Smaller cities and rural towns are finding the NWSS a useful early warning tool for tracking COVID-19 in their communities
In a move that mirrors similar programs around the world, the federal Centers for Disease Control and Prevention (CDC) now monitors sewage nationwide and records levels of SARS-CoV-2 in an effort to prevent new outbreaks of COVID-19 and spot any new variants of the coronavirus.
Advances in gene sequencing technologies are enabling the CDC’s National Wastewater Surveillance System (NWSS), and in many communities, clinical laboratories and health system laboratories have worked with local health authorities to test wastewater since onset of the pandemic.
“What started as a grassroots effort by academic researchers and wastewater utilities has quickly become a nationwide surveillance system with more than 34,000 samples collected representing approximately 53 million Americans,” noted epidemiologist Amy Kirby, PhD (above) during the telebriefing.
Kirby is a Senior Service Fellow in the Waterborne Disease Prevention Branch at the CDC.
“Currently, CDC is supporting 37 states, four cities, and two territories to help develop wastewater surveillance systems in their communities. More than 400 testing sites around the country have already begun their wastewater surveillance efforts,” she added.
“Estimates suggests between 40% and 80% of people with COVID-19 shed viral RNA in their feces, making wastewater and sewage an important opportunity for monitoring the spread of infection,” said epidemiologist Amy Kirby, PhD (above), a Senior Service Fellow in the Waterborne Disease Prevention Branch at the CDC. The NWSS’ findings could enable public health officials to better allocate mobile clinical laboratory testing and COVID-19 vaccination sites around the country. This would be especially beneficial in rural and underserved healthcare populations. (Photo copyright: Center for Global Safe Water, Sanitation, and Hygiene.)
Genetic Sequencing Enables Tracking of Virus and Bacteria
At the time of the telebriefing, the federal agency anticipated having an additional 250 sites online within a few weeks and even more sites added within the coming months. Many of the participating sites are sequencing the genes of their biological samples and reporting that data to the CDC.
“So, we’ve seen from very early days in the pandemic that rates of detection in wastewater correlate very well with other clinical indicators, like pace rates and hospitalization and test positivity,” Kirby stated. “That data continues to come in and it continues to be a very solid indicator of what’s going on in the community.”
Wastewater, also referred to as sewage, includes water from toilets, showers, and sinks that may contain human fecal matter and water from rain and industrial sources. To use the CDC’s wastewater surveillance system:
Wastewater is collected from a community area served by the surveillance system as it flows into a local water treatment plant.
Collected samples are sent to an environmental or public health laboratory where they are tested for SARS-CoV-2.
Health departments submit the testing data to the CDC through the online NWSS Data Collection and Integration for Public Health Event Response (DCIPHER) portal.
The DCIPHER system then analyzes the data and reports the results back to the health department for use in their COVID-19 response.
Beginning in February 2022, members of the public can view the results of collected data online through the CDC’s COVID Data Tracker.
Wastewater Sampling Is a ‘Critical Early Warning System’
According to the CDC NWSS website, there are many advantages to using wastewater surveillance in the fight against COVID-19, including:
Wastewater can capture the presence of the virus shed by people both with and without symptoms.
Health officials can determine if infections are increasing or decreasing within a certain monitoring site.
Wastewater surveillance does not depend on people having access to healthcare or the availability of COVID-19 testing.
It is possible to implement wastewater surveillance in many communities as nearly 80% of the US population are served by municipal wastewater collection systems.
“These built-in advantages can inform important public health decisions, such as where to allocate mobile testing and vaccination sites,” Kirby said. “Public health agencies have also used wastewater data to forecast changes in hospital utilization, providing additional time to mobilize resources and preparation for increasing cases.”
The wastewater sampling represents a critical early warning system for COVID-19 surges and variants, and the CDC hopes this type of sampling and research can be utilized in the future for other infectious diseases.
“Wastewater surveillance can be applicable to a wide variety of health concerns. And so, we are working to expand the National Wastewater Surveillance platform to use it for gathering data on other pathogens, and we expect that work to commence by the end of this year,” Kirby said. “Our targets include antibiotic resistance, foodborne infections like E. Coli, salmonella, norovirus, influenza, and the emerging fungal pathogen Candida Auris.”
Critical Surveillance Tool for Microbiology Laboratories
Independent of the nation’s network of public health laboratories, expansion of this program may give microbiology and clinical laboratories in smaller cities and rural towns an opportunity to test wastewater specimens in support of local wastewater monitoring programs.
As the CDC develops this surveillance network into a more formal program, microbiology labs may find it useful to learn which infectious diseases are showing up in their localities, often days or weeks before any patients test positive for the same infectious agents.
That would give pathologists and clinical laboratory leaders an early warning to be on the alert for positive test results of infectious diseases that wastewater monitoring has confirmed exist in the community.
According to the Centers for Disease Control and Prevention (CDC), the 1918 influenza (aka, the Spanish Flu) pandemic took place worldwide between 1918 and 1919. It was caused by the H1N1 virus (A/H1N1), a subtype of the Influenza A virus, and infected approximately 500 million people worldwide (a third of the human population at the time). Fifty million people died. Many were children or otherwise healthy individuals, but people from all age groups perished.
The CDC calls the Spanish Flu the “deadliest pandemic of the 20th century.” Past pandemics have generally concluded after 2.5 to 3.5 years. That’s how long it takes for new viruses to mutate and become endemic diseases, Healthline reported.
The COVID-19 pandemic has been around for about that long. It stands to reason the natural end of the COVID-19 pandemic may be just around the corner. But is it? And is the Omicron variant an indicator that the COVID-19 pandemic is winding down?
“Our analysis suggests that in the US, this combination of characteristics would lead to Omicron replacing Delta as the dominant variant in the next few months and to a higher peak burden of disease than the country saw in the second half of 2021 (but likely below the peak reached in the winter of 2020-21),” the report states.
McKinsey analysts also acknowledged the possible impact of new therapeutics, COVID-19 vaccine booster doses, and public health measures on Omicron spread. “In the short term, an accelerated rollout of booster doses of COVID-19 vaccines is likely to be one of the best protections against an Omicron-fueled wave of the disease,” the analysts wrote.
Does How the Spanish Flu Came to an End Mirror the COVID-19 Pandemic?
Virologists and infectious disease experts explained that the Spanish Flu virus did what viruses still do: mutate and become less dangerous. Herd immunity also helped end the 1918 pandemic.
“The 1918 influenza virus eventually mutated to the point of not having a high number of deaths—eventually over three years or so. We may very well be witnessing this process with ongoing variants of SARS-CoV-2,” virologist Rodney Rohde, PhD, Director of the Clinical Laboratory Science Program at Texas State University, told Healthline.
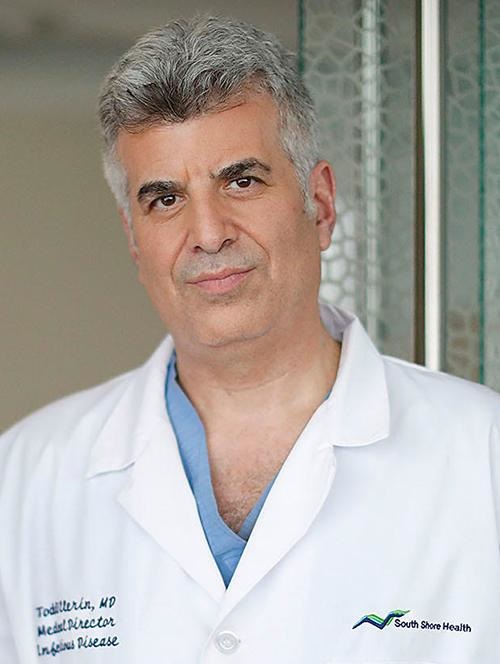
Today’s flu strains have “ancestral links” to the 1918 flu, and thus, the SARS-CoV-2 coronavirus will most likely also leave its mark, The Boston Herald reported. “The coronavirus will evolve and hopefully morph into a seasonal illness to which we pay little mind, but it’s still too early to tell,” Todd Ellerin, MD (above,) Director of Infectious Diseases, South Shore Health, South Weymouth, Mass., told The Boston Herald. (Photo copyright: Greg Derr/The Patriot Ledger.)
“If you think about the way viruses behave, biologically, their reason for living is to replicate and spread, and there’s really no advantage for the virus to kill the host,” infectious disease specialist Keith Armitage, MD, Professor of Medicine, Division of Infectious Diseases at Case Western Reserve University, told Healthline. “The hope is, that if the pandemic doesn’t go away, we will get new variants that are highly contagious but don’t produce much of a clinical illness,” he added.
In “2021’s Top 10 Lab Stories Confirm Important Trends,” Dark Daily’s sister publication, The Dark Report (TDR), posed a similar question in its number one story of 2021: “COVID-19: Will it Become Endemic and a Respiratory Virus that Shows Up Every Year like Influenza?”
“The question of whether SARS-CoV-2 is a pandemic that fades, as did SARS in 2003, or becomes endemic and a respiratory virus that shows up every season like influenza and the common cold, is of major concern to clinical lab administrators. That’s because clinical labs and pathology groups must continue to serve physicians and patients with the usual menu of routine, reference, and esoteric testing,” TDR noted.
Clinical Laboratories to Continue COVID Testing
It would be most helpful for medical laboratories and pathology groups to have some idea of when the pandemic will end. Unfortunately, such predictions would not be very useful.
“Since COVID-19 infections have a high number of asymptomatic transmitters, we may not fully understand how societal and environmental pressures—masks, distancing, remote working, etc.—on the virus will allow it to evolve,” Rohde told Healthline.
For now, clinical laboratories will need to continue to remain prepared as COVID-19 cases rise and people seek SARS-COV-2 tests, vaccinations, and treatments. COVID-19 testing is likely to be in demand throughout the coming year. The current surge in demand for COVID-19 tests is putting additional stress on the supply chain.
“We know pandemics end; it’s just a matter of time,” Sara Paton, PhD, Associate Professor of Epidemiology, Wright State University, told the Journal-News. “It could be in 2022, maybe later in the year, but I can’t say for sure. It could be 2023.”
Molecular probes designed to spot minute amounts of pathogens in biological samples may aid clinical laboratories’ speed-to-answer
Driven to find a better way to isolate minute samples of pathogens from among high-volumes of other biological organisms, researchers at Canada’s McMaster University in Hamilton, Ontario, have unveiled a bioinformatics algorithm which they claim shortens time-to-answer and speeds diagnosis of deadly diseases.
Two disease pathogens the researchers specifically targeted in their study are responsible for sepsis and SARS-CoV-2, the coronavirus causing COVID-19. Clinical laboratories would welcome a technology which both shortens time-to-answer and improves diagnostic accuracy, particularly for pathogens such as sepsis and SARS-CoV-2.
Their design of molecular probes that target the genomic sequences of specific pathogens can enable diagnosticians and clinical laboratories to spot extremely small amounts of viral and bacterial pathogens in patients’ biological samples, as well as in the environment and wildlife.
“There are thousands of bacterial pathogens and being able to determine which one is present in a patient’s blood sample could lead to the correct treatment faster when time is very important,” Zachery Dickson, a lead author of the study, told Brighter World. Dickson is a bioinformatics PhD candidate in the Department of Biology at McMaster University. “The probe makes identification much faster, meaning we could potentially save people who might otherwise die,” he added.
Sepsis is a life-threatening response to infection that leads to organ failure, tissue damage, and death in hospitals worldwide. According to Sepsis Alliance, about 30% of people diagnosed with severe sepsis will die without quick and proper treatment. Thus, a “shortcut” to identifying sepsis in its early stages may well save many lives, the McMaster researchers noted.
And COVID-19 has killed millions. Such a tool that identifies sepsis and SARS-CoV-2 in minute biological samples would be a boon to hospital medical laboratories worldwide.
“We currently need faster, cheaper, and more succinct ways to detect pathogens in human and environmental samples that democratize the hunt, and this pipeline does exactly that,” Hendrik Poinar, PhD (above), McMaster Professor of Anthropology and a lead author of the study, told Brighter World. Poinar is Director of the McMaster University Ancient DNA Center. Hospital medical laboratories could help save many lives if sepsis and COVID-19 could be detected earlier. (Graphic copyright: McMaster University.)
Is Bioinformatics ‘Shortcut’ Faster than PCR Testing?
The researchers say their probes enable a shortcut to detection—even in an infection’s early stages—by “targeting, isolating, and identifying the DNA sequences specifically and simultaneously.”
The probes’ design makes possible simultaneous targeted capture of diverse metagenomics targets, Biocompare explained.
But is it faster than PCR (polymerase chain reaction) testing?
The McMaster scientists were motivated by the “challenges of low signal, high background, and uncertain targets that plague many metagenomic sequencing efforts,” they noted in their paper.
They pointed to challenges posed by PCR testing, a popular technique used for detection of sepsis pathogens as well as, more recently, for SARS-CoV-2, the coronavirus causing COVID-19.
“The (PCR) technique relies on primers that bind to nucleic acid sequences specific to an organism or group of organisms. Although capable of sensitive, rapid detection and quantification of a particular target, PCR is limited when multiple loci are targeted by primers,” the researchers wrote in Cell Reports Methods.
According to LabMedica, “A wide array of metagenomic study efforts are hampered by the same challenge: low concentrations of targets of interest combined with overwhelming amounts of background signal. Although PCR or naive DNA capture can be used when there are a small number of organisms of interest, design challenges become untenable for large numbers of targets.”
Detecting Pathogens Faster, Cheaper, and More Accurately
As part of their study, researchers tested two probe sets:
one to target bacterial pathogens linked to sepsis, and
another to detect coronaviruses including SARS-CoV-2.
They were successful in using the probes to capture a variety of pathogens linked to sepsis and SARS-CoV-2.
“We validated HUBDesign by generating probe sets targeting the breadth of coronavirus diversity, as well as a suite of bacterial pathogens often underlying sepsis. In separate experiments demonstrating significant, simultaneous enrichment, we captured SARS-CoV-2 and HCoV-NL63 [Human coronavirus NL 63] in a human RNA background and seven bacterial strains in human blood. HUBDesign has broad applicability wherever there are multiple organisms of interest,” the researchers wrote in Cell Reports Methods.
The findings also have implications to the environment and wildlife, the researchers noted.
Of course, more research is needed to validate the tool’s usefulness in medical diagnostics. The McMaster University researchers intend to improve HUBDesign’s efficiency but note that probes cannot be designed for unknown targets.
Nevertheless, the advanced application of novel technologies to diagnose of sepsis, which causes 250,000 deaths in the US each year, according to the federal Centers for Disease Control and Prevention, is a positive development worth watching.
The McMaster scientists’ discoveries—confirmed by future research and clinical studies—could go a long way toward ending the dire effects of sepsis as well as COVID-19. That would be a welcome development, particularly for hospital-based laboratories.
Several young companies hope to expand the direct-to-consumer test market by introducing new diagnostic tests to serve the women’s health market
Providing women with at-home lab test kits is the goal of a growing class of start-up companies that are bringing to market consumer test kits for a range of health conditions common to women. These companies believe they can shift a substantial volume of such testing away from the nation’s medical laboratories.
Moreover, diagnostic startups that develop at-home direct-to-consumer (DTC) clinical laboratory genetic tests have been hot commodities among venture capitalists and other healthcare investors willing to put tens of millions of dollars into these new firms. The New York Times observed that, until recently, women’s healthcare needs have rarely been the focus of new diagnostic testing companies, but that the situation may be changing.
“Femtech” (short for female technology) products and services that address the health and wellness needs of women is the new buzz word in healthcare. It describes female-focused diagnostic startups aiming at vaginal health and other medical issues that go beyond reproductive health concerns.
This, however, is a dual-edged sword for clinical laboratory leaders. Growth in this segment could lead to new diagnostics tests that boost a medical lab’s bottom line or, conversely, it could reduce revenue as patients self-diagnose urinary tract infections (UTIs), yeast infections, and other conditions through at-home DTC testing.
“The market potential is huge,” Michelle Tempest, MD (above), a partner at the London-based healthcare consulting firm Candesic, told The New York Times. “There’s definitely an increasing appetite for anything in the world which is technology and a realization that female consumer power has arrived—and that it’s arrived in healthcare.” Tempest maintains the women’s health marketplace is ripe for growth, which could mean a boon for clinical laboratory testing and diagnostics designed specifically for women. (Photo copyright: Candesic.)
Vaginal Microbiome At-home Clinical Laboratory Tests in High Demand
One area in particular drawing the attention of several female-led startups is vaginal health. According to an article in Vogue, test developers Juno Bio and Evvy are leading the way with at-home vaginal microbiome tests that let users “know what’s up down there.”
New York City-based Evvy ($129 for a single test or $99 each for four tests per year) uses metagenomic sequencing to identify the bacteria and fungi present in the vaginal microbiome. This information helps customers to understand their levels of protective and disruptive bacteria, which can be associated with everything from reoccurring infections and transmission of sexually transmitted diseases to infertility.
London-based Juno Bio ($149 per test) does not disclose its testing method. It does, however, provide users with a “full vaginal microbiome profile.” The profile is accessed online within a “few days” of returning the vaginal swab sample to the company’s clinical laboratory.
Both companies note that their tests are intended to be used for wellness purposes and are not meant to diagnose or treat disease or substitute for a physician’s consultation.
Gynecologist Oluwatosin Goje, MD, MSCR, FACOG, a reproductive infectious disease specialist at Cleveland Clinic, believes the availability of at-home vaginal microbiome testing will provide valuable information to both women and their doctors.
“It’s a powerful tool because it enables us to look at the entire microbial community through metagenomics and decipher how the overall composition might be affecting symptoms and infections, as well as determine the best treatment pathway,” Goje, an Evvy Medical Advisor, told Vogue. “Understanding the complete vaginal microbiome allows us to be good antibiotic stewards and only administer antibiotics when needed. Patients can also retest remotely to understand how antibiotics and other treatments impacted their vaginal microbiome.”
Evvy, which offers women an at-home vaginal microbiome test (above) that can provide insights into chronic vaginal infections and proclivity to contract sexually transmitted diseases and other women’s health issues, is one of several women-led diagnostic start-ups focused on women’s health. (Photo copyright: Evvy.)
Removing the Discomfort of Shopping for Women’s Health Products
Jamie Norwood and Cynthia Plotch, co-founders of Stix, a supplier of women’s health products and education, launched their company with a product line of at-home pregnancy and ovulation tests. They have since expanded their offerings to include urinary tract infection (UTI) and yeast infection testing and treatments.
“You can test, relieve, treat, and help prevent future infections—all from the comfort of your own home,” Norwood, told Vogue. She emphasized that this is the kind of experience healthcare consumers are demanding in today’s ever-growing direct-to-consumer clinical laboratory testing landscape. “Agonizing over confusing over-the-counter products in the drugstore aisles, or bending over backwards to pick up a prescription at the pharmacy, just isn’t cutting it for Millennial and Gen Z consumers.”
According to WebMD, yeast infections are a chronic problem for many women. While 75% of women will get at least one yeast infection in their lifetime, up to 8% get more than four a year. In addition, the federal Centers for Disease Control and Prevention (CDC) points out that bacterial vaginosis is the most common vaginal condition in females ages 15-44.
Lola Priego, is CEO and founder of blood test company Base, which sells at-home saliva and finger-prick blood tests to monitor hormone levels, vitamin levels, neurotransmitters, and blood cell markers to improve everything from sleep and diet to sex drive. She predicts direct-to-consumer testing will become as common as fitness watches.
“Eventually, at-home lab testing will be another readily-used tool, similar to your health-tracking wearables, that helps us optimize for a well-rounded healthy lifestyle in a more individualized way,” Priego told Vogue.
Femtech a ‘Significantly Underdeveloped’ Market
In its latest Analyst Note, financial data firm PitchBook maintained that the market for female health products is poised for growth. TechCrunch, which reviewed PitchBook’s analysis of female-focused health products, reported that Femtech remains a “significantly underdeveloped” slice of health-tech spending.
While women spend an estimated $500 billion annually on medical expenses, only 4% of research and development money is targeted at women’s health, PitchBook noted. In its analysis, Pitchbook predicted the global market for female-focused health products will reach $3 billion by the end of 2030. By comparison, that segment of the healthcare market totaled $820.6 million last year.
“While we still view Femtech as a niche industry, we believe secular drivers could help propel new growth opportunities in the space,” PitchBook analysts wrote. “These include the increasing representation of women in the venture-backed technology community, rising awareness and acceptance of women’s health issues, and the growing prevalence of infectious diseases among women in some countries in Africa and Asia.
“Furthermore, while the majority of Femtech products have traditionally focused on reproductive health, we believe new approaches to women’s health research will help open the door to new products and services,” they noted.
Clinical laboratory leaders will be wise to carefully watch the growth of at-home DTC tests and products targeted at female healthcare consumers since fewer trips to physicians’ offices may mean fewer test orders for local labs.
At the same time, the opportunity exists for innovative pathologists and lab managers to develop digital services that allow consumers who are self-testing to store their home-test results in the lab’s app. They can then receive relevant insights from clinical pathologists to help them fully understand the implications of the test results.
CDC advises clinical laboratories and microbiologists encountering C. auris to follow their own protocols before adopting federal agency guidelines
In July, the Centers for Disease Control and Prevention (CDC) warned healthcare facilities and clinical laboratories to be on the alert for Candida auris (C. auris) infections in their patients. An outbreak of the drug resistant and potentially deadly fungus had appeared in two Dallas hospitals and a Washington D.C. nursing home.
Since those outbreaks, researchers have studied with urgency the “superbug’s” emergence in various types of healthcare facilities around the nation, not just hospitals. Their goal was to discover how it was successfully identified and contained.
“Seeing what was happening in New York, New Jersey, and Illinois [was] pretty alarming for a lot of the health officials in California [who] know that LTACHs are high-risk facilities because they take care of [very] sick people. Some of those people are there for a very long time,” the study’s lead author Ellora Karmarkar, MD, MSc, told Medscape. Karmarkar is an infectious disease fellow with the University of Washington and formerly an epidemic intelligence service officer with the CDC.
“One of the challenges was that people were so focused on COVID that they forgot about the MDROs (multi-drug resistant organisms] … Some of the things that we recommend to help control Candida auris are also excellent practices for every other organism including COVID care,” she added.
According to Medscape, “The OCHD researchers screened LTACH and vSNF patients with composite cultures from the axilla-groin or nasal swabs. Screening was undertaken because 5%–10% of colonized patients later develop invasive infections, and 30%–60% die.
Medscape also reported that the first bloodstream infection was detected in May 2019, and that, according to the Annals of Internal Medicine study, as of January 1, 2020, of 182 patients:
22 (12%) died within 30 days of C. auris identification,
“This is really the first time we’ve seen clustering of resistance in which patients seemed to be getting the infections from each other,” Meghan Lyman, MD, Medical Officer in the Mycotic Diseases Branch of the CDC, told Fox News.
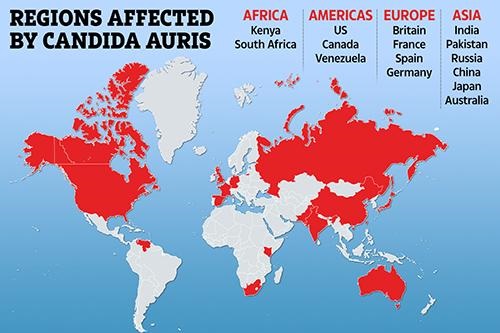
The graphic above illustrates how Candida auris is “spanning the globe,” The New York Times reported. Clinical laboratories that encounter this potentially deadly fungus are advised to contact the CDC immediately for guidance and to take proactive steps to prepare for the “superbug’s” arrival. (Graphic copyright: The Scottish Sun.)
Be More Proactive than Reactive in Identifying C. Auris, CDC Says
C. auris is a type of yeast infection that can enter the bloodstream, spread throughout the body, and cause serious complications. People who appear to have the highest risk of contracting the infection are those:
Who have had a lengthy stay in a healthcare facility,
Individuals connected to a central venous catheter or other medical tubes, such as breathing or feeding tubes, or
Have previously received antibiotics or antifungal medications.
It tends to be resistant to the antifungal drugs that are commonly used to treat Candida infections.
It can be difficult to identify via standard laboratory testing and is easily misidentified in labs without specific technology.
It can quickly lead to outbreaks in healthcare settings.
“With all this spread that we’ve been seeing across the country we’re really encouraging health departments and facilities to be more proactive instead of reactive to identifying Candida auris in general,” Lyman told STAT. “Because we’ve found that controlling the situation and containing spread is really easiest when it’s identified early before there’s widespread transmission.”
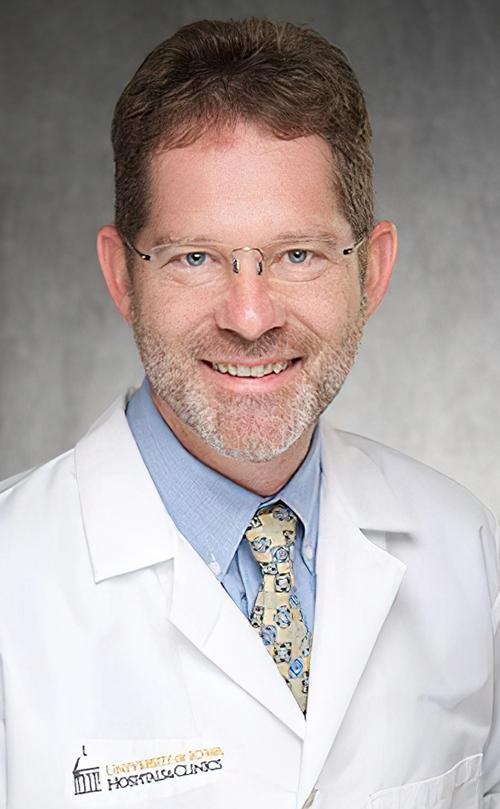
There continues to be concerns over this highly drug-resistant infection among hospital physicians and medical laboratories. “Acute care hospitals really ought to be moving toward doing species identification of Candida from nonsterile sites if they really want to have a better chance of detecting this early,” Dan Diekema, MD (above), an epidemiologist and clinical microbiologist at the University of Iowa, told Medscape. (Photo copyright: University of Iowa.)
Candia Auris versus Other Candida Infections
C. auris can cause dangerous infections in the bloodstream and spread to the central nervous system, kidneys, liver, spleen, bones, muscles, and joints. It spreads mostly in long-term healthcare facilities among patients with other medical conditions.
The symptoms of having a Candida auris infection include:
Fever
Chills
Pain
Redness and swelling
Fluid drainage (if an incision or wound is present)
General feeling of tiredness and malaise
C. auris infections are typically diagnosed via cultures of blood or other bodily fluids, but they are difficult to distinguish from more common types of Candida infections, and special clinical laboratory tests are needed to definitively diagnose C. auris.
Whole-genome Sequencing of C. Auris and Drug Resistance
The CDC conducted whole-genome sequencing of C. auris specimens gathered in Asia, Africa, and South America and discovered four different strains of the potentially life-threatening Candida species. All four detected strains have been found in the United States.
There are only three classes of antifungal drugs used to treat Candida auris infections:
However, 85% of the infections in the US have proven to be resistant to azoles and 38% are resistant to polyenes. Patients respond well to echinocandins, but more effective therapies are needed especially as some isolates may become resistant while a patient is on drug therapy, STAT reported.
“Even while it might be susceptible upfront, after a week or two of therapy, we may find that the patient has an infection now caused by an isolate of the same Candida auris that has become resistant to the echinocandins and we are really left with nothing else,” Jeffrey Rybak, PhD, PharmD, Instructor, Department of Pharmaceutical Sciences, St. Jude Children’s Research Hospital, told Infection Control Today.
Although relatively rare, C. auris infections are on the rise. The good news is that there may be further pharmaceutical help available soon. New antifungal agents, such as Ibrexafungerp (Brexafemme) show promise in fighting C. auris infections, but more research is needed to prove their efficacy.
What Should Clinical Laboratories Do?
The CDC stresses that clinical laboratories and microbiologists working with known or suspected cases of Candida auris should first adhere to their own safety procedures. The CDC issued guidelines, but they are not meant to supersede the policies of individual labs.
The CDC also recommends that healthcare facilities and clinical laboratories that suspect they have a patient with a Candida auris infection immediately contact the CDC and state or local public health authorities for guidance.