Microbiologists will want to take note of the CDC’s statement that the illness can masquerade as other diseases
It is the latest example of a bacterium uncommon in the United States that has infected patients in this country—one of whom has died. The three infected patients live in separate states, but genetic analysis indicates their cases may be related.
According to the health alert, “Based on genomic analysis, these three cases (one male, two females; two adults and one child) may share a potential common source of exposure. The first case, identified in March 2021, was fatal. Two other patients were identified in May 2021, one of whom is still hospitalized. One has been discharged to a transitional care unit. None of the patients’ families reported a history of traveling outside of the continental United States.”
The CDC warned, “Symptoms of melioidosis are varied and nonspecific and may include pneumonia, abscess formation, and/or blood infections. Due to its nonspecific symptoms, melioidosis can initially be mistaken for other diseases such as tuberculosis, and proper treatment may be delayed.”
Microbiology Laboratories Should Be on Alert
Melioidosis is typically only seen in subtropical and tropical regions and can be highly fatal. It is unknown how the trio of patients who contracted the illness became infected, but according to the CDC the cases do appear to be connected.
“Testing suggests a common source of infection, but that source has not yet been identified,” a CDC representative told Gizmodo. “CDC is working with states to assess exposures or products these individuals have in common, as well as environmental samples from the states where cases have been identified. Additionally, CDC experts are providing epidemiologic assistance to help investigate the cause of infection,” the CDC added.
“Melioidosis is a serious neglected tropical disease of Southeast Asia, India, and Australia where it is a major cause of pneumonia, abscesses, and sepsis. The fact that it may be gaining a foothold in the US is concerning,” pediatrician Peter Hotez, MD, PhD (above), Dean of the National School of Tropical Medicine, Professor of Pediatrics and Molecular Virology and Microbiology at Baylor College of Medicine, and Director of the Center for Vaccine Development at Texas Children’s Hospital, told Gizmodo. Clinical laboratories and microbiologists will want to monitor these cases for future developments. (Photo copyright: Baylor College of Medicine.)
Melioidosis, also called Whitmore’s disease, was first described by Alfred Whitmore, an English pathologist, in 1912 in what is now present-day Myanmar. The bacterium (Burkholderia pseudomallei) can be found in contaminated soil and water. It is predominately found in tropical climates in Southeast Asia and northern Australia and can affect humans and many species of animals.
Researchers believe the disease may be acquired through the inhalation of contaminated dust particles or water droplets, the ingestion of contaminated water or soil-contaminated food, or other contact with tainted soil, especially through skin abrasions. It is very rare to contract melioidosis from infected individuals.
Melioidosis Masquerades as Other Illnesses
The symptoms of melioidosis are wide-ranging and non-specific and can resemble those of other illnesses. In addition, there are several types of the illness, and they can each act differently depending on where the infection is in the body. The most common symptoms of melioidosis include:
Localized Infection:
Localized pain or swelling
Fever
Ulceration
Abscess
Pulmonary Infection:
Cough
Chest pain
High fever
Headache
Anorexia
Bloodstream Infection:
Fever
Headache
Respiratory distress
Abdominal discomfort
Joint pain
Disorientation
Disseminated Infection:
Fever
Weight loss
Stomach or chest pain
Muscle or joint pain
Headache
Central nervous system/brain infection
Seizures
According to the CDC, the time between an exposure to Burkholderia pseudomallei and the first emergence of Melioidosis symptoms is not clearly defined but could range from one day to many years. However, most infected individuals begin experiencing symptoms of melioidosis within two to four weeks after exposure.
Melioidosis is difficult to diagnose, and some automated bacterial reading instruments can mistake Burkholderia pseudomallei for other bacteria. It is estimated that the disease accounts for 89,000 deaths per year worldwide. Delays in diagnosis and treatment often lead to poor patient outcomes and the mortality rate can exceed 40% in some regions, Nature reported.
The illness is typically treated with appropriate drug therapies including intravenous antimicrobial medications, such as Ceftazidime or Meropenem, followed by an oral antimicrobial therapy such as Trimethoprim-sulfamethoxazole or Amoxicillin/Clavulanic Acid. It may take several months for a patient to be cured of melioidosis, depending on the extent of the infection.
Deadly Bacterium’s Countries of Origin and Spread to the US
According to CDC data, the greatest number of melioidosis cases are reported in Thailand, Malaysia, Singapore, and northern Australia. Cases also have been reported in other Asian countries as well as Mexico and Central America.
Burkholderia pseudomallei does not occur naturally in the US, and cases of melioidosis identified in the US are usually only seen in world travelers and immigrants who come from countries where the disease is widespread. The bacterium has been found in soil in Mexico, so it is possible that it could spread to parts of the US, which has led to concern among microbiologists.
“Due to changes in weather patterns, some pathogens that normally were not present in a particular area might start causing disease,” Alfredo Torres, PhD, Associate Provost, Department of Microbiology and Immunology, University of Texas Medical Branch, told Gizmodo. “Therefore, it is important to make the health professionals aware of this pathogen and the disease that it causes, so quick identification can be done, and treatment is properly used to save lives. Without that, it might be too late for the next melioidosis patient when the proper diagnosis is done.”
The CDC has suggested that healthcare workers consider melioidosis as a possible diagnosis for patients who have compatible symptoms, even if they have not recently traveled outside of the US.
CDC Suggests Rerunning Certain Clinical Laboratory Tests
Because Burkholderia pseudomallei can be mistaken for other bacteria, the CDC also urges the rerunning of clinical laboratory tests using automated identification, especially if another bacterium that is often mistaken for Burkholderia pseudomallei is present, Gizmodo noted.
“CDC encourages healthcare workers to be aware of the potential for more cases and to report cases to their state health departments,” the CDC stated.
The CDC considers the risk of melioidosis to the public in the US to be low, and that the chances of a potential outbreak are unlikely. However, the origins of these three cases remain a mystery and warrant further investigation.
Microbiologists and clinical laboratories should be aware of and remain alert about this potentially fatal illness. It is possible that more cases will arise in the future, especially in the three states where it has already been found.
Following a nearly two-year disruption due to the SARS-CoV-2 pandemic, pathologists and clinical laboratory professionals once again have an opportunity to gather and learn from each other
It is good news that the daily number of new cases of COVID-19 continue declining here in the United States. That fact, and the growing number of vaccinations, have encouraged state and federal officials to lift many restrictions on business and social activities.
Clinical laboratories are watching a big drop in the daily number of COVID-19 tests they perform, even as routine test volumes climb and more patients show up in doctors’ offices for the typical mix of ailments and health conditions.
It’s true that many familiar routines are back. But it is also true that things are not exactly the way they were pre-pandemic. And that’s the rub. Going forward, what should medical laboratory managers and pathologists expect to be the “post-pandemic normal” in how patients access care and how providers deliver clinical services? How will healthcare in this country be different from what it was pre-pandemic?
Preparing Clinical Lab Leaders for What Comes Next
These questions and more will be front and center when the Executive War College on Lab and Pathology Management returns on Nov. 2-3, 2021, at the Hyatt Riverwalk Hotel in San Antonio. The theme of this first live gathering since the spring of 2019 will be “Preparing Your Clinical Laboratory and Pathology Group for Post-Pandemic Success.”
“Today, lab managers have the interesting challenge of understanding the new opportunities they can use to advance their labs, both clinically and financially,” stated Robert L. Michel, Editor-in-Chief of Dark Daily and its sister publication The Dark Report, and founder of the Executive War College. “It isn’t that the pandemic changed healthcare in fundamental ways. Rather, it is that the pandemic accelerated changes that were underway before the outbreak began.
“That’s true of telehealth as well, for example,” he continued. “Once the nation was locked down, utilization of virtual physician visits and telehealth services skyrocketed. Today, national surveys confirm that as many as 50% of all patients and physicians have used a telehealth service, are comfortable with this type of appointment, and are ready to continue to use virtual office visits.
Robert Michel (above), Editor-in-Chief of Dark Daily, its sister publication The Dark Report, and founder of The Dark Intelligence Group, will host the first live edition of the Executive War College since May 2019 in San Antonio. The theme will be “Preparing Your Clinical Laboratory and Pathology Group for Post-Pandemic Success.” Attendees from clinical laboratories and pathology groups will gain critical insights they can act on immediately. (Photo copyright: The Dark Report.)
“Another trend accelerated by the pandemic is patient self-testing at home,” Michel added. “Government health officials saw the benefit of clearing for clinical use different specimen collection systems and COVID-19 test methods designed for use by consumers in the comfort of their home. Today, consumers can choose from multiple specimen collection products and SARS-CoV-2 tests designed for in-home use. Clinical laboratory managers should consider this development to be a consumer home-test baseline. Federal officials have created a regulatory pathway that will make it easier and faster for federal regulators to clear other types of diagnostic tests for consumer home use.”
What if the FDA Approves More Consumer At-Home Tests?
There are implications to each of the two trends described above. In the case of telehealth, if patients see their doctors virtually and the doctors order medical tests, how do clinical laboratories access these patients to collect the specimens needed to do this testing?
Similarly, if, in coming years, the federal Food and Drug Administration (FDA) increases the number of diagnostic test specimen-collection kits that consumers can use from home, how should local clinical laboratories position themselves to receive those kits and perform those tests?
These are two examples of important questions to be answered at sessions scheduled for the Executive War College in San Antonio on Nov. 2-3. Case studies by innovative lab leaders will address topics ranging from high-level strategy to daily management, operations, marketing, and managed care contracting.
Attendance Limited at This Fall’s Executive War College
At the first live edition of the Executive War College since May 2019, attendees will notice one significant difference from earlier years. By design, and for the safety and well-being of attendees, the number of attendees will be limited to 300. The hotel follows the Centers for Disease Control and Prevention (CDC) guidelines and is prepared to adjust those numbers as CDC guidance evolves. Thus, those interested in attending this year’s conference are advised to register early to guarantee their place and avoid being disappointed.
Suggestions for session topics and speakers are welcome and can be sent to info@darkreport.com. Conference details, session topics, and speakers will be updated regularly at www.executivewarcollege.com.
So, register today because seating is limited at the 2021 Executive War College Presents “Preparing Your Clinical Laboratory and Pathology Group for Post-Pandemic Success.” To ensure your place at this valuable conference, click HERE or place this URL (https://dark.regfox.com/2021-ewc-presents) into your browser.
This is yet another example that dogs can be highly accurate screeners for disease. But are they ready to be included in clinical laboratory diagnostic tests?
Thailand researchers have trained dogs to screen for COVID-19 infections in humans, despite the country’s “spicy and flavorful cuisine,” the AP reported. This is just the latest example of a country using dogs to identify individuals who are infected with the SARS-CoV-2 coronavirus. Clinical laboratory managers and pathologists have seen other examples of dogs being trained to identify different diseases or health conditions.
In fact, dogs have been shown to be highly accurate at spotting disease in humans and the practice is becoming common worldwide. But could dogs achieve the required clinical accuracy and reproducibility in detecting disease for the procedure to be translated into clinical practice?
Smelling Disease as a Clinical Laboratory Diagnostic
Clinical laboratory professionals are quite familiar with the concept of the human body producing volatile chemicals that can serve as biomarkers for disease or illness. Dark Daily has previously reported on multiple breath/aroma-based diagnostic clinical laboratory tests going as far back as 2013.
But it is in the use of dogs to spot COVID-19 infections in humans where this type of breath/aroma-based diagnostic test research is making a notable impact.
“Even if this approach were not warranted as a clinical diagnostic procedure, trained dogs could be deployed at airports, train stations, sporting events, concerts, and other public places to identify individuals who may be positive for SARS-CoV-2, the coronavirus that causes the COVID-19 illness,” we wrote. “Such an approach would make it feasible to ‘screen’ large numbers of people as they are on the move. Those individuals could then undergo a more precise medical laboratory test as confirmation of infections.”
According to the researchers, individuals with a COVID-19 infection emit a unique odor that is present in sweat samples. The six Labrador retrievers used in the research were able to detect the presence of COVID-19 with an impressive 95% accuracy rate in more than 1,000 samples presented to them, the AP reported.
A Labrador Retriever named Bobby (above) sniffs sample of human sweat through containers to detect COVID-19 coronavirus at Veterinary Faculty, Chulalongkorn University in Bangkok. Thailand has deployed a canine virus detection squad to help provide a fast and effective way of identifying people with COVID-19 as the country faces a surge in cases, with clusters found in several crowded slum communities and large markets. Clinical laboratory professionals and pathologists will find it interesting that the dogs are given a sample of sweat, each presented in a unique container. Thus, the dogs never are in the presence of the humans who provided the specimens. (Photo and caption copyright: AP/Sakchai Lalit)
To perform the study, the scientists placed sweat samples in metal containers and allowed the dogs to sniff each sample. If no trace of the infection was present, the dogs simply walked past the container. If the disease was detected in a particular sample, the dogs would sit down in front of the container.
Would Spicy Food Interfere with Dogs’ Ability to Detect COVID-19?
The head of the research team, Professor Kaywalee Chatdarong, PhD, noted that other countries also have been using canines to detect the presence of COVID-19. She did have some concerns that the utilization of dogs for this purpose may not work in Thailand due to their often-spicy cuisine. However, since the samples used were from students and faculty at the university, as well as people from the surrounding area, the cuisine did not seem to affect the study results, the AP reported.
Thailand is facing a surge in COVID-19 cases with recent clusters reported at construction sites, crowded neighborhoods, and large markets. The research team plans to use the canines in mobile units in communities suspected of being hotspots for the disease.
A major plus of using dogs to sniff out the disease from sweat samples is the ability to test people who may not be able to get out of their homes to be tested.
“People can simply put cotton balls underneath their armpits to collect sweat samples and send them to the lab,” Suwanna Thanaboonsombat, a volunteer who collects samples and brings them to the clinical laboratory for testing, told the AP. “And the result is quite accurate.”
According to the US Centers for Disease Control and Prevention (CDC), dogs can become infected with the SARS-CoV-2 coronavirus. However, their chances of transmitting the disease to humans is extremely low. Nevertheless, to ensure the dogs do not become infected with COVID-19 themselves, the researchers designed the sample containers to avoid contact between the samples and the dogs’ noses.
Living Animals Come with Limitations
While dogs can provide a quick and inexpensive method of testing for COVID-19, they do have limitations.
“5 p.m. is their dinner time. When it’s around 4:50, they will start to be distracted. So, you can’t really have them work anymore,” Chatdarong told the AP. “And we can’t have them working after dinner either because they need a nap. They are living animals and we do have to take their needs and emotions into consideration. But for me, they are heroes and heroines.”
Using Dogs to Detect COVID-19 in Other Countries
Last fall, the Helsinki Airport in Finland announced it would use a team of trained dogs to detect the presence of COVID-19 among visitors to the airport to ensure the health and safety of its customers and their families, and to help prevent the spread of SARS-CoV-2 in Finland.
Being tested for the coronavirus at the Helsinki airport in Finland does not require direct contact with a dog. Individuals simply need to swipe their skin with a test wipe and drop the wipe into a cup. The cup is then given to a dog that is working in a separate booth (shown above), which protects both the dog and the dog’s handler from contamination. All tests are processed anonymously and anyone testing positive for COVID-19 is directed to a health information point located at the airport. (Photo copyright: Finavia.)
“We are among the pioneers. As far as we know no other airport has attempted to use canine scent detection on such a large scale against COVID-19,” said Airport Director Ulla Lettijeff in a Finavia press release. “This might be an additional step forward on the way to beating COVID-19.”
In addition to being “man’s best friend,” dogs serve valuable purposes in the medical community. Their strong sense of smell may render them useful in the detection of and fight against illnesses, including COVID-19.
Whether the performance and accuracy of individual dogs can be validated with acceptable quality control (QC) procedures remains to be seen. Medical laboratory managers and pathologists understand the challenges presented with demonstrating accuracy and reproducibility with this method of diagnostic testing. That obstacle has prevented research outcomes from being translated into clinical practice.
Legal, regulatory, and payer experts outline steps that help medical laboratories better navigate federal and state regulatory guidelines, eliminate coding and billing missteps, and maximize reimbursements
Even as daily COVID-19 test numbers continue to decrease, many clinical laboratories have substantial numbers of COVID-19 test claims that remain unpaid. Despite federal and state law requiring that labs be paid for these tests, commercial health plans are using many strategies to avoid paying labs for COVID-19 test claims.
That means a large portion of the nation’s labs are owed tens of thousands, hundreds of thousands, even millions of dollars for unpaid SARS-CoV-2 test claims they submitted since the onset of the pandemic last year.
What Clinical Labs Can Do to Be Paid for Their COVID-19 Test Claims
These four subject-matter experts provided insider tips and insights on steps clinical laboratories can take to get paid for COVID-19 test claims. This advice can help labs, maximize collected dollars, reduce the chance of post-payment audits, and navigate emerging payer trends.
During the webinar, Caitlin Forsyth, an Associate Attorney at Davis Wright Tremaine LLP in Seattle who specializes in healthcare regulatory compliance, said the new guidance “impressed upon commercial health plans the requirement to cover COVID testing in a lot of different circumstances.” The guidance included information on how providers can be reimbursed for providing COVID-19 care to uninsured people.
However, labs should be aware of what may come after they receive payment.
“We applaud you if you’ve had success thus far in securing reimbursement,” Forsyth continued. “However, clinical laboratories are not necessarily home free if Medicare, Medicaid, or a health plan has paid all or most of the lab claims for COVID-19 tests. This is because the payer may at some point down the line require the laboratory to submit to a post-payment audit. As part of the audit, the government payer or health plan is likely to require a laboratory to provide supporting documentation underscoring the medical necessity of each test performed on each patient at issue.”
What Constitutes ‘Medical Necessity’ for a SARS-CoV-2 Test?
There are many tripwires that can derail COVID-19 test claims. Medical necessity standards related to testing is one example that has been a major area of concern for clinical laboratories.
Kathryn Edgerton, Esq., Counsel at Davis Wright Tremaine LLP in Los Angeles, notes that the guidance providers have received has been “somewhat inconsistent and has created confusion as to what test is covered.” This lack of clarity in Medicare’s guidance has caused many denials of payment.
This Special Report from Dark Daily is the companion to the recent Dark Daily webinar on “Getting Paid for COVID-19 Test Claims: Prepare for Audits, Maximize Reimbursement and Navigate Payer Trends.” Clinical laboratory professionals can download the report by clicking here. (Photo copyright: Dark Daily.)
The webinar panelists provided the following three tips for optimizing billing claims for COVID-19 tests (additional recommendations on decreasing the number of COVID-19 test claim denials, increasing payments, and avoiding post-payment audits are available in the webinar’s on-demand replay and its companion special report):
When seeking reimbursement for COVID-19 testing from non-traditional sources, such as employers, schools, or local governments, ensure valid orders support each test claim. “Even if the employer, school, or local government has agreed to pay for the tests, a medical laboratory still must comply with state laws in regard to persons authorized to order the tests, as well as comply with CLIA requirements for a valid order,” Forsyth said.
Serial testing is on the rise in workplaces to increase the chances of detecting asymptomatic infection. However, Forsyth says, laboratories should “push for direct reimbursement from the workplace” because coverage from Medicare, Medicaid, and health plans is uncertain. “We also expect health plans to start cracking down on tests performed as part of an employment or surveillance program, taking the position that even if there are physician orders supporting each test performed as part of the program, health plans are not required to cover tests,” she added.
COVID-19-only testing providers and independent laboratories should expect health plans to begin narrowing their provider networks. To avoid being pushed out, Steve Stonecypher, Managing Partner at Shipwright Healthcare Group, says laboratories should “think about what you do, how you do it, and how you can be a benefit [to the health plan]. Make the payers think of you not as a nice-to-have in their network, but as a need-to-have in their network.”
COVID-19 Testing Labs Advised to ‘Have All Your Ducks in a Row’
Stonecypher urges clinical laboratories to be vigilant in record keeping, noting that the US Department of Health and Human Services Office of Inspector General (OIG) indicated earlier this year that it will conduct audits that focus on aberrant billing for COVID-19 testing during the pandemic.
“There are flags out there already that the OIG is potentially going to look to do claim audits,” he said. “You can pretty much guarantee that the payers are going to follow. So, have all your ducks in a row. We’re talking about all the individual patient assessments, all that necessary documentation … make sure all of that is in order because payers are going to look at this as an opportunity to come back and recoup money.”
Billing and finance executives, clinical laboratory leadership, compliance officers, and billing and coding administrators are especially encouraged to listen to this webinar about increasing the number of COVID-19 test claims for which the lab is reimbursed. This webinar is available to stream on-demand.
This can be one of the best low-cost, high return investments your lab team can make, particularly if it helps the lab’s coding/billing/collections team interact with health insurance plans to settle SARS-CoV-2 test claims that then bring in tens of thousands or hundreds of thousands of dollars from outstanding claims that have yet to be paid.
Clinical laboratories may see increase in flu and COVID-19 specimen processing as people return to pre-pandemic social behaviors, experts predict
While SARS-CoV-2 infections continue to ravage many parts of the world, influenza (flu) cases in North America have hit a historic low. As winter approached last year, infectious disease experts warned of a “twindemic” in which the COVID-19 outbreak would combine with seasonal influenza to overwhelm the healthcare system. But this did not happen, and many doctors and medical laboratory scientists are now investigating this unexpected, but welcomed, side-effect of the pandemic.
From the start of the current flu season in September 2020, clinical laboratories in the US reported that 1,766 specimens tested positive for flu out of 931,726—just 0.2%—according to the CDC’s Weekly US Influenza Surveillance Report. That compares with about 250,000 positive specimens out of 1.5 million tested in the 2019-2020 flu season, the CDC reported. Public health laboratories reported 243 positive specimens out of 438,098 tested.
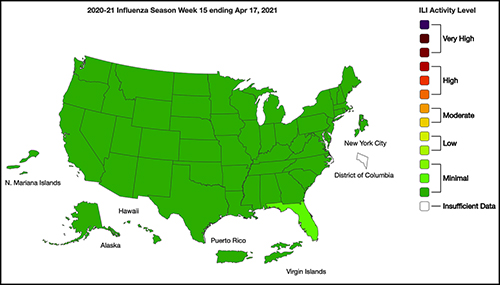
The graphic above taken from the CDC’s Weekly Influenza Surveillance Report for the week ending April 17, 2021, illustrates how “Nationwide during week 15, 1.1% of patient visits reported through ILINet were due to ILI [Influenza-like Illness].” This percentage, according to the CDC, is below the national baseline of 2.6%. “Seasonal influenza activity in the United States remains lower than usual for this time of year.” (Graphic copyright: Federal Centers for Disease Control and Prevention.)
Fear of COVID-19 Linked to Fewer Flu Deaths in Children
WebMD reported that just one child in the US has died from the flu this year, compared with 195 in 2020. Why the low numbers?
Precautions people take to avoid COVID-19 transmission, including masking, social distancing, and handwashing.
Reduced human mobility, including less international travel.
Higher-than-usual flu vaccination rates. As of February 26, the CDC reported that nearly 194 million doses of flu vaccine had been distributed in the US.
WebMD noted this could be a record, but that the CDC data doesn’t indicate how many doses were actually administered.
However, Schaffner told WebMD that efforts to keep kids home from school and away from social gatherings were likely a bigger factor. “Children are the great distributors of the influenza virus in our society,” he said. But due to fears about COVID-19 transmission, kids “weren’t even playing together, because mothers were keeping them off the playground and not having play dates.”
Repercussions for Fighting Flu Next Year
Public health experts welcomed the low flu levels, however, Politico reported that limited data about flu circulation this year could hamper efforts to develop an effective vaccine for next season’s flu strains.
Each February, Politico explained, experts convened by the World Health Organization (WHO) look at data from the current and previous flu seasons to predict which strains are likely to predominate in the Northern Hemisphere next winter. That includes data about which strains are currently circulating in the Southern Hemisphere. The WHO uses these predictions to recommend the composition of flu vaccines. In the US, the final decision is made by an FDA advisory committee.
A similar WHO meeting in September guides vaccine development in the Southern Hemisphere.
The WHO issued this year’s Northern Hemisphere recommendations on Feb. 26. The advisory includes recommendations for egg-based and cell- or recombinant-based vaccines, and for quadrivalent (four-strain) or trivalent (three-strain) vaccines.
In a document accompanying the recommendations, the WHO acknowledged concerns about this year’s limited pool of data.
“The volume of data available from recently circulating influenza viruses, and the geographic representation, have been significantly lower for this northern hemisphere vaccine recommendation meeting than is typical,” the document stated. “The reduced number of viruses available for characterization raises uncertainties regarding the full extent of the genetic and antigenic diversity of circulating influenza viruses and those likely to pose a threat in forthcoming seasons.”
The report notes that experts identified changes in circulating Influenza A(H3N2) viruses this year, and that the changes are reflected in the new vaccine recommendation.
But Paul A. Offit, MD, who serves on the FDA’s vaccine advisory panel, downplayed worries about the vaccine. “The belief is that there was enough circulating virus to be able to pick what is likely to be the strains that are associated with next year’s flu outbreak,” he told Politico. Offit is a Professor of Vaccinology and Pediatrics at the Perelman School of Medicine at the University of Pennsylvania and Director of the Vaccine Education Center at the Children’s Hospital of Philadelphia.
Pediatrician and internationally recognized expert in the fields of virology and immunology, Paul A. Offit, MD (above), told Politico that the low level of flu circulation this year, along with the resulting uncertainty, “is unprecedented.” Clinical laboratories might not have noticed the severe decrease in influenza specimens sent for processing due to being hyper-focused on COVID-19 testing. But as the pandemic subsides, loss of flu testing revenues will likely become more apparent. (Photo copyright: University of Pennsylvania.)
Offit suggests that efforts to mitigate the COVID-19 outbreak could be useful to combat other infectious disease outbreaks. However, both Offit and Gostin expressed doubt about that prospect.
“I mean, could we reasonably in a winter month, wear masks just at least when we’re outside in large crowds? … Or are we comfortable having hundreds of 1000s of cases of hospitalizations for flu and 10s of 1000s [of] deaths? I suspect the answer is B. We’re comfortable with that, we’re willing to have that even though we just learned, there’s a way to prevent it,” Offit told Politico.
“Remember after the 1918 flu pandemic, most people don’t realize what happened when that was over. But what happened was the roaring ‘20s,” Gostin told Politico. “People started congregating, mingling, hugging, kissing. All the things they missed. They crowded into theaters and stadiums and went back to church. That’s what’s likely to happen this fall and that makes the influenza virus very happy.”
So, what should clinical laboratories expect in future flu and COVID-19 vaccines? That is not yet clear. One thing is certain, though. New lab test panels that test for influenza and the SARS-CoV-2 coronavirus will be arriving in the marketplace.