout, which has been increasing since the COVID-19 pandemic.
“Language models have a huge potential in impacting almost every workflow,” Girish Navani, co-founder and CEO of eClinicalWorks, told EHRIntelligence. “Whether it’s reading information and summarizing it or creating the right type of contextual response, language models can help reduce cognitive load.”
Generative AI can also translate information into many different languages.
“Health systems spend a lot of time trying to make patient education and different things available in certain languages, but they’ll never have every language possible,” Lindemann said. “This technology can take human language, translate it at any reading level in any language, and have it understandable.”
MEDITECH is working on a generative AI project to simplify clinical documentation with an emphasis on hospital discharge summaries that can be very laborious and time-consuming for clinicians.
“Providers are asked to go in and review previous notes and results and try to bring that all together,” Helen Waters, Executive Vice President and COO of MEDITECH, told EHRIntelligence. “Generative AI can help auto-populate the discharge note by bringing in the discrete information that would be most relevant to substantiate that narrative and enable time savings for those clinicians.”
Many Applications for Generative AI in Healthcare
According to technology consulting and solutions firm XenonStack, generative AI has many potential applications in healthcare including:
The technology is currently in its early stages and does present challenges, such as lack of interpretability, the need for large datasets and more transparency, and ethical concerns, all of which will need to be addressed.
“We see it as a translation tool,” Lindemann told EHRIntelligence. “It’s not a panacea, but there’s going to be really valuable use cases, and the sooner the community can agree on that, the more useful the technology’s going to be.”
Since generative AI can be used to automate manual work processes, clinical laboratories and anatomic pathology groups should be alert to opportunities to interface their LISs with referring physicians’ EHRs. Such interfaces may enable the use of the generative AI functions to automate manual processes in both the doctors’ offices and the labs.
Research results call into question the safety and dependability of using artificial intelligence in medical diagnosis, a development that should be watched by clinical laboratory scientists
ChatGPT, an artificial intelligence (AI) chatbot that returns answers to written prompts, has been tested and found wanting by researchers at the University of Florida College of Medicine (UF Health) who looked into how well it could answer typical patient questions on urology. Not good enough according to the researchers who conducted the study.
AI is quickly becoming a powerful new tool in diagnosis and medical research. Some digital pathologists and radiologists use it for data analysis and to speed up diagnostic modality readings. It’s even been said that AI will improve how physicians treat disease. But with all new discoveries there comes controversy, and that’s certainly the case with AI in healthcare.
Many voices in opposition to AI’s use in clinical medicine claim the technology is too new and cannot be trusted with patients’ health. Now, UF Health’s study seems to have confirmed that belief—at least with ChatGPT.
The study revealed that answers ChatGPT provided “fell short of the standard expected of physicians,” according to a UF Health new release, which called ChatGPT’s answers “flawed.”
The questions posed were considered to be common medical questions that patients would ask during a visit to a urologist.
The researchers believes their study is the first of its kind to focus on AI and the urology specialty and which “highlights the risk of asking AI engines for medical information even as they grow in accuracy and conversational ability,” UF Health noted in the news release.
“I am not discouraging people from using chatbots,” said Russell S. Terry, MD (above), an assistant professor in the UF College of Medicine’s department of urology and the study’s senior author, in a UF Health news release. “But don’t treat what you see as the final answer. Chatbots are not a substitute for a doctor.” Pathologists and clinical laboratory managers will want to monitor how developers improve the performance of chatbots and other applications using artificial intelligence. (Photo copyright: University of Florida.)
UF Health ChatGPT Study Details
UF Health’s study featured 13 of the most queried topics from patients to their urologists during office visits. The researchers asked ChatGPT each question three times “since ChatGPT can formulate different answers to identical queries,” they noted in the news release.
The urological conditions the questions covered included:
The researchers then “evaluated the answers based on guidelines produced by the three leading professional groups for urologists in the United States, Canada, and Europe, including the American Urological Association (URA). Five UF Health urologists independently assessed the appropriateness of the chatbot’s answers using standardized methods,” UF Health noted.
Notable was that many of the results were inaccurate. According to UF Health, only 60% of responses were deemed appropriate from the 39 evaluated responses. Outside of those results, the researchers noted in their Urology paper, “[ChatGPT] misinterprets clinical care guidelines, dismisses important contextual information, conceals its sources, and provides inappropriate references.”
When asked, for the most part ChatGPT was not able to accurately provide the sources it referenced for its answers. Apparently, the chatbot was not programmed to provide such sources, the UF Health news release stated.
“It provided sources that were either completely made up or completely irrelevant,” Terry noted in the new release. “Transparency is important so patients can assess what they’re being told.”
Further, “Only 7 (54%) of 13 topics and 21 (54%) of 39 responses met the BD [Brief DISCERN] cut-off score of ≥16 to denote good-quality content,” the researchers wrote in their paper. BD is a validated healthcare information assessment questionnaire that “provides users with a valid and reliable way of assessing the quality of written information on treatment choices for a health problem,” according to the DISCERN website.
ChatGPT often “omitted key details or incorrectly processed their meaning, as it did by not recognizing the importance of pain from scar tissue in Peyronie’s disease. As a result … the AI provided an improper treatment recommendation,” the UF Health study paper noted.
Is Using ChatGPT for Medical Advice Dangerous to Patients?
Terry noted that the chatbot performed better in some areas over others, such as infertility, overactive bladder, and hypogonadism. However, frequently recurring UTIs in women was one topic of questions for which ChatGPT consistently gave incorrect results.
“One of the more dangerous characteristics of chatbots is that they can answer a patient’s inquiry with all the confidence of a veteran physician, even when completely wrong,” UF Health reported.
“In only one of the evaluated responses did the AI note it ‘cannot give medical advice’ … The chatbot recommended consulting with a doctor or medical adviser in only 62% of its responses,” UF Health noted.
For their part, ChatGPT’s developers “tell users the chatbot can provide bad information and warn users after logging in that ChatGPT ‘is not intended to give advice,’” UF Health added.
Future of Chatbots in Healthcare
In UF Health’s Urology paper, the researchers state, “Chatbot models hold great promise, but users should be cautious when interpreting healthcare-related advice from existing AI models. Additional training and modifications are needed before these AI models will be ready for reliable use by patients and providers.”
UF Health conducted its study in February 2023. Thus, the news release points out, results could be different now due to ChatGPT updates. Nevertheless, Terry urges users to get second opinions from their doctors.
“It’s always a good thing when patients take ownership of their healthcare and do research to get information on their own,” he said in the news release. “But just as when you use Google, don’t accept anything at face value without checking with your healthcare provider.”
That’s always good advice. Still, UF Health notes that “While this and other chatbots warn users that the programs are a work in progress, physicians believe some people will undoubtedly still rely on them.” Time will tell whether trusting AI for medical advice turns out well for those patients.
The study reported above is a useful warning to clinical laboratory managers and pathologists that current technologies used in ChatGPT, and similar AI-powered solutions, have not yet achieved the accuracy and reliability of trained medical diagnosticians when answering common questions about different health conditions asked by patients.
Device is latest example that wearable healthcare devices are moving past simple biomarker monitoring and into the area of assisting in rehab
Companies unrelated to traditional clinical laboratory medicine continue to develop wearable devices that enable individuals to monitor their health while also alerting physicians and caregivers in real time when certain biomarkers are out of range.
One recent example is US biotechnology company STAT Health Informatics in Boston, which has developed a wearable device that monitors blood flow to the ear and face “to better understand symptoms such as dizziness, brain fog, headaches, fainting, and fatigue that occur upon standing,” according to a press release. The tiny device is worn in the ear and connects wirelessly to a smartphone app.
Johns Hopkins University clinically tested the STAT device, and according to Medical Device Network, “It can predict a person fainting minutes before it happens and can be worn with more than 90% of devices that go in or around the ear. It can also be left in while sleeping and showering, meaning less likelihood of removing the device and forgetting to replace it.”
Another notable aspect of this invention is that it’s an example of how the ongoing miniaturization of various technologies makes it possible to invent smaller devices but with greater capabilities. In the case of the STAT device, it combines tiny sensors, Bluetooth, and an equally tiny battery to produce a device that fits in the ear and can function for up to three days before needing a recharge.
It’s easy to imagine these technologies being used for other types of diagnostic testing devices that could be managed by clinical laboratories.
“It’s well understood that the ear is a biometric gold mine because of its close proximity to the brain and major arteries. This allows for new biometrics … to be possible,” said Daniel Lee (above), co-founder and CEO of STAT Health, in a press release. “In addition, the ear is largely isolated from data corruption caused by arm motion—a problem that plagues current wearables and prevents them from monitoring heart metrics during many daily tasks. The ear is really the ideal window into the brain and heart.” Clinical laboratory managers may want to watch how this technology is further developed to incorporate other biomarkers for diseases and health conditions. (Photo copyright: STAT Health.)
How STAT Works
Every time the wearer stands, the STAT device tracks the change in response of blood pressure, heart rate, and blood flow to the head. “The device distills all this information into an ‘Up Score’ to track time spent upright. Its ‘Flow Score’ helps users pace their recovery by watching for blood flow abnormalities,” MassDevice reported.
According to the company’s website, STAT is intended for use in individuals who have been diagnosed with conditions known to suffer from drops in blood flow to the head, such as:
As an individual continues to use the device, STAT “learns about each user’s unique body to provide personalized coaching for healthy lifestyle choices,” MassDevice reported.
Another key factor is the technology built into the device. An optical sensor was chosen over ultrasound because STAT Health felt it was both easy to use and provided precise measurements accessing the shallow ear artery, MassDevice reported.
“Despite its small scale, the device incorporates advanced optical sensors, an accelerometer, a pressure sensor, temperature sensors, artificial intelligence (AI)-edge computing, three-day battery life (or more), and a micro solar panel,” Medical Device Network noted.
STAT’s image above demonstrates how truly minute the company’s wearable device is, even though it monitors blood flow to the face and ear looking for signs that the wearer is about to suffer bouts of dizziness or lightheadedness due to a drop in blood flow. (Photo copyright: STAT Health Informatics Inc.)
STAT’s Impact on Users’ Health
STAT’s developers intend the device to help individuals stay on track with their health. “The target population can navigate their condition better. If they’re not standing when they can, they will become deconditioned. This product encourages standing and being upright where possible, as part of rehab,” Lee told Medical Device Network.
Lee has been developing wearable in-ear devices for many years.
“Nobody has realized the ear’s true potential due to the miniaturization and complex systems design needed to make a practical and user-friendly ear wearable,” he told MassDevice. “After multiple engineering breakthroughs, we’ve succeeded in unlocking the ear to combine the convenience and long-term nature of wearables with the high fidelity nature of obtrusive clinical monitors. No other device comes close along the axis of wearability and cardiac signal quality, which is why we believe STAT is truly the world’s most advanced wearable.”
For clinical laboratories, though STAT is not a diagnostic test, it is the latest example of how companies are developing wearable monitoring devices intended to allow individuals to monitor their health. It moves beyond the simple monitoring of Apple Watch and Fitbit. This device can aid individuals during rehab.
Wearable healthcare devices will continue to be introduced that are smaller, allow more precise measurements of target biomarkers, and alert wearers in real time when those markers are out of range. Keeping in tune with the newest developments will help clinical laboratories and pathologists find new ways to support healthcare providers who recommend these devices for monitoring their patients conditions.