Royal College of Pathologists of Australia says the pandemic is ‘suppressed’ to ‘intermittent’ outbreaks, thanks to the dedication of thousands of pathologists, medical scientists, and laboratory professionals
COVID-19 efforts in Australia have achieved a milestone. Pathology laboratories there have performed more than 12 million SARS-CoV-2 tests since the pandemic began. That is an impressive feat and is equal to about half the country’s population of 25.4 million people.
“It is an incredible feat,” they continued. “Australia’s current position of having effectively suppressed the virus to intermittent outbreaks owes much to the year-long dedication and ingenuity of 35,000 pathologists, medical scientists, lab technicians, couriers, phlebotomists, and ancillary personnel.”
Australia Pathology Society Recognizes Accomplishments
Furthermore, Graves and Bott wrote, pathology in Australia deserves recognition for these pandemic-related accomplishments, among others, as well:
Australia launched drive-through COVID-19 testing clinics even before the pandemic was declared by the World Health Organization (WHO).
An RCPA quality assurance program for lab COVID-19 testing was the first of its kind to start worldwide, and it became a model for other countries.
Australia’s pathology labs were fast to develop in-house test kits once they had the genome sequence for the SARS-CoV-2 coronavirus.
Quick Responses to COVID-19 in the Land Down Under
The Doherty Institute (a joint venture of the University of Melbourne and the Royal Melbourne Hospital) offers research, teaching, public health and reference lab services, diagnostics, and clinical care for infectious diseases and immunity.
After receiving the patient sample on Jan. 24, 2020, institute scientists were the first outside China to grow the coronavirus in cell culture, noted a University of Melbourne news release.
“We’ve planned for an incident like this for many, many years, and that’s really why we were able to get an answer so quickly,” Dr. Mike Catton (above), Co-Deputy Director, Doherty Institute and Director of the Victorian Infectious Diseases Reference Laboratory (VIDRL), said in the news release. (Photo copyright: ABC News.)
Doherty Institute researchers also were first to report on immune response to COVID-19, according to a second news release.
“When COVID-19 emerged, we already had ethics and protocols in place so we could rapidly start looking at the virus and immune system in great deal,” Dr. Irani Thevarajan, Infectious Disease Physician, Doherty Institute, Royal Melbourne Hospital, said in the second news release.
“Our study provides novel contributions to the understanding and kinetics of immune responses during a non-severe case of COVID-19. This patient did not experience complications of respiratory failure or acute respiratory distress syndrome, did not require supplemental oxygenation, and was discharged within a week of hospitalization, consistent with non-severe but symptomatic disease,” Thevarajan and co-authors wrote in Nature Medicine.
Drive-Through COVID-19 Testing Sites in Australia
Also impressive was Australia’s launch of drive-through COVID-19 testing on March 9, 2020, before the pandemic was declared by WHO on March 11.
The COVID-19 testing site in Adelaide, South Australia, was “believed to be a first for the country’s public health system,” ABC News reported.
Public Recognition for Medical Laboratories has Global Reach
The COVID-19 response and scientific contributions by pathology laboratory scientists and researchers in Australia are noteworthy. It is also significant that Australia’s pathology professional society sought recognition for medical laboratory workers by detailing their accomplishments during the pandemic and sharing them in media with national and global reach.
CAP president maintains medical laboratory staff are ‘indispensable’ in pandemic fight and should be in ‘top tier’ for vaccination
As COVID-19 vaccinations continue to roll out, the College of American Pathologists (CAP) is lobbying for clinical pathologists and medical laboratory staff to be moved up the priority list for vaccinations, stating they are “indispensable” in the pandemic fight.
In a news release, CAP’s President Patrick Godbey, MD, FCAP argued for the early vaccination of laboratory workers, “It is essential that early access to the vaccine be provided to all pathologists and laboratory personnel,” he said. “Pathologists have led throughout this pandemic by bringing tests for the coronavirus online in communities across the country and we must ensure that patient access to testing continues. We must also serve as a resource to discuss the facts about the vaccine and answer questions patients, family members, and friends have about why they should get the vaccine when it is available to them.”
In a phone call following a virtual press conference, pathologists and CAP President Patrick Godbey, MD (above), told MedPage Today that even if medical laboratory staff are not directly in contact with patients, they should be considered “top tier” (designated as Phase 1a) for getting the vaccine. “I think they [clinical laboratory workers] should be considered in the same tier as nurses,” said Godbey, who also is Laboratory Director at Southeastern Pathology Associates and Southeast Georgia Health System in Brunswick, Ga. “They’re indispensable. Without them, there’d be no one to run the tests.” (Photo copyright: Southeast Georgia Health System.)
Who Does CDC Think Should Be First to Be Vaccinated?
According toThe New York Times (NYT), there are an estimated 21 million healthcare workers in the United States, making it basically “impossible,” the NYT wrote, for them all to get vaccinated in the first wave of COVID-19 vaccinations.
A December 11, 2020, CDC Morbidity and Mortality Weekly Report, titled, “ACIP Interim Recommendation for Allocating Initial Supplies of COVID-19 Vaccine—United States, 2020,” notes that “The [federal] Advisory Committee on Immunization Practices (ACIP) recommended, as interim guidance, that both 1) healthcare personnel and 2) residents of long-term care facilities be offered COVID-19 vaccine in the initial phase of the vaccination program.”
The ACIP report defines healthcare personnel as “paid and unpaid persons serving in healthcare settings who have the potential for direct or indirect exposure to patients or infectious materials.”
However, a CDC terminology guidance document listed at the bottom of the ACIP report states, “For this update, HCP [Healthcare Personnel] does not include dental healthcare personnel, autopsy personnel, and laboratory personnel, as recommendations to address occupational infection prevention and control (IPC) services for these personnel are posted elsewhere.”
In part, the letter stated, “We are convinced that ACIP did not intend to exclude any healthcare workers from its recommendation to offer vaccinations to healthcare personnel in the initial phase of the COVID-19 vaccination program (Phase 1a). However, we would hate for jurisdictions to overlook dental, autopsy, and laboratory personnel because of a minor footnote in [CDC] guidance that was developed for an entirely different purpose (i.e., infection control).
“We respectfully ask CDC to clarify,” the letter continues, “… that all healthcare workers—including dental, autopsy, and laboratory personnel—are among those who should be given priority access to vaccine during the initial phase of the COVID-19 vaccination program.”
“In the laboratory, they are encountering and handling thousands of samples that have active live virus in them,” said Karger, who called clinical laboratory staff and phlebotomists the “forgotten” frontline healthcare workers. “We’re getting 10,000 samples a day. That’s a lot of handling of infectious specimens, and we do want [staff] to be prioritized for vaccination.”
Karger continued to stress the vital role clinical laboratories play not only in COVID-19 testing but also in the functioning of the overall health system. She added that staff burnout is a concern since laboratory staff have been working “full throttle” since March.
“From an operational standpoint, we do need to keep our lab up and running,” she said. “We don’t want to have staff out such that we would have to decrease our testing capacity, which would have widespread impacts for our health system and state.”
Testing for Post-Vaccine Immunity
The CAP panelists also highlighted the need to prepare for the aftermath of widespread COVID-19 vaccinations—the need to test for post-vaccine immunity.
“It’s not routine practice to check antibody levels after getting a vaccine but given the heightened interest in COVID testing, we are anticipating there is going to be some increased in demand for post-vaccine antibody testing,” Karger said. “We’re at least preparing for that and preparing to educate our providers.”
Karger pointed out that clinical pathologists will play an important role in educating providers about the type of antibody tests necessary to test for COVID-19 immunity, because, she says, only the SARS-CoV-2 spike protein antibody test will check for an immune response.
With the pandemic expected to stretch far into 2021, clinical laboratories will continue to play a crucial role in the nation’s healthcare response to COVID-19. As essential workers in the fight against infectious disease, clinical pathologists, clinical chemists, and all medical laboratory staff should be prioritized as frontline healthcare workers.
As demand for SARS-CoV-2 coronavirus testing increases, leaders of the College of American Pathologists meet online to brainstorm possible solutions to the crisis
In September, the College of American Pathologists (CAP) began its series of “virtual media briefings” given by leading pathologists and physicians at the forefront of COVID-19 testing which are designed to “offer insights and straight talk” on the crisis confronting today’s clinical laboratories.
During the third virtual meeting on December 9, presenters discussed how the ever-increasing demand for COVID-19 testing has placed an enormous amount of stress on clinical laboratories, medical technologists (MTs), and clinical laboratory scientists (CLSs) responsible for processing the high volume of SARS-CoV-2 tests, and on the supply chains medical laboratories depend on to receive and maintain adequate supplies of testing materials.
“As soon as we get one set of supplies, then it’s another set of supplies that we can’t get our hands on,” said Christine Wojewoda, MD, Clinical Pathologist and Associate Professor at the University of Vermont Medical Center, during the third CAP virtual briefing. “Right now, we’re very concerned that our lab can’t get pipette tips that have a certain filter in them to transfer patient samples into the tubes that we need, or the plates that we need to do the testing. If we can’t get the patient sample into where it needs to go, safely, without contaminating other patient samples, that’s a big issue.”
Other members of the CAP panel concurred with Wojewoda and indicated that their clinical labs also are encountering supply chain challenges.
“It’s a daily battle,” said Amy Karger, MD, PhD, Clinical Pathologist and Associate Professor at University of Minnesota Physicians. “One of our managers spends hours a day making sure our lab has enough supplies, plastics, and chemicals to do the testing that we want to do. And he is often having to look for alternative solutions for COVID-19 testing, making phone calls, trying to find alternative products, and so we have a consistent worry about that.”
A June survey of CAP-accredited laboratories for COVID-19 testing found that more than 60% of lab directors reported difficulties in procuring critical supplies needed to conduct COVID-19 testing. The respondents indicated they encountered substantial barriers to obtaining equipment needed for SARS-CoV-2 testing—particularly test kits (69%), swabs (66%), and transport media (62%).
Staff Burnout and Shortages at Many Medical Laboratories
Karger also indicated that she is concerned about staff burnout and the toll the workload is taking on medical technologists at her laboratory.
“Lab staff have been working full throttle since March. I think that is often lost on people. They kind of assumed that when cases were low with COVID-19, that maybe the lab staff got a break. Well, that wasn’t the case,” she stated, adding, “They [the medical technologists] were planning for this surge that we’re experiencing now and have been working often seven days a week, double shifts to get us to this point of high testing capacity [to respond to the demand for COVID-19 testing].”
Another member of the CAP panel echoed Karger’s concerns.
“We worry about that as well,” said Patrick Godbey, MD, Founder and Laboratory Director at Southeastern Pathology Associates and current CAP President. “This demand for COVID-19 testing has made an already bad situation worse because there’s an absolute shortage of medical laboratory personnel and the increased demands on clinical labs have made this shortage even more acute.”
Almost all of the surveyed CAP-accredited laboratories reported losses in revenue and financial stress since the pandemic started. But few had applied for any of the available funds offered through federal assistance programs. The survey found that the top issues among pathologists reported by laboratory directors were:
reduced work hours (72%),
reductions in pay (41%),
increased burnout (21%), and
increased work hours (20%).
According to the survey, the top stresses affecting non-pathologist professionals working in clinical labs were:
The diminishing labor pool trained for COVID-19 testing—coupled with high stress/burnout among existing staff—is a major impediment to ongoing expansion in the daily number of molecular COVID-19 tests that can be performed by the nation’s labs.
Also, the already-tight supply of med techs means many metropolitan area labs—particularly hospital labs—are operating with just 75% of the number of staff they are authorized to hire, because there are no techs available. Thus, existing staff are working lots of overtime, and vacant FTE positions are being temporarily filled by MTs placed by employment agencies.
A New York Times (NYT) article in December, titled, “‘Nobody Sees Us’: Testing-Lab Workers Strain Under Demand,” revealed that testing teams across the country are dealing with “burnout, repetitive-stress injuries, and an overwhelming sense of doom.” The article reported on the shortages of supplies needed to perform testing and states there is a “dearth of human power” in the field of pathology as well.
The supply of MTs and CLSs, molecular PhDs, clinical pathologists, MLTs, and other laboratory scientists available to work in the nation’s labs is finite and training programs take years to produce qualified workers to perform laboratory testing.
In the NYT article, microbiologist Karissa Culbreath, PhD (above), Scientific Director, Infectious Diseases at TriCore Reference Laboratories, and Assistant Professor of Pathology at the University of New Mexico, said that when shortages arise, “there are workarounds for almost everything else, but people are irreplaceable.” In addition to the large volume of COVID-19 tests that labs are expected to perform, they also must keep up with the other tests that are sent to them for analysis. Some facilities are even transitioning to 24/7 testing to keep up with the demand. “Labs are trying to maintain our standard of operation with everything else, with a pandemic on top of it,” said Culbreath. (Photo copyright: KOB 4/NBC.)
Should Clinical Lab Workers Be First to Receive the COVID-19 Vaccine?
In the third CAP virtual media briefing, the panel suggested that medical laboratory workers should be among the first to receive the COVID-19 vaccine.
“They are encountering and handling thousands of samples that have active live virus in them,” Karger said. “We are getting 10,000 samples a day [for SARS-CoV-2 testing]. That’s a lot of handling of infectious specimens and we do want them to be prioritized for vaccination.”
She added, “From an operational standpoint, we need to keep our lab up and running. We don’t want to have staff out such that we would have to decrease our SARS-CoV-2 testing capacity, which would have widespread impact on our health system and our state.”
Since the pandemic began nearly a year ago, there have been more than 18 million cases of COVID-19 confirmed in the US and more than 300,000 people have died from the virus, according to data from the federal Centers for Disease Control and Prevention (CDC).
And, as we move into flu season, the number of new COVID-19 cases is reportedly increasing, which adds more stress to clinical laboratories and their supply chains. As this is unlikely to end anytime soon, clinical lab managers must find new ways to do more with less.
Pathologists and clinical laboratory scientists know that influenza vaccines typically produce short-lived protection and researchers have new clues as to why this is true
With so much interest in development of a COVID-19 vaccine, findings by researchers at Atlanta’s Emory Vaccine Center into why the vaccine for influenza (Flu) is so short-lived offer a new window on how the body’s immune system responds to invading viruses and what happens to the immunity over time.
Because the autumn influenza season is just weeks away, these insights into the body’s immune response to influenza will be of interest to clinical laboratories that provide testing for influenza, as well as SARS-CoV-2, the coronavirus that causes COVID-19.
Clinical laboratory managers recognize that an influenza vaccine is an annual imperative for people—especially the elderly and those with existing comorbidities—and medical laboratory tests are typically used to diagnose the illness and identify which strains of viruses are present. The flu vaccine is even more important amid the COVID-19 pandemic, infectious disease authorities say.
The scientists at the Emory Vaccine Center published their findings in the journal Science.
Not so with influenza vaccines. The immunity they impart generally only lasts for a single flu season and are “lost within one year,” the Emory study notes.
As Genetic Engineering and Biotechnology News (GEN) explains, the influenza genome has eight RNA segments which can change as the virus enters a cell. This antigenic shift creates new influenza strains that require updated vaccines, GEN noted.
However, the Emory researchers stated that “The fact that a small number did persist over one year raises prospects that the longevity of flu vaccines can be improved and provides key information for the development of universal vaccines against influenza.”
Bone Marrow Has Major Role in Producing New Flu Antibodies
The Emory study focused on the influenza vaccine’s role in how it affects the immune system and what needs to change to create a longer-lasting influenza vaccine. “Our results suggest that most bone marrow plasma cells (BMPC) generated by influenza vaccination in adults are short-lived. Designing strategies to enhance their persistence will be key,” the Emory researchers wrote in Science.
The scientists analyzed bone marrow from 53 healthy volunteers (age 20 to 45). An Emory news release states that bone marrow is the “home base for immune cells producing antibodies.”
Besides the bone marrow, the researchers also examined blood samples from the volunteers, all of which was collected between 2009 and 2018:
before influenza vaccination,
one month after influenza vaccination, and
one year post vaccination.
Through DNA sequencing the samples, the Emory researchers found the number of flu-specific cells increased from 0.8% to 1.9% after one month. They concluded that an annual vaccine does increase antibody-producing cells for influenza in bone marrow.
However, in follow-up visits one year after vaccination, they found that the number of cells present in the volunteers had fallen back to the starting point.
“Specific cells produced by the vaccine … produced unique antibodies that can be identified using sequencing techniques,” Carl Davis, PhD, postdoctoral fellow in the Rafi Ahmed Laboratory at Emory and first author of the paper, said in the news release, adding, “We could see that these new antibodies expanded in the bone marrow one month after vaccination and then contracted after one year.”
He continued, “On the other hand, antibodies against influenza that were in the bone marrow before the vaccine was given stayed at a constant level over one year.”
Vaccine Adjuvants Help Boost Immunity
A vaccine additive called an adjuvant could be the answer to extending the power of influenza vaccines, the Emory scientists noted.
“Just getting to the bone marrow is not enough. A plasma cell has to find a niche within the bone marrow and establish itself there and undergo gene expression and metabolism changes that promote longevity,” Rafi Ahmed, PhD, Director of the Emory Vaccine Center, said in the news release.
“It’s totally crazy (that the most commonly used influenza vaccines don’t include an adjuvant), Ahmed told Science. “I’m hoping that things will change in the influenza vaccine world, and 10 years from now, you will not be getting any nonadjuvanted vaccines.”
According to USA Today, about 20-million “essential” workers will likely be the first to receive the new COVID-19 vaccine and participate in check-in text messages with the Centers for Disease Control and Prevention (CDC) by the end of 2020.
In its COVID-19 vaccine testing, Novavax, a late-state biotechnology company, suggests that “an adjuvant is critical to its vaccine working well,” National Public Radio (NPR) reported in “The Special Sauce That Makes Some Vaccines Work.” However, vaccine developers may be reluctant to share their adjuvant research.
“Adjuvants end up being very proprietary. It’s kind of the secret sauce on how to make your protein vaccine work,” Barney Graham, MD, PhD, Deputy Director, Vaccine Research Center, National Institute of Allergy and Infectious Diseases, told NPR.
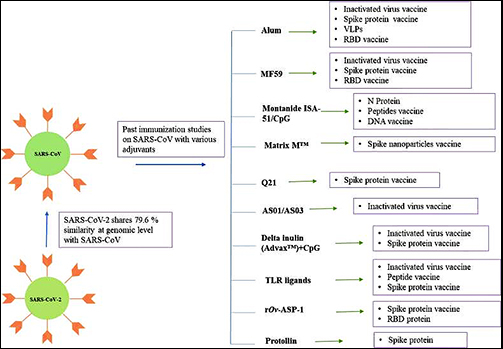
Still, a study published in Immunopharmacology revealed potential adjuvants for the COVID-19 vaccine based on vaccine studies of other coronaviruses. While there are many adjuvants available, not all have safety track records that can be leveraged to gain clearance from regulatory bodies, the researchers pointed out. But some do.
“CpG 1018, MF59, and AS03 are already approved for human vaccine and their inclusion may expedite the vaccine development process. Further, Protollin has shown promising results in pre-clinical studies,” the authors wrote.
Clinical laboratories that provide influenza testing will want to follow these types of research studies. Findings on immunity will affect development of vaccines that medical labs provide—including for COVID-19.
Though not a replacement for clinical laboratory testing, the CDC says the surveillance system will help slow spread of COVID-19 in vulnerable communities
Clinical laboratory testing for COVID-19 is receiving an ally. In mid-August, the Centers for Disease Control and Prevention (CDC) and the US Department of Health and Human Services (HHS) announced they were initiating a National Wastewater Surveillance System (NWSS) in response to the COVID-19 pandemic.
In collaboration with other federal agencies, the NWSS will work with state, local, territorial, and tribal health departments to collect data on wastewater (aka, sewage) samples throughout the United States.
The goal of the NWSS is to detect SARS-CoV-2, the coronavirus that causes COVID-19, before it spreads by detecting traces of it in local sewer systems. The level of the virus detected in wastewater can be a leading indicator of a worsening outbreak in a community, according to a CDC statement.
“Quantitative SARS-CoV-2 measurements in untreated sewage can provide information on changes in total COVID-19 infection in the community contributing to that wastewater treatment plant,” noted the CDC.
People infected with the coronavirus discard traces of it—whether they are symptomatic or asymptomatic—and levels of the virus in untreated sewage can provide scientists with information about the degree of outbreak in specific areas.
The NWSS will not include or monitor homes that use septic tanks or entities with decentralized systems that treat their own waste, such as hospitals, universities, and prisons.
Not a Replacement for Clinical Laboratory Testing
The CDC stressed that sewage testing is not meant to replace clinical laboratory testing, but it can be a valuable tool in communities where COVID-19 tests are underutilized or unavailable. Wastewater testing, CDC noted in its statement, could have an enormous reach as 80% of households in the US are connected to a municipal sewage system.
The CDC is not actively taking samples from wastewater, but relying on local partners to take samples, test them, and enter data into the NWSS portal for the purpose of summarizing and interpreting for public health action.
The agency predicts that participation in a national database will ensure data comparability across separate jurisdictions.
Could Testing Raw Sewage Be More Effective than Contact Tracing for Tracking COVID-19 Outbreaks?
A Yale University study published in Nature Biotechnology, titled, “Measurement of SARS-CoV-2 RNA in Wastewater Tracks Community Infection Dynamics,” detected SARS-CoV-2 concentrations in sewage sludge in New Haven, Conn., over a 10-week period earlier this year. The results of the study “show the utility of viral RNA monitoring in municipal wastewater for SARS-CoV-2 infection surveillance at a population-wide level,” the study authors noted.
The published study states that “SARS-CoV-2 RNA was detected throughout the more than 10-week study and, when adjusted for time lags, tracked the rise and fall of cases seen in SARS-CoV-2 clinical test results and local COVID-19 hospital admissions. Relative to these indicators, SARS-CoV-2 RNA concentrations in sludge were 0–2 [days] ahead of SARS-CoV-2 positive test results by date of specimen collection, 0–2 [days] ahead of the percentage of positive tests by date of specimen collection, 1–4 [days] ahead of local hospital admissions and 6–8 [days] ahead of SARS-CoV-2 positive test results by reporting date.”
The Yale researchers concluded, “Our results demonstrate that measurement of SARS-CoV-2 RNA concentrations in primary sludge provides an approach to estimate changes in COVID-19 prevalence on a population level. Sludge results were not a leading indicator compared to positive test results or percentage of positive tests by date of specimen collection. However, they led hospitalizations by 1–4 [days] and test results by report date by ~1 week. Thus, in communities where test reporting is delayed, sludge results, if analyzed and reported on the same day as sampling, can provide substantial advance notice of infection dynamics.”
Jordan Peccia, Jr., PhD (above), Professor of Chemical and Environmental Engineering at the Yale School of Engineering and Applied Science, and study author, told NBC News, “There’s still a lot more to do. We’re one of the earlier groups to have developed a robust relationship between wastewater and coronavirus cases, but this is just a first step.” He added, “It doesn’t replace contact tracing. [But] if we know a little bit ahead of time, we can raise the alarm.” (Photo copyright: Yale University.)
Sewage Testing for COVID-19 Around the World
Sewage testing can provide data to complement other collected information about COVID-19 and steer public health decision-making. However, the CDC notes that “it is not possible to reliably and accurately predict the number of infected individuals in a community based on sewage testing” and that “more data on fecal shedding by infected individuals over the course of disease are needed to better understand the limits of detection.”
Nevertheless, some experts have leaned heavily on sewage sample testing for their conclusions about the origination of the coronavirus. In August, Dark Daily reported on a theory based on finding remnants of SARS-CoV-2 in sewage systems that suggested the virus may not have originated in Wuhan, China. Analysis of sewage samples in Italy, Spain, and Brazil indicated the virus was present in those countries before the disease was known to exist outside of China. The controversy over these findings has motivated virologists to expand wastewater testing.
The creation of the NWSS by the CDC validates growing interest in new methods of testing for infectious disease. Lower cost, faster response time, more automation of genetic sequencing, and improved analytical software has enabled this type of testing to become a useful tool. It would be wise for clinical laboratory managers to monitor the expanded use of new testing technologies for infectious diseases.