Acceptance of digital pathology and whole-slide imaging is now almost universal among academic health center pathology departments and the nation’s largest pathology companies
Across the United States, many private practice anatomic pathology groups now recognize that digital pathology is the path forward for the entire profession. During the past decade, most academic pathology departments and large pathology lab companies have incorporated digital pathology (DP) and whole-slide imaging (WSI) into many of their labs’ daily activities.
However, in community hospital-based anatomic pathology groups, there have been barriers to even the partial adoption of digital pathology. The two biggest barriers are well-known and discussed frequently at conferences and in the literature.
Some Pathologists Reluctant to Give Up Light Microscopes
One recognized barrier to wider adoption of DP is the reluctance of many long-serving pathologists to give up their familiar light microscopes and glass slides so they can make the transition to reading pathology images on a computer screen. These pathologists remain loyal to the tools and workflows that have served them well throughout their careers.
They generally oppose their group’s move to digital pathology when the subject is discussed in partner meetings and strategic retreats. Since many pathology groups require 100% of partners or shareholders to approve major business decisions, even one recalcitrant and stubborn pathologist-partner can block the motion to adopt digital pathology that is supported by most partners.
The second barrier is the fully-loaded cost to acquire, validate, implement, and use a digital pathology system with whole-slide imaging. A full-featured scanner can cost $250,000 or more and acquiring all the software, systems, and tools needed by a group to fully incorporate digital pathology into daily workflow can easily total $500,000 to $1,000,000.
This substantial commitment of a pathology group’s capital can trigger the same intense debates as the original question of whether the pathologists in the group should adopt DP and WSI. And, not surprisingly, in most pathology groups the same dynamics come into play when votes are tallied on the motion for the pathology group to commit the funds necessary to acquire a digital pathology system, the scanners, and associated tools.
Just one or two partner holdouts can block the decision to spend the money, despite that most of the pathologist partners are ready to make the commitment.
More Community Pathology Groups Considering Digital Pathology
Yet, the momentum in favor of adopting DP and WSI continues to build. “Those pathology labs that are early adopters report multiple clinical and financial benefits. These can include generating positive financial outcomes—including the ability to attract new clients, increasing case referrals, and generating new sources of revenue to the group. In turn, the increased revenue can allow the group to increase pathologist compensation,” said Robert L. Michel, Editor-in-Chief of Dark Daily and its sister publication The Dark Report.
Every day, more anatomic pathologists in the United States use a digital pathology system with a workstation (like above) to view whole-slide images and manage their daily caseload. Most academic center pathology departments use digital pathology, as do many of the nation’s largest pathology lab companies. (Photo copyright: WizardHealth.)
“We are in a time when health insurers are hammering away at the reimbursement paid to anatomic pathologists,” Michel continued. “Year after year, payers cut reimbursement for technical component and professional component services. They exclude many pathology groups from payer networks. That is why more community pathology groups are recognizing several important benefits with the use of DP and WSI that can increase a pathology group’s revenue and boost its pathologist compensation.
Community Pathology Groups Can Use Digital Pathology to Add Value
Equally important, there are specific ways that digital pathology and whole-slide imaging increase the value of the clinical services pathologists deliver to their client physicians. These dual benefits of DP are often overlooked—or not discussed—when community pathology groups conduct their annual retreats and debate the key points of when to adopt—and how to fund—a digital pathology system for their group. These benefits range from giving physicians a faster diagnostic answer on their cancer cases to helping the group’s subspecialist pathologists get more case referrals from physicians in other states.
“It’s important for all surgical pathologists to recognize several realities in today’s pathology marketplace,” Michel noted. “First, almost every sector in healthcare is digitizing itself. Reinforcing this trend is the federal government’s mandates for interoperability across EHRs, HISs, and LISs. Any private pathology group practice that lags in its adoption of digital capabilities and digital images will find itself falling farther and farther behind as physicians switch their case referrals to other pathology labs that have converted to digital pathology and whole-slide images.
“Second, pathology groups that adopt DP and WSI put themselves in a position to build market share in their service region, while at the same time increasing case referrals for their in-house subspecialist pathologists from throughout the United States,” Michel continued. “Also, when the histology is done locally, the local pathology group can deliver faster diagnostic answers and provide digital images as appropriate to referring physicians and hospitals in that region without the need to transport glass slides by couriers.
“Third—and this is an often-overlooked benefit of digital pathology—the local pathology group with DP and WSI can recruit today’s graduating pathology residents and fellows who have trained on DP and WSI. These new pathologists typically limit their job search to pathology groups that have gone digital,” Michel noted. “Millennial pathologists trained with digital images in their residency program. They are eager to work with the automated image analysis algorithms now coming to market.”
On Thursday, May 27, at 1:00 PM EDT, Keith Kaplan, MD, Chief Medical Officer of Corista (left), Andrew Evans, MD, Medical Director of Laboratory Medicine at Mackenzie Health (center left), William DeSalvo, President of Collaborative Advantage Consulting and Manager of Histology Operations at Sonora Quest Laboratories in Tempe, Ariz. (center right), and Lisa-Jean Clifford, COO and Chief Strategy Officer at Gestalt Diagnostics (right) will present “Adopting Digital Pathology on a Budget: Getting Started, Knowing What’s Feasible, and Funding Your DP from Overlooked Sources.” Anatomic pathologists, clinical laboratory directors, laboratory managers, clinical pathologists, and laboratory technicians will gain a critical understanding of which components a fully integrated digital pathology system requires, the differences between your lab’s existing LIS and a digital pathology system, budget-minded approaches to buying the components of a digital pathology system and implementing them in a stepwise fashion, and much more! (Photo copyright: Dark Daily.)
Recognizing the significant capital investment needed to acquire and deploy digital pathology and WSI, one goal of the webinar’s panel of experts is to identify ways that pathology groups can go digital on a budget. “We will do our best to identify different ways that pathology groups with limited financial resources can get into digital pathology,” said Keith Kaplan, MD, Chief Medical Officer at Corista in Concord, Mass., who will chair the upcoming webinar. “This may be the first public presentation where there is candid information about different financial strategies that your pathology group can utilize to acquire the scanners, the DP systems, and the associated tools needed for a full conversion to daily digital pathology.”
Don’t overlook how your participation in this webinar can be the foundation for helping your pathology group practice develop a timely, cost-effective path forward to introduce digital pathology and whole-slide imaging. Use of DP and WSI can become an important factor in helping your group offset payer prices cuts, develop new clients and sources of revenue, and increase pathologist compensation.
Click HERE to register today (or copy and paste this URL into your browser: https://www.darkdaily.com/webinar/adopting-digital-pathology-on-a-budget/). Make sure to have your pathology practice administrator and your histology manager join you for this important webinar.
As consumer demand increases for medical laboratory testing services that bypass the supervision of primary care doctors, clinical laboratories may be affected
Direct-to-consumer (DTC) genetic testing organizations and telecommunications companies in South Korea are collaborating to help consumers stay informed of their health status by sending lab test results directly to their mobile devices without requiring physician involvement. What can labs in the West learn from these developments?
Founded in 2015, NGeneBio provides smartphone-based healthcare services for individuals who solicit genetic testing. Through the partnership, KT plans to combine its knowledge of artificial intelligence (AI) and cloud computing with NGeneBio’s genetic decoding expertise to “provide services such as tailored health management (diet and exercise therapy) services, and storage and management of personal genome analysis information.”
No Doctors Involved?
Outside of genealogy, the general intent of DTC genetic testing is to equip consumers with certain genetic data that may help them manage their healthcare without requiring visits to their healthcare provider. The healthcare information provided through the NGeneBio venture will include data delivered directly to customers’ smartphones on the status of their:
skin,
hair,
nutrition, and
muscular strength.
According to an article in Korean business news publication Pulse, “Genetic test services in Korea are restricted to some 70 categories, such as the analysis of the risk of hair loss, high blood pressure, and obesity.”
Last September, Pulse reported, Korean mobile carrier SK Telecom Co. announced a similar partnership with Macrogen Inc. to introduce a mobile app-based DNA testing service called “Care8 DNA.” To utilize this service, consumers order a DNA test kit, take a saliva sample via mouth swab, and then send the kit to a clinical laboratory for analysis. Users typically receive their test results on the Care8 DNA app (available from both Google Play and Apple’s App Store) within a few weeks.
The service costs ₩8,250 South Korean won ($7.36 US) per month. A one-year subscription to the service costs ₩99,000 won or $88.36 US. The Care8 DNA app features 29 testing services, including:
skin aging,
possibility of hair loss,
resistance to nicotine,
the body’s recovery speed after exercise,
and more.
Along with those results, consumers can receive personalized health coaching guidance from professionals like nutritionists and exercise physiologists to improve their overall wellbeing, Pulse noted.
KoreaTechToday reports that the Macrogen/SK Telcom Care8 DNA app (above) “links the consumer immediately to a gene testing company instead of going through a medical institute first. BIS Research [a marketing research and intelligence company located in Freemont, Calif.] estimates the global direct-to-consumer (DTC) gene test market would increase to ₩7.6 trillion won in 2028.” That is more than $6.7 billion US dollars. Such a shift toward DTC home testing would likely have a huge financial impact on clinical laboratories that process genetic tests as well as the healthcare providers who order them. (Photo copyright: SK Telecom Co.)
In February 2019, Macrogen became the first company in South Korea to take advantage of the government’s relaxed regulations on DTC genetic testing, Korea Biomedical Review reported. In addition to the basic services offered through the Care8 DNA app, Macrogen’s DTC tests also can cover 13 diseases, including:
Other Korean Genetic Testing Companies Adding DTC Services
“Industry officials think DTC genetic tests should include testing for diseases,” an industry official told Korea Biomedical Review in April. “There will be more companies who make these attempts.”
“A DTC genetic test is a contactless healthcare service suitable for the COVID-19 era. The expansion of detailed test items allows users to comprehensively check nutrients, obesity, skin, hair, eating habits, and exercise characteristics at one time,” an official at Theragen Bio told Korea Biomedical Review. “We expect that our service will attract more attention from consumers.”
What Can Be Learned?
Countries in Asia—particularly South Korea, Japan, and Taiwan—are among the fastest adopters of new technology in the world. Thus, it can be instructive to see how their consumers use healthcare differently than in the West, and how those users embrace new technologies to help them manage their health.
It is not certain how all this will impact clinical laboratories and genetic doctors in the western nations. Direct-to-consumer genetic testing has had its ups and downs, as Dark Daily reported in multiple e-briefings.
Nevertheless, these developments are worth watching. Worldwide consumer demand for genetic home testing, price transparency, and easy access to test results on mobile devices is increasing rapidly.
Adopting Digital Pathology on a Budget: Getting Started, Knowing What’s Feasible, and Funding Your DP from Overlooked Sources 90-MINUTE LIVE WEBINAR WITH Q&A Held Thursday, May 27 | Available on DVD or On-Demand Hosted by: ORDER DVD OR ON-DEMAND Different paths to digital pathology can contribute new streams of revenue and increase pathologists’ compensation It’s time to consider adopting digital pathology! Today’s scanners and digital pathology systems are attractive for...
Oddly, as upcoding severity levels have risen, reported higher-severity inpatient hospital stays have dropped, OIG reported
Medicare upcoding fraud is a growing problem for the federal Centers for Medicare and Medicaid Services (CMS). Now, a report from the US Department of Health and Human Services (HHS) Office of Inspector General (OIG) suggests that the practice is increasingly occurring for high-severity inpatient hospital stays that account for the most expensive part of US healthcare.
“The [COVID-19] pandemic has placed unprecedented stress on the country’s healthcare system, making it more important than ever to ensure that Medicare dollars are spent appropriately,” the OIG report states.
The OIG website notes, “Medicare pays for many physician services using Evaluation and Management (commonly referred to as “E/M”) codes. New patient visits generally require more time than follow-up visits for established patients, and therefore E/M codes for new patients command higher reimbursement rates than E/M codes for established patients.”
The OIG describes one type of upcoding as “… an instance when [providers] provide a follow-up office visit or follow-up inpatient consultation, but bill using a higher-level E/M code as if [they] had provided a comprehensive new patient office visit or an initial inpatient consultation.
“Another example of upcoding related to E/M codes is misuse of Modifier 25,” the OIG continued. “Modifier 25 allows additional payment for a separate E/M service rendered on the same day as a procedure. Upcoding occurs if a provider uses Modifier 25 to claim payment for an E/M service when the patient care rendered was not significant, was not separately identifiable, and was not above and beyond the care usually associated with the procedure.”
How OIG Conducted the Study of Hospital Coding Practices
To perform its research, the OIG analyzed Medicare Part A claims for hospital stays for the six-year period from fiscal year (FY) 2014 through FY 2019. The OIG identified trends in billing and payments for inpatient hospital stays at the highest severity levels, as determined by the Medicare Severity Diagnosis Related Group (MS-DRG).
The OIG investigation revealed that the number of hospital stays billed at the highest severity level increased almost 20% between 2014 and 2019, while the number of stays billed at other severity levels decreased. These expenditures accounted for nearly half of all Medicare spending on inpatient hospital stays, the OIG reported.
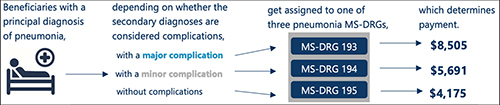
According to the OIG report, “Medicare pays hospitals more for beneficiaries in MS-DRGs with higher severity levels because they are typically more costly to treat.” The graphic above taken from the OIG report illustrates “how the presence of complications can affect Medicare payment for three beneficiaries with the same principal diagnosis.” (Graphic copyright: Federal Office of Inspector General Department of Health and Human Services.)
As Severity Levels Went Up, Inpatient Length of Stays Went Down
Interestingly, the average length of inpatient stays at the highest severity level decreased, and the average length of hospital stays overall remained largely the same, decreasing by just 0.1 days. In addition, the total number of inpatient hospital stays decreased by 5%.
The OIG report noted that “the increase in the number of stays billed at the highest severity level implies that beneficiaries were sicker overall. However, the decrease in the average length of stays at the highest severity level potentially undermines that idea because it is not consistent with sicker beneficiaries. Length of stay generally has a positive relationship to severity of stay; sicker beneficiaries stay in the hospital longer.”
The OIG confirmed that in FY 2019, Medicare spent $109.8 billion for 8.7 million hospital stays. Approximately 3.5 million (or 40%) of those stays were billed at the highest severity level, as determined by the MS-DRG. In addition, nearly half of the $109.8 billion spent, or $54.6 billion, was for stays billed at the highest severity level and Medicare paid an average of $15,500 per stay at that level.
The OIG report states that “stays at the highest severity level are vulnerable to inappropriate billing practices, such as upcoding—the practice of billing at a level that is higher than warranted. Specifically, nearly a third of these stays lasted a particularly short amount of time and over half of the stays billed at the highest severity level had only one diagnosis qualifying them for payment at that level. Further, hospitals varied significantly in their billing of these stays, with some billing much differently than most.”
The OIG study also found that over half of the inpatient stays billed at the highest severity level achieved that level due to only one diagnosis. According to the OIG, the severity of an inpatient stay depends on a patient’s secondary diagnosis and it only takes one secondary diagnosis to propel a patient into the highest severity level. The OIG determined that if the diagnosis was inaccurate or inappropriate, higher payments would not be warranted.
OIG Recommends CMS Conduct Targeted Reviews
The report found that the most frequently billed MS-DRG in FY 2019 was septicemia or severe sepsis and that hospitals billed for 581,000 of these stays, for which Medicare paid $7.4 billion. In addition, kidney and urinary tract infections, pneumonia, and renal failure were among the most common conditions to have a complication that led to a high severity classification.
In its report, the OIG recommended more oversight from CMS to ensure that Medicare dollars are spent appropriately. The OIG also suggests that CMS conduct targeted reviews of MS-DRGs and hospital stays that are vulnerable to upcoding, as well as the hospitals that frequently bill them.
Clinical Laboratories Are Forewarned
Medicare audits continue to be more detailed and rigorous and all healthcare providers—including clinical laboratories and anatomic pathology groups—should be prepared to present all necessary documentation to support claims if and when they are audited.
Improvements in software, machine learning, and artificial intelligence (AI) give Medicare officials and the OIG powerful tools to spot questionable provider billing. This includes medical laboratories whose billing patterns could arouse suspicions and trigger audits.
Upcoding is a long-standing problem for the Medicare program. What is changing is that federal officials now have better tools and resources to use in identifying patterns of upcoding that fall outside accepted parameters.
By mining results of unrelated blood tests, the CIRRUS algorithm can inform doctors and patients earlier than usual of liver disease
For years Dark Daily and its sister publication The Dark Report have predicted that the same type of analytical software used on Wall Street to analyze bundles of debt, such as car loans, mortgages, and installment loans, would eventually find application in healthcare and clinical laboratory medicine. Now, researchers at the University of Southampton in England have developed just such an analytical tool.
The UK researchers call their algorithm CIRRUS, which stands for CIRRhosis Using Standard tests. It can, they say, accurately predict if a patient has cirrhosis of the liver at a much earlier stage than usual and produce information that is clinically actionable, using results from several common, routinely-ordered medical laboratory tests.
The University of Southampton scientists published their findings in BMJ Open.
Currently, the leading edge for this in clinical laboratory medicine is analysis of digital pathology images using image analysis tools and artificial intelligence (AI). However, CIRRUS is an example that analytical software is advancing in its ability to mine data from a number of clinically-unrelated lab tests on a patient and identify a health condition that might otherwise remain unknown.
The UK researchers designed the CIRRUS algorithm using routine clinical laboratory blood tests often requested in general practice to identify individuals at risk of advanced liver disease. These tests include:
“More than 80% of liver cirrhosis deaths are linked to alcohol or obesity and are potentially preventable,” noted Nick Sheron, MD, FRCP, Head of Population Hepatology at University of Southampton, and lead author of the study, in a press release. “However, the process of developing liver cirrhosis is silent and often completely unsuspected by GPs [general practitioners]. In 90% of these patients, the liver blood test that is performed is normal, and so liver disease is often excluded.
“This new CIRRUS algorithm can find a fingerprint for cirrhosis in the common blood tests done routinely by GPs,” he continued. “In most cases the data needed to find these patients already exists and we could give patients the information they need to change their lifestyle. Even at this late stage, if people address the cause by stopping drinking alcohol or reducing their weight, the liver can still recover.”
Mining Clinical Laboratory Blood Test Results
To perform the study, the research team analyzed data on blood test results for nearly 600,000 patients. Unlike most diagnostic liver algorithms, the CIRRUS model was created using a dataset comprised of patients from both primary and secondary care without the main intent of preselecting for liver disease. This renders it better suited for detecting liver disease outside a secondary care hepatology environment.
“Whilst we are all preoccupied with the coronavirus pandemic we must not lose sight of other potentially preventable causes of death and serious illness,” said Michael Moore, BM, BS, MRCP, FRCGP, Professor of Primary Health Care Research and Head of Academic Unit Primary Care and Population Sciences at University of Southampton, in the press release. Professor Moore co-authored the CIRRUS study.
“This test using routine blood test data available, gives us the opportunity to pick up serious liver disease earlier, which might prevent future emergency admission to hospital and serious ill health,” he said.
Cirrhosis (shown above in a trichrome stained micrograph) is a condition in which the liver is scarred and permanently damaged. As the condition progresses, more scar tissue replaces healthy liver tissue. This accumulated scar tissue prevents the liver from doing its primary job of regulating chemical levels in the blood and excreting bile, a substance which helps eliminate toxins from the body and breaks down fats during digestion. As cirrhosis worsens, the liver begins to fail. (Photo copyright: Wikipedia.)
According to the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), cirrhosis is most common in adults ages 45 to 54 and about 1 in 400 adults in the US live with the disease. However, the actual number may be much higher as many people are not aware they have cirrhosis, because they do not experience symptoms until the liver is badly damaged.
The NIDDK reports complications from cirrhosis include:
Portal Hypertension, a condition where scar tissue partially blocks the normal flow of blood through the liver,
“Liver cirrhosis is a silent killer. The tests used most by GPs are not picking up the right people and too many people are dying preventable deaths. We looked at half a million anonymous records and the data we needed to run CIRRUS was already there in 96% of the people who went on to have a first liver admission,” stated Sheron in the press release. “With just a small change in the way we handle this data it should be possible to intervene in time to prevent many of these unnecessary deaths.”
“Alcohol-related liver diseases are far and away the most significant cause of alcohol-specific deaths, yet currently the vast majority of people find out that their liver is diseased way too late,” said Richard Piper, PhD, Chief Executive of Alcohol Change UK, a British charity and campaign group dedicated to reducing harm caused by alcohol abuse. “What is needed is a reliable means of alerting doctors and their patients to potential liver disease as early as possible. The CIRRUS process shows real promise, and we want to see it further developed, tested and implemented, to help save hundreds of thousands, if not millions, of lives.”
CIRRUS is a true milestone in the development of computer-assisted healthcare diagnostics. It will need more research, but the University of Southampton study shows that analytical software tools can mine clinical laboratory test results that were ordered for unrelated diagnostics and identify existing health conditions that might otherwise remain hidden to the patient’s physicians.