Switching from non-profit to for-profit may affect how clinical laboratories operate in the new healthcare system
Shifting away from fee-for-service payment models and towards value-based healthcare is the goal of many non-profit hospital systems. One such transformation is underway at Summa Health, one of the largest integrated delivery networks (IDNs) in Ohio. On January 17, venture capital firm General Catalyst announced that its subsidiary—Health Assurance Transformation Corporation (HATCo)—had entered into an agreement to purchase Summa Health.
“HATCo’s investment into Summa Health will drive not only near-term benefit to the organization and the patients it serves but also sustainable, long-term transformation through a true shift to value-based care and access to new revenue streams, resources, innovations, and technologies,” states a General Catalyst news release penned by Marc Harrison, MD, CEO of HATCo.
Harrison was formerly President and CEO of Intermountain Healthcare, a 33 hospital not-for-profit IDN in Salt Lake City, Utah. This is a noteworthy fact because Intermountain Health has a national reputation as an innovative multi-hospital health system. Some observers believe that Harrison’s involvement signals that General Catalyst believes it has a care model that can deliver better patient care in a profitable manner.
“Under its new structure, Summa will become a for-profit organization, and General Catalyst says it will introduce new tech-enabled solutions that aim to make care more accessible and affordable,” CNBCreported.
“This is the first time that anybody has done anything quite like this,” Harrison told CNBC. “There are many digital health solutions that are out there as point solutions. This is the first holistic transformation of a health system to a thoughtful combination of digital and in-person care.”
“Our intent is to build on and augment the system’s considerable strengths. First and foremost, we share Summa Health’s commitment to serving all members of the community,” wrote HATCo CEO Marc Harrison, MD (above), in a news release. “The Summa Health team also shares our belief that achieving healthcare transformation will require a shift to value-based care … Together, we intend to demonstrate that a model that is better for patients can also be good for business, creating a blueprint for other health systems to effectively serve all people in their communities.” How this shift will affect Summa’s clinical laboratories remains to be seen. (Photo copyright: General Catalyst.)
Betting on Healthcare
In 2023, General Catalyst, an American venture capital firm headquartered in Cambridge, Mass., unveiled its Health Assurance Transformation Corporation (HATCo) and began shopping for a health system to buy.
HATCo has 20 healthcare systems in a network that spans 43 states and four countries, according to Healthcare Dive. The company’s news release states it has been focused on three areas since its start-up:
Helping its partners on their “transformation journeys.”
Planning to “acquire and operate a health system for the long-term.”
“The goal of the purchase is for the health system to act as a proving ground for General Catalyst to test ways to improve hospital operations and patient care, without risk aversion or cash shortfalls, management said,” Healthcare Dive reported.
Thus, the firm’s announcement to purchase a health system last October “sent shockwaves through the healthcare industry” according to Healthcare Dive.
“At its core, General Catalyst’s long-term Health Assurance thesis is that value-based care not only is good for patients, but also can be a successful business model if deployed with innovative technology at meaningful scale. Its rationale for buying a health system is a belief that it can improve on the traditional model of not-for-profit health system governance and management by embedding new incentives,” wrote Christopher Kerns, CEO and co-founder of Washington, D.C-based research firm Union Healthcare Insight, in a blog post analysis.
General Catalyst’s HATCo may offer up “a profit motive, a longer time horizon, and a channel for dozens of innovative companies to demonstrate value,” he noted.
“The single biggest barrier to promising young healthcare companies is an inability to scale. Many of their innovations—in digital health, patient engagement, revenue cycle workflow, etc.—require willing health system partners who are famously conservative in their investments and service providers, and rarely take risks on newbies. The addition of Summa provides an open laboratory for those innovations,” Kerns added.
Is the Summa Health Deal Good for Healthcare?
Some in the industry were taken aback by General Catalyst’s announcement.
“A lot of people feel like a PE (private equity) or venture capital company owning a hospital is kind of like asking Freddy Krueger to come babysit your kids. It just makes people a little nervous, and it doesn’t feel quite aligned with this concept of healthcare being a human right,” John Bass, CEO of Hashed Health, a Nashville, Tenn.-based healthcare venture studio, told CNBC.
Nevertheless, it’s a moot point. HATCo is moving forward with its purchase of Summa Health.
“For this bet to work, Summa will have to be a solid proving ground for [General Catalyst’s] portfolio companies. And that means either Summa itself will have to grow, or it will have to act as a force multiplier for its other value-based portfolio companies to justify the considerable capital expended. I have to say, that’s a tall order, but not an insane one,” said Kerns in the Union Healthcare Insight blog post.
Healthcare managers may find it interesting to follow HATCo and Summa Health on their planned journey. The results may speak for themselves. Either way, clinical laboratories and anatomic pathology group practices in HATCo’s health system may be in for some interesting changes.
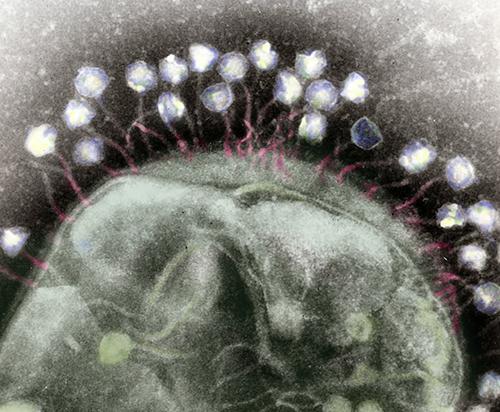
Phages are miniscule, tripod-looking viruses that are genetically programmed to locate, attack, and eradicate a specific kind of pathogen. These microscopic creatures have saved lives and are being touted as a potential solution to superbugs, which are strains of bacteria, viruses, parasites, and fungi that are resistant to most antibiotics and other treatments utilized to counteract infections.
“These multi-drug-resistant superbugs can cause chronic infections in individuals for months to years to sometimes decades,” Dwayne Roach, PhD, Assistant Professor of Bacteriophages, Infectious Disease, and Immunology at SDSU told CNN. “It’s ridiculous just how virulent some of these bacteria get over time.”
Labs across the country are conducting research on phages in eradicating superbugs. Roach’s lab is currently probing the body’s immune response to phages and developing purification techniques to prepare phage samples for intravenous use in patients.
“There are a lot of approaches right now that are happening in parallel,” said Dwayne Roach, PhD (above), Assistant Professor of Bacteriophages, Infectious Disease, and Immunology at San Diego State University (SDSU), in a CNN interview. “Do we engineer phages? Do we make a phage cocktail, and then how big is the cocktail? Is it two phages or 12 phages? Should phages be inhaled, applied topically, or injected intravenously? There’s a lot of work underway on exactly how to best do this.” Clinical laboratories that test for bacterial infections may play a key role in diagnosis and treatment involving bacteriophages. (Photo copyright: San Diego State University.)
Building Libraries of Phages
When certain a bacterial species or its genotypes needs to be annihilated, a collection of phages can be created to attack it via methods that enter and weaken the bacterial cell. The bacteria will attempt to counter the intrusion by employing evasive actions, such as shedding outer skins to eliminate the docking ports utilized by the phages. These maneuvers can cause the bacteria to lose their antibiotic resistance, making them vulnerable to destruction.
Some research labs are developing libraries of phages, accumulating strains found in nature in prime breeding grounds for bacteria to locate the correct phage for a particular infection. Other labs, however, are speeding up the process by producing phages in the lab.
“Rather than just sourcing new phages from the environment, we have a bioreactor that in real time creates billions upon billions of phages,” Anthony Maresso, PhD, Associate Professor at Baylor College of Medicine in Houston told CNN. “Most of those phages won’t be active against the drug-resistant bacteria, but at some point, there will be a rare variant that has been trained, so to speak, to attack the resistant bacteria, and we’ll add that to our arsenal. It’s a next-generation approach on phage libraries.”
For the Baylor study, 12 patients were treated with phages customized to each individual’s unique bacterial profile. The antibiotic-resistant bacteria were exterminated in five of the patients, while several others showed improvement.
Clinical trials are currently being executed to test the effectiveness of phages against a variety of chronic health conditions, including:
Using a phage cocktail could be used to treat a superbug outbreak in real time, while preventing a patient from a future infection of the same superbug.
“The issue is that when patients have infections with these drug-resistant bacteria, they can still carry that organism in or on their bodies even after treatment,” Maroya Walters, PhD, epidemiologist at the federal Centers for Disease Control and Prevention (CDC) told CNN.
“They don’t show any signs or symptoms of illness, but they can get infections again, and they can also transmit the bacteria to other people,” she added.
The colorized transmission electron micrograph above shows numerous phages attached to a bacterial cell wall. Phages are known for their unique structures, which resemble a cross between NASA’s Apollo lunar lander and an arthropod. (Caption and photo copyright: Berkeley Lab.)
More Studies are Needed
According to CDC data, more than 2.8 million antimicrobial-resistant (AMR) infections occur annually in the United States. More than 35,000 people in the country will die as a result of these infections.
In addition, AMR infections are a huge global threat, associated with nearly five million deaths worldwide in 2019. Resistant infections can be extremely difficult and sometimes impossible to treat.
More research is needed before phages can be used clinically to treat superbugs. But if phages prove to be useful in fighting antibiotic-resistant bacteria, microbiologists and their clinical laboratories may soon have new tools to help protect patients from these deadly pathogens.
Forces in play will directly impact the operations and financial stability of many of the nation’s clinical laboratories
With significant regulatory changes expected in the next 18 to 24 months, experts are predicting a “Perfect Storm” for managers of clinical laboratories and pathology practices.
Currently looming are changes to critical regulations in two regulatory areas that will affect hospitals and medical laboratories. One regulatory change is unfolding with the US Food and Drug Administration (FDA) and the other regulatory effort centers around efforts to update the Clinical Laboratory Improvement Amendments of 1988 (CLIA).
The major FDA changes involve the soon-to-be-published Final Rule on Laboratory Developed Tests (LDTs), which is currently causing its own individual storm within healthcare and will likely lead to lawsuits, according to the FDA Law Blog.
In a similar fashion—and being managed under the federal Centers for Medicare and Medicaid Services (CMS)—are the changes to CLIA rules that are expected to be the most significant since 2003.
The final element of the “Perfect Storm” of changes coming to the lab industry is the increased use by private payers of Z-Codes for genetic test claims.
In his general keynote, Robert L. Michel, Dark Daily’s Editor-in-Chief and creator of the 29th Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management, will set the stage by introducing a session titled, “Regulatory Trifecta Coming Soon to All Labs! Anticipating the Federal LDT Rule, Revisions to CLIA Regulations, and Private Payers’ Z-Code Policies for Genetic Claims.”
“There are an unprecedented set of regulatory challenges all smashing into each other and the time is now to start preparing for the coming storm,” says Robert L. Michel (above), Dark Daily’s Editor-in-Chief and creator of the 29th Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management, a national conference on lab management taking place April 30-May 1, 2024, at the Hyatt in New Orleans. (Photo copyright: The Dark Intelligence Group.)
Coming Trifecta of Disruptive Forces to Clinical Laboratory, Anatomic Pathology
The upcoming changes, Michel notes, have the potential to cause major disruptions at hospitals and clinical laboratories nationwide.
“Importantly, this perfect storm—which I like to describe as a Trifecta because these three disruptive forces that will affect how labs will conduct business—is not yet on the radar screen of most lab administrators, executives, and pathologists,” he says.
Because of that, several sessions at this year’s Executive War College conference, now in its 29th year, will offer information designed to give attendees a better understanding of how to manage what’s coming for their labs and anatomic pathology practices.
“This regulatory trifecta consists of three elements,” adds Michel, who is also Editor-in-Chief of Dark Daily’s sister publication The Dark Report, a business intelligence service for senior level executives in the clinical laboratory and pathology industry, as well in companies that offer solutions to labs and pathology groups.
According to Michel, that trifecta includes the following:
Element 1
FDA’s Draft LDT Rule
FDA’s LDT rule is currently the headline story in the lab industry. Speaking about this development and two other FDA initiatives involving diagnostics at the upcoming Executive War College will be pathologist Tim Stenzel, MD, PhD, former director of the FDA’s Office of In Vitro Diagnostics. It’s expected that the final rule on LDTs could be published by the end of April.
Stenzel will also discuss harmonization of ISO 13485 Medical Devices and the FDA’s recent memo on reclassifying most high-risk in vitro diagnostics to moderate-risk to ease the regulatory burden on companies seeking agency review of their diagnostic assays.
Salerno will also cover the CDC’s efforts to foster closer connections with clinical labs and their local public health laboratories, as well as the expanding menu of services for labs that his department now offers.
Element 3
Private Payer Use of Z-Codes for Test Claims
On the third development—increased use by private payers of Z-Codes for genetic test claims—the speaker will be pathologist Gabriel Bien-Willner, MD, PhD. He is the Medical Director of the MolDX program at Palmetto GBA, a Medicare Administrative Contractor (MAC). It is the MolDX program that oversees the issuance of Z-Codes for molecular and diagnostic tests.
UnitedHealthcare (UHC) was first to issue such a Z-Code policy last year, although it has delayed implementation several times. Other major payers are watching to see if UHC succeeds with this requirement, Michel says.
Other Critical Topics to be Covered at EWC
In addition to these need-to-know regulatory topics, Michel says that this year’s Executive War College will present almost 100 sessions and include 148 speakers. Some of the other topics on the agenda in New Orleans include the following and more:
Standardizing automation, analyzers, and tests across 25 lab sites.
Effective ways to attract, hire, and retain top-performing pathologists.
Leveraging your lab’s managed care contracts to increase covered tests.
“Our agenda is filled with the topics that are critically important to senior managers when it comes to managing their labs and anatomic pathology practices,” Michel notes.
“Every laboratory in the United States should recognize these three powerful developments are all in play at the same time and each will have direct impact on the clinical and financial performance of our nation’s labs,” Michel says. “For that reason, every lab should have one or more of their leadership team present at this year’s Executive War College to understand the implications of these developments.”
Visit here to learn more about the 29th Executive War College conference taking place in New Orleans.
Following the loss of its histology accreditation, pressure on APS laboratory continues to mount
Government-run healthcare systems around the world often under-invest as demand grows and new healthcare technologies enter clinical practice. One such example is taking place in New Zealand, where public pathology and medical laboratory services are under extreme stress as physician test orders exceed the ability of the island nation’s clinical laboratories to keep up.
“The escalating pressure is complicating what was already a very difficult rescue job at one of the country’s busiest labs—Community Anatomic Pathology Services (APS),” RNZ reported. In 2023, APS lost its histology accreditation after it came to light that lab workers were not only exposed to toxic chemical levels at the facility, but that patients were waiting weeks for test results to return from the lab.
“The service is in crisis mode and, without urgent investment … there is a real risk that it will fail. The changes required are of such urgency that it is recommended that they be placed at the top of the agenda,” the report reads, RNZ reported.
“The size of New Zealand’s economy is restricting what our country spends on health. Health is already the second highest demand on the New Zealand tax dollar,” wrote Andrew Blair, CMInstD (above), then General Manager of Royston Hospital, Hastings, New Zealand, in an article he penned for Jpn Hosp, the journal of the Japan Hospital Association. “The tolerance of New Zealanders would be challenged if a government attempted to increase taxes further to meet the growing demands for expenditure on health, but at the same time the population’s expectations are increasing. This is the challenging situation we face today.” For New Zealand’s clinical laboratories, the demand for testing is increasing annually as the country’s population grows. (Photo copyright: Blair Consulting.)
Increased Demand on APS Leads to Problems
Established in 2015, APS tests thousands of anatomic and tissue samples yearly and is utilized by approximately a third of NZ’s population, according to RNZ.
The big story, however, is that from 2022 to 2023 utilization increased by a third. “The overall increasing demand is greater than the capacity of the service,” Te Whatu Ora (Health New Zealand), the country’s publicly-funded healthcare system, told RNZ.
As planned care increased, public hospitals started outsourcing operations to private surgical centers. A domino effect ensued when all of those samples then made their way to APS. There was an “increased volume of private surgery being carried out by 600 specialists in the region and 2,000 general practitioners, with up to 450 histology cases a day,” RNZ noted, adding, “The backlog has hit turnaround times for processing samples, which had been deteriorating.”
To make matters even more dire, working conditions at the country’s clinical labs is unfavorable and deteriorating, with short staffing, outdated workspaces and equipment, and exposure to dangerous chemicals.
“Conditions got so bad from 2019-2021 that workers were exposed to cancer-causing formaldehyde in cramped workspaces, and flammable chemicals were stored unsafely,” RNZ reported.
While pay increases and safety improvements have provided some relief, the memory of past incidences coupled with increasing delays continue to undermine confidence in New Zealand’s laboratory industry.
Patients Also at Risk Due to Long Delays in Test Results
“We recognize the concern and impact any delayed results can cause referrers and their patients,” Health New Zealand said in a statement, RNZ reported.
Nevertheless, a 2023 article in The Conversation noted that, “38,000 New Zealanders had been waiting longer than the four-month target for being seen by a specialist for an initial assessment.”
However, according to plastic surgeon and Melanoma Network of New Zealand (MelNet) Chair Gary Duncan, MBChB, FRACS, when patients return to their doctors for test results, those results often have not come back from the medical laboratory. Therefore, the physician cannot discuss any issues, which causes the patient to have to make another appointment or receive a melanoma diagnosis over the telephone, RNZ reported.
“Slow pathology services are unfair to patients. Such delays could result in the spreading of the melanoma to other parts of the body and require major surgery under anesthetic,” dermatologist Louise Reiche, MBChB, FRACS, told RNZ. “Not only will they suffer an extensive surgical procedure, but it could also shorten their life.”
Improvements at APS Underway
Changes are currently underway that may decrease the long delays in test results at New Zealand’s labs. “A business case was being done to set up an electronic ordering system to cut down on manual processing errors,” RNZ reported.
Additionally, “the situation is much improved due to dispersal of work around [the] city and country for now. The teamwork around the region has been a veritable lifesaver,” a source familiar with the work told RNZ.
Construction of a new lab for APS is also allegedly in the works. However, to date no announcement has been made, according to RNZ.
Time will tell if New Zealand’s government can repair its pathology system. News stories showcasing damage caused by lengthy delays in clinical laboratory test results—and the ensuing patient harm due to rationed care in general—continue to reveal the weakness in government-run healthcare systems.
New non-invasive test could replace traditional painful spinal taps and clinical laboratory fluid analysis for diagnosis of Parkinson’s disease
Scientists at AXIM Biotechnologies of San Diego have added another specimen that can be collected non-invasively for rapid, point-of-care clinical laboratory testing. This time it is tears, and the diagnostic test is for Parkinson’s disease (PD).
The new assay measures abnormal alpha-synuclein (a-synuclein), a protein that is a biomarker for Parkinson’s, according to an AXIM news release which also said the test is the first rapid test for PD.
“The revolutionary nature of AXIM’s new test is that it is non-invasive, inexpensive, and it can be performed at a point of care. It does not require a lumbar puncture, freezing, or sending samples to a lab. AXIM’s assay uses a tiny tear drop versus a spinal tap to collect the fluid sample and the test can be run at a doctor’s office with quantitative results delivered from a reader in less than 10 minutes,” the news release notes.
“Furthermore, emerging evidence shows that a-synuclein assays have the potential to differentiate people with PD from healthy controls, enabling the potential for early identification of at-risk groups,” the news release continues. “These findings suggest a crucial role for a-synuclein in therapeutic development, both in identifying pathologically defined subgroups of people with Parkinson’s disease and establishing biomarker-defined at-risk cohorts.”
This is just the latest example of a disease biomarker that can be collected noninvasively. Other such biomarkers Dark Daily has covered include:
“With this new assay, AXIM has immediately become a stakeholder in the Parkinson’s disease community, and through this breakthrough, we are making possible new paradigms for better clinical care, including earlier screening and diagnosis, targeted treatments, and faster, cheaper drug development,” said John Huemoeller, CEO, AXIM (above), in a news release. Patients benefit from non-invasive clinical laboratory testing. (Photo copyright: AXIM Biotechnologies.)
Fast POC Test versus Schirmer Strip
AXIM said it moved forward with its novel a-synuclein test propelled by earlier tear-related research that found “a-synuclein in its aggregated form can be detected in tears,” Inside Precision Medicine reported.
But that research used what AXIM called the “outdated” Schirmer Strip method to collect tears. The technique involves freezing tear samples at -80 degrees Celsius (-112 Fahrenheit), then sending them to a clinical laboratory for centrifugation for 30 minutes; quantifying tear protein content with a bicinchoninic acid assay, and detecting a-synuclein using a plate reader, AXIM explained.
Alternatively, AXIM says its new test may be performed in doctors’ offices and offers “quantitative results delivered from a reader in less than 10 minutes.”
“Our proven expertise in developing tear-based diagnostic tests has led to the development of this test in record speed, and I’m extremely proud of our scientific team for their ability to expand our science to focus on such an important focus area as Parkinson’s,” said John Huemoeller, CEO, AXIM in the news release.
“This is just the beginning for AXIM in this arena,” he added. “But I am convinced when pharmaceutical companies, foundations, and neurologists see how our solution can better help diagnose Parkinson’s disease in such an expedited and affordable way, we will be at the forefront of PD research, enabling both researchers and clinicians a brand-new tool in the fight against PD.”
One of those tests was “a lateral flow diagnostic for point-of-care use that measures the level of lactoferrin proteins in tear fluid, which work to protect the surface of the eye. … Axim said that low lactoferrin levels have also been linked to Parkinson’s disease and that the assay can be used alongside its alpha-synuclein test,” Fierce Biotech noted.
“It made sense to try and look at the proteinaceous [consisting of or containing protein] constituents of tear fluid,” Lew told Neurology Live. “Tear fluid is easy to collect. It’s noninvasive, inexpensive. It’s not like when you do a lumbar puncture, which is a much more involved ordeal. There’s risk of contamination with blood (saliva is dirty) issues with blood and collection. [Tear fluid analysis] is much safer and less expensive to do.”
In Biomarkers in Medicine, Lew et al noted why tears make good biomarkers for Parkinson’s disease, including “the interconnections between the ocular [eye] surface system and neurons affected in Parkinson’s disease.”
The researchers also highlighted “recent data on the identification of tear biomarkers including oligomeric α-synuclein, associated with neuronal degeneration in PD, in tears of PD patients” and discussed “possible sources for its release into tears.”
Future Clinical Laboratory Testing for Parkinson’s
Parkinson’s disease is the second most common neurodegenerative disorder after Alzheimer’s. It affects nearly one million people in the US. About 1.2 million people may have it by 2030, according to the Parkinson’s Foundation.
Thus, an accurate, inexpensive, non-invasive diagnostic test that can be performed at the point of care, and which returns clinical laboratory test results in less than 10 minutes, will be a boon to physicians who treat PD patients worldwide.
Clinical laboratory managers and pathologists may want to follow AXIM’s future research to see when the diagnostic test may become available for clinical use.