New ‘simple’ pricing scheme will provide transparency and value to all stakeholders, says company’s Chief Pharmacy Officer
Woonsocket, R.I.-based CVS Health (NYSE:CVS) is planning to scrap what it says is an old-school prescription reimbursement model and turn to a new way to price prescription medications at its 9,000 CVS pharmacies nationwide. Why is this relevant for clinical laboratory and pathology managers? It shows the disruption that is ongoing in healthcare.
Like clinical laboratories, retail pharmacies have significant reimbursement, competition, and labor challenges to address. But unique to retail pharmacies is the emergence of pharmacy benefit management (PBM) companies that work between health insurance plans and drug makers.
“National pharmacy chains found themselves disintermediated from providing prescriptions to patients by pharmacy benefit management (PBM) companies. By 2021, PBMs had captured $484 billion of the total prescription drug spending of $576.9 billion. That meant PBMs controlled 84% of the prescription drug market! That caused retail pharmacies to look for new sources of revenue,” noted Dark Daily’s sister publication The Dark Report.
This arrangement may be motivating retail pharmacy companies to seek ways to recover the volume lost to PBMs.
CVS’ new CostVantage model will work with a formula based on how much CVS paid for the drug, a set markup over those costs, and a fee for pharmacy services to fill the prescription, according to a news release. Some experts and publications have compared the change to the approach used by the Mark Cuban Cost Plus Drug Company.
CVS Health expects to start CostVantage in 2024 before introducing it to PBMs for commercial payers in 2025.
CVS is “committed to lowering drug pricing,” CVS Health Chief Executive Officer Karen Lynch (above), CVS Health’s President and Chief Executive Officer, told CNBC. “What this (the new model) does is it essentially aligns the economics of our pricing for drugs to what consumers will pay at the pharmacy counter,” she added. Clinical laboratory managers and pathologists should understand that this new pricing strategy may be an attempt by CVS to win back prescription business lost to pharmacy benefit management companies. (Photo copyright: Rick Burn/Wikipedia.)
CVS Aims for Value and Transparency
CVS Health’s leaders believe it is time for a change in how the company’s pharmacies are reimbursed by PBMs and other payers.
Generic drugs dispensed in CVS pharmacies reached 90%. “That limits the capacity or the amount of value remaining through the higher levels of generic dispensing,” he said.
Also branded drugs have risen in price about 40% since 2019, leading to “higher costs for patients, our customers’ plans, and PBM plan sponsors.”
“This model has reached an inflection point that is just ripe for change,” Shah said. “We’re changing this outdated reimbursement model that made sense for the last decade, but no longer works today or in the future. We’re introducing a new simple model that provides value for all stakeholders across the supply chain in a much more simple, transparent, and comprehensive way,” he continued.
Cost-Plus Plans versus Retail Drug Prices
Fierce Healthcare compared CVS CostVantage to the Mark Cuban Cost Plus Drug Company, which claims it offers prescription drugs at prices below traditional pharmacies and openly shares with customers the “15% markup over its cost, plus pharmacy fees.”
Some examples on the company’s website include: Abiraterone acetate (generic for Zytiga), a prostate cancer treatment. It is priced at $33.50, compared to $1,093 retail. Cost Plus Drug Company says its costs are:
Manufacturing: $24.60
15% markup: $3.90
Pharmacy labor fee: $5.00
Another drug offered is canagliflozin (generic for Invokana), a type 2 diabetes medication, which sells for $245.92, compared to $676.14 retail. Cost Plus Drug Company says its costs are:
Fein predicts there will be more cost-plus models by retail pharmacies. “Other large pharmacies will likely follow CVS with attempts to force payers and PBMs to accept some form of cost-plus reimbursement,” he wrote.
Fein noted pharmacies prefer cost-plus models for reasons including the “stripping away of complexity and hidden cross-subsidies. … For a pharmacy, the same PBM would pay the same price for the same prescription regardless of the PBM’s arrangement with different plan sponsors.”
Turbulent Retail Pharmacy Market
CVS has also been dealing with limited growth, pharmacist labor relations issues, and a decline in COVID-19 testing, Healthcare Dive reported.
Meanwhile, pharmacies have been closing store sites and affiliated physician practices. CVS announced plans to close 900 stores between 2022 and 2024, according to a news release.
Rite Aid Corporation, Philadelphia, announced last year that it had filed for bankruptcy and may eventually close 400 to 500 of its 2,100 stores.
Walgreens Boots Alliance, Deerfield, Ill., intends to close 150 US and 300 United Kingdom locations, according to its former Chief Financial Officer James Kehoe’s remarks in a third quarter 2023 earnings call transcribed by Motley Fool.
The turbulence in the retail pharmacy market is another sign of ongoing disruption in healthcare. Long-established sectors are experiencing market shifts that are eroding their access to patients and ability to generate adequate profits.
Understanding how pharmacies approach these issues may help medical laboratory and pathology managers develop strategies for adding value to their relationships with healthcare providers and insurance plans.
Lack of regular clinical laboratory screenings in this age group at least partially to blame, researchers say
While cervical cancer rates have seen a 50-year decline overall, that trend is shifting among 30- to 40 year-olds who have experienced a near 2% increase from 2012-2019. This finding comes from a 2024 American Cancer Society (ACS) report that is eyeing the timeline of the human papillomavirus (HPV) vaccines and the lack of clinical laboratory cancer screenings as possible contributors to this new trend.
Though a 2% increase is significant, the study, which was published in CA: ACancer Journal for Clinicians, titled “Cancer Statistics, 2024,” noted that these cancers were “mostly early, curable tumors,” epidemiologist Ahmedin Jemal DVM, PhD, Senior Vice President Surveillance and Health Equity Science at ACS, and senior author of the new report, told NBC News.
To understand how the increase in cancer rates impacts this age group, consider the numbers: “About 13,800 American women are diagnosed with cervical cancer each year and 4,360 die from the disease,” NBC reported.
US vaccination programs for youths have lagged behind nations that have embraced HPV vaccination to positive results.
Australia, for example, has vaccinated a high proportion of its youth since the vaccine was first released in 2006. In 2023, the nation created its National Strategy for the Elimination of Cervical Cancer in Australia program and expects cervical cancer to be fully eliminated there by 2035.
For lab professionals, this demonstrates how new technologies like the HPV test and vaccine can alter how individuals are screened for diseases, and how vaccines can reduce and even eliminate diseases that were once common.
“We need to make sure we are not forgetting about that generation that was a little too old for HPV vaccination,” Jennifer Spencer, PhD (above), Assistant Professor, Department of Population Health and Department Internal Medicine, Dell Medical School, University of Texas at Austin, told NBC News. “The onus is on the healthcare system to think about who is slipping through the cracks,” she added. Lack of clinical laboratory screenings among the 30-40 age group may be contributing to the increase in cervical cancer rates. (Photo copyright: Dell Medical School.)
Lack of Clinical Laboratory Screenings
Research points to a lag in cervical cancer screenings as a possible cause for the recent rise in cases. Timely screening allows doctors to both identify and remove any worrisome lesions before they become cancerous, Jennifer Spencer, PhD, Assistant Professor of the Department of Population Health, Dell Medical School, University of Texas at Austin, told NBC News.
Screenings for women ages 21-65 have fallen 15% since 2000, according to data from the National Cancer Institute. Also, more than half of women with cervical cancer have “either never been screened or haven’t been screened in the past five years, according to the Centers for Disease Control and Prevention,” NBC reported.
The US Preventative Services Task Force recommends that women 21-29 years of age should receive Pap smears every three years. Women 30-65 years of age should do the same, or every five years with an HPV test or combo test.
Despite a decrease in cervical cancer, 29% of women in their 20s are overdue to get screening, NBC noted. This was the age group most likely to be lagging on getting screened. Spencer says that this delay in screening could explain the resulting increase in cervical cancer among the 30-40 age group.
Causes for Lack in Screenings
Regardless of age group, women who were uninsured, in a rural area, non-white, or identifying as lesbian, bisexual, or gay were also more likely to be overdue on screenings, according to Spencer’s study.
In addition, women who just moved to the United States may have missed their screenings, thus increasing risk, epidemiologist Nicholas Wentzensen, MD, PhD, Deputy Director, Senior Investigator, and Head of the Clinical Epidemiology Unit at the National Cancer Institute, told NBCNews.
Additionally, Spencer found in her research that confusion exists by both patients and doctors on when cervical screening should take place. Some participants in her study did not have screening recommended by their doctors, while others simply did not recognize it was necessary.
“When women in one of Spencer’s studies were asked why they hadn’t been screened recently, they commonly said that they didn’t know they needed to be screened or that a health provider hadn’t recommended it. Only 1% [of] women ages 21 to 29 said they had skipped screening because they had received the HPV shot,” NBC News reported.
A 2022 Journal of American Medicine (JAMA) report also looked at screenings as a possible cause. Those researchers found that “only 73% of women with abnormal screening results received follow-up care,” NBC reported.
“If the increase (in cases) is real, it could be a result of missed screening opportunities at earlier ages, as suggested by the increase in squamous cell carcinoma and localized disease. It may also stem from a decrease in screening at younger ages,” the JAMA study authors wrote.
HPV Vaccine and Cervical Cancer Prevention
The HPV vaccine is another important area of research to be considered. Approved in 2006, HPV vaccines were beneficial because HPV “causes six types of cancer, including cervical cancer,” NBC reported.
Women in their early 20s at that time were the first generation to benefit from HPV vaccines, NBC noted. It may be that they continue to benefit in a decrease in cervical cancer among their cohort.
Countries that have emphasized HPV vaccines and stringent screenings in their cancer prevention efforts are reaping the benefits of that policy.
Though cancer screening and the HPV vaccine are important first steps women should take to prevent cervical cancer, follow-through clinical laboratory testing and diagnosis is crucial, Spencer added. This would include additional testing and treatment for any abnormal results of the cancer screening.
However, according to Spencer, “only 73% of women with abnormal screening results received follow-up care,” NBC reported.
Healthcare policymakers today are emphasizing the need for providers to identify and close gaps in care as a way to improve patient outcomes and help control the cost of care. Women who are overdue for a cervical cancer screening test—whether an HPV test or Pap smear—have this care gap. This creates an opportunity for clinical labs to add value.
Clinical laboratories could be helpful during this period by looking at patient files to note which patients are overdue for screenings and then alerting their doctors. Medical labs also could work directly with doctors to establish a program to reach out to patients. Labs would thus be adding value as well as benefitting patients.
This may be a new ‘sign of the times’ as hospitals, clinical laboratories, and other healthcare providers working with AI find they also need to hire their own prompt engineers
AI “prompting,” according to Florida State University, “refers to the process of interacting with an AI system by providing specific instructions or queries to achieve a desired outcome.”
According to workable.com, prompt engineers specialize “in developing, refining, and optimizing AI-generated text prompts to ensure they are accurate, engaging, and relevant for various applications. They also collaborate with different teams to improve the prompt generation process and overall AI system performance.”
Healthcare institutions are getting more serious about using AI to improve daily workflows and clinical care, including in the clinical laboratory and pathology departments. But adopting the new technology can be disruptive. To ensure the implementation goes smoothly, hospitals are now seeking prompt engineers to guide the organization’s strategy for using AI.
When Boston Children’s Hospital leaders set out to find such a person, they looked for an individual who had “a clinical background [and] who knows how to use these tools. Someone who had experience coding for large language models and natural language processing, but who could also understand clinical language,” according to MedPage Today.
“We got many, many applications, some really impressive people, but we were looking for a specific set of skills and background,” John Brownstein, PhD, Chief Innovation Officer at Boston Children’s Hospital and Professor of Biomedical Informatics at Harvard Medical School, told MedPage Today.
“It was not easy to find [someone]—a bit of a unicorn-type candidate,” noted Brownstein, who is also a medical contributor to ABC News.
After a four-month search, the hospital hired Dinesh Rai, MD, emergency room physician and AI engineer, for the position. According to Brownstein, Rai had “actually practiced medicine, lived in a clinical environment,” and had “successfully launched many [AI] applications on top of large language models,” MedPage Today reported.
“Some of the nuances I bring to the table in terms of being a physician and having worked clinically and understanding really deeply the clinical workflows and how we can implement the [AI] technology—where its limits are, where it can excel, and the quickest way to get things [done],” Dinesh Rai, MD (above), told MedPage Today. “I’m happy to be able to help with all of that.” Hospital clinical laboratory and pathology managers may soon by engaging with prompt engineers to ensure the smooth use of AI in their departments. (Photo copyright: LinkedIn.)
Prompt Engineers are like F1 Drivers
“It’s kind of like driving a car, where basically anyone can drive an automatic car, and anyone can go onto ChatGPT, write some text, and get a pretty solid response,” said Rai, describing the act of AI prompting to MedPage today.
Then, there are “people who know how to drive manual, and there are people who will know different prompting techniques, like chain-of-thought or zero-shot prompting,” he added. “Then you have those F1 drivers who are very intimate with the mechanics of their car, and how to use it most optimally.”
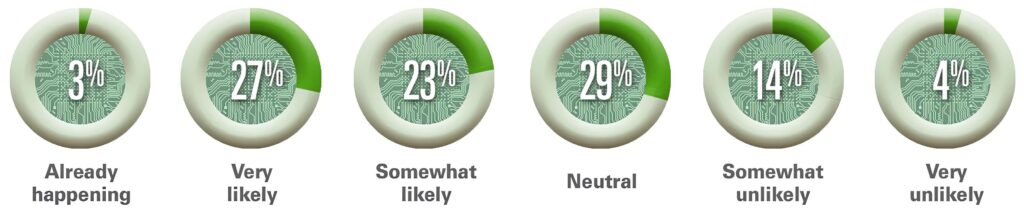
The American Hospital Association (AHA) believes that AI “holds great promise in helping healthcare providers gain insights and improve health outcomes.” In an article titled, “How AI Is Improving Diagnostics, Decision-Making and Care,” the AHA noted that, “Although many questions remain regarding its safety, regulation, and impact, the use of AI in clinical care is no longer in its infancy and is expected to experience exponential growth in the coming years.
“AI is improving data processing, identifying patterns, and generating insights that otherwise might elude discovery from a physician’s manual effort. The next five years will be critical for hospitals and health systems to build the infrastructure needed to support AI technology, according to the recently released Futurescan 2023,” the AHA wrote.
The graphic above is taken from the American Hospital Association’s article about Futurescan’s 2023 survey results on AI in healthcare. “Healthcare executives from across the nation were asked how likely it is that by 2028 a federal regulatory body will determine that Al for clinical care delivery augmentation (e.g., assisted diagnosis and prescription, personalized medication and care) is safe for use by our hospital or health systems,” AHA stated. This would include the use of AI in clinical laboratories and pathology group practices. (Graphic copyright: American Hospital Association.)
The AHA listed the top three opportunities for AI in clinical care as:
Clinical Decision Tools: “AI algorithms analyze a vast amount of patient data to assist medical professionals in making more informed decisions about care.”
Diagnostic and Imaging: The use of AI “allows healthcare professionals to structure, index, and leverage diagnostic and imaging data for more accurate diagnoses.”
Patient Safety: The use of AI improves decision making and optimizes health outcomes by evaluating patient data. “Systems that incorporate AI can improve error detection, stratify patients, and manage drug delivery.”
The hiring of a prompt engineer by Boston Children’s Hospital is another example of how AI is gaining traction in clinical healthcare. According to the Futurescan 2023 survey, nearly half of hospital CEOs and strategy leaders believe that health systems will have the infrastructure in place by 2028 to successfully utilize AI in clinical decision making.
“I’m lucky to [be] in an organization that has recognized the importance of AI as part of the future practice of medicine,” Rai told MedPage Today.
Pathologists and managers of clinical laboratories and genetic testing companies will want to track further advancements in artificial intelligence. At some point, the capabilities of future generations of AI solutions may encourage labs to hire their own prompt engineers.
Groups representing academic publishers are taking steps to combat paper mills that write the papers and then sell authorship spots
Clinical laboratory professionals rely on peer-reviewed research to keep up with the latest findings in pathology, laboratory medicine, and other medical fields. They should thus be interested in new efforts to combat the presence of “research paper mills,” defined as “profit oriented, unofficial, and potentially illegal organizations that produce and sell fraudulent manuscripts that seem to resemble genuine research,” according to the Committee on Publication Ethics (COPE), a non-profit organization representing stakeholders in academic publishing.
“They may also handle the administration of submitting the article to journals for review and sell authorship to researchers once the article is accepted for publication,” the COPE website states.
In a recent example of how paper mills impact scholarly research, multinational publishing company John Wiley and Sons (Wiley) announced in The Scholarly Kitchen last year that it had retracted more than 1,700 papers published in journals from the company’s Hindawi subsidiary, which specializes in open-access academic publishing.
“In Hindawi’s case, this is a direct result of sophisticated paper mill activity,” wrote Jay Flynn, Wiley’s Executive Vice President and General Manager, Research, in a Scholarly Kitchen guest post. “The extent to which our processes and systems were breached required an end-to-end review of every step in the peer review and publishing process.”
In addition, journal indexer Clarivate removed 19 Hindawi journals from its Web of Science list in March 2023, due to problems with their editorial quality, Retraction Watch reported.
Hindawi later shut down four of the journals, which had been “heavily compromised by paper mills,” according to a blog post from the publisher.
Wiley also announced at that time that it would temporarily pause Hindawi’s special issues publishing program due to compromised articles, according to a press release.
“We urgently need a collaborative, forward-looking and thoughtful approach to journal security to stop bad actors from further abusing the industry’s systems, journals, and the communities we serve,” wrote Jay Flynn (above), Wiley EVP and General Manager, Research and Learning, in an article he penned for The Scholarly Kitchen. “We’re committed to addressing the challenge presented by paper mills and academic fraud head on, and we invite our publishing peers, and the many organizations that work alongside us, to join us in this endeavor.” Clinical laboratory leaders understand the critical need for accurate medical research papers. (Photo copyright: The Scholarly Kitchen.)
Using AI to Detect Paper Mill Submissions
Wiley acquired Hindawi in 2021 in a deal valued at $298 million, according to a press release, but the subsidiary has since become a financial drain for the company.
The journals earn their revenue by charging fees to authors. But in fiscal year 2024, which began last fall, “Wiley expects $35-40 million in lost revenue from Hindawi as it works to turn around journals with issues and retract articles,” Retraction Watch reported, citing an earnings call.
Wiley also revealed that it would stop using the Hindawi brand name and bring the subsidiary’s remaining journals under its own umbrella by the middle of 2024.
The service will incorporate tools to detect signs that submissions originated from paper mills, including similarities with “known papermill hallmarks” and use of “tortured phrases” indicating that passages were translated by AI-based language models, according to a press release.
These tools include:
Papermill Similarity Detection: Checks for known papermill hallmarks and compares content against existing papermills papers.
Problematic Phrase Recognition: Flags unusual alternatives to established terms.
Unusual Publication Behavior Detection: Identifies irregular publishing patterns by paper authors.
Researcher Identity Verification: Helps detect potential bad actors.
Gen-AI Generated Content Detection: Identifies potential misuse of generative AI.
Journal Scope Checker: Analyzes the article’s relevance to the journal.
The company said that the new service will be available through Research Exchange, Wiley’s manuscript submission platform, as early as next year.
Other Efforts to Spot Paper Mill Submissions
Previously, STM announced the launch of the STM Integrity Hub, with a mission “to equip the scholarly communication community with data, intelligence, and technology to protect research integrity,” Program Director Joris van Rossum, PhD, told The Scholarly Kitchen.
In 2023, the group announced that the hub would integrate Papermill Alarm from Clear Skies, a paper mill detection tool launched in 2022 with a focus on cancer research. It uses a “traffic-light rating system for research papers,” according to a press release.
In an announcement about the launch of Wiley’s Papermill Detection service, Retraction Watch suggested that one key to addressing the problem would be to reduce incentives for authors to use paper mills. Those incentives boil down to the pressure placed on many scientists, clinicians, and students to publish manuscripts, according to the research report from STM and COPE.
In one common scenario, the report noted, a paper mill will submit a staff-written paper to multiple journals. If the paper is accepted, the company will list it on a website and offer authorship spaces for sale.
“If a published paper is challenged, the ‘author’ may sometimes back down and ask for the paper to be retracted because of data problems, or they may try to provide additional supporting information including a supporting letter from their institution which is also a fake,” the report noted.
All of this serves as a warning to pathologists and clinical laboratory professionals to carefully evaluate the sources of medical journals publishing studies that feature results on areas of healthcare and lab medicine research that are of interest.
Trifecta of forces at work that will affect the clinical laboratory and pathology industries have been described as a ‘perfect storm’ requiring lab and practice managers to be well informed
Digital pathology, artificial intelligence (AI) in healthcare, and the perfect storm of changing federal regulations, took centerstage at the 29th Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management in New Orleans this week, where more than 1,000 clinical laboratory and pathology leaders convened over three days.
This was the largest number of people ever onsite for what has become the world’s largest event focused exclusively on lab management topics and solutions. Perhaps the highlight of the week was the federal Food and Drug Administration’s (FDA’s) announcement of its final rule on Laboratory Developed Tests (LDTs). Overall, the conference featured more than 120 speakers, many of them national thought leaders on the topic of clinical lab and pathology management. More than 65% of the audience onsite were executive level lab managers.
“The level of interest in the annual Executive War College is testimony to the ongoing need for dynamic, engaging, and highly relevant conference events,” said Robert Michel (above), Editor-in-Chief of Dark Daily and its sister publication The Dark Report, and founder of the Executive War College. “These in-person gatherings present great opportunities for clinical laboratory and pathology managers and leaders to network and speak with people they otherwise might not meet.” (Photo copyright: Dark Intelligence Group.)
Demonstrating Clinical Value
For those who missed the action onsite, the following is a synopsis of the highlights this week.
Lâle White, Executive Chair and CEO of XiFin, spoke about the future of clinical laboratory testing and the factors reshaping the industry. There are multiple dynamics impacting healthcare economics and outcomes—namely rising costs, decreasing reimbursements, and the move to a more consumer-focused healthcare. But it is up to labs, she said, to ensure their services are not simply viewed as a commodity.
“Laboratory diagnostics have the potential to change the economics of healthcare by really gaining efficiencies,” she noted. “And it’s up to labs to demonstrate clinical value by helping physicians manage two key diagnostic decision points—what tests to order, and what to do with the results.”
But even as labs find ways to increase the value offered to clinicians, there are other disruptive factors in play. Consumer-oriented tech companies such as Google, Apple, and Amazon are democratizing access to patient data in unforeseen ways, and Medicare Advantage plans are changing the way claims are processed and paid.
Clinical labs are fundamental components of the public health infrastructure. So, the CDC plans on focusing on delivering high-quality laboratory science, supported by reliable diagnostics and informatics for disease outbreaks and exposures, and engaging with public and private sector partners.
The history of MolDX and Z-Codes were the topics discussed by Gabriel Bien-Willner, MD, PhD, Chief Medical Officer for healthcare claims and transaction processing company Palmetto GBA. Molecular testing is highly complex, and the lack of well-defined billing codes and standardization makes it difficult to know if a given test is reasonable and necessary.
Z-Codes were established to clarify what molecular testing was performed—and why—prompting payers to require both Z-Codes and Current Procedural Terminology (CPT) codes when processing molecular test claims. Medicare’s MolDX program further streamlines the claims process by utilizing expertise in the molecular diagnostics space to help payers develop coverage policies and reimbursement for these tests.
FDA Final Rule on LDT Regulation
Timothy Stenzel, MD, PhD, CEO of Grey Haven Consulting and former director of the FDA’s Office of In Vitro Diagnostics reviewed the latest updates from the FDA’s Final Rule on LDT (laboratory developed test) regulation. Prior to the FDA releasing its final rule, some experts suggested that the new regulations could result in up to 90% of labs discontinuing their LDT programs, impacting innovation, and patient care.
However, the final rule on LDTs is very different from the original proposed rule which created controversy. The final rule actually lowers the regulatory burden to the point that some labs may not have to submit their LDTs at all. The FDA is reviewing dozens of multi-cancer detection assays, some of which have launched clinically as LDTs. The agency is likely to approve those that accurately detect cancers for which there is no formal screening program.
Stenzel explained the FDA’s plan to down-classify most in vitro diagnostic tests, changing them from Class III to Class II, and exempting more than 1,000 assays from FDA review. He also discussed the highlights of the Quality Management System Regulation (QMSR). Launched in January, the QMSR bought FDA requirements in line with ISO 13485, making compliance easier for medical device manufacturers and test developers working internationally.
Looming Perfect Storm of Regulatory Changes
To close out Day 1, Michel took to the stage again with a warning to clinical laboratories about the looming “Perfect Storm” trifecta—the final FDA ruling on LDTs, Z-Code requirements for genetic testing, and updates to CLIA ’92 that could result in patient data being considered a specimen.
Laboratory leaders must think strategically if their labs are to survive the fallout, because the financial stress felt by labs in recent years will only be exacerbated by macroeconomic trends such as:
Staff shortages,
Rising costs,
Decreasing and delayed reimbursements, and
Tightening supply chains.
Lab administrators looking for ways to remain profitable and prosperous should look beyond the transactional Clinical Lab 1.0 fee-for-service model and adopt Clinical Lab 2.0, which embraces HEDIS (Healthcare Effectiveness Data and Information Set) scores and STAR ratings to offer more value to Medicare Advantage and other payers.
Wednesday’s General Session agenda was packed with information about the rise of artificial intelligence, big data, and precision medicine in healthcare. Taking centerstage on the program’s final day was Michael Simpson, President and CEO of Clinisys. Simpson gave a global perspective on healthcare data as the new driver of innovation in diagnostics and patient care.