Pathologists and clinical laboratory scientists know that influenza vaccines typically produce short-lived protection and researchers have new clues as to why this is true
With so much interest in development of a COVID-19 vaccine, findings by researchers at Atlanta’s Emory Vaccine Center into why the vaccine for influenza (Flu) is so short-lived offer a new window on how the body’s immune system responds to invading viruses and what happens to the immunity over time.
Because the autumn influenza season is just weeks away, these insights into the body’s immune response to influenza will be of interest to clinical laboratories that provide testing for influenza, as well as SARS-CoV-2, the coronavirus that causes COVID-19.
Clinical laboratory managers recognize that an influenza vaccine is an annual imperative for people—especially the elderly and those with existing comorbidities—and medical laboratory tests are typically used to diagnose the illness and identify which strains of viruses are present. The flu vaccine is even more important amid the COVID-19 pandemic, infectious disease authorities say.
The scientists at the Emory Vaccine Center published their findings in the journal Science.
Not so with influenza vaccines. The immunity they impart generally only lasts for a single flu season and are “lost within one year,” the Emory study notes.
As Genetic Engineering and Biotechnology News (GEN) explains, the influenza genome has eight RNA segments which can change as the virus enters a cell. This antigenic shift creates new influenza strains that require updated vaccines, GEN noted.
However, the Emory researchers stated that “The fact that a small number did persist over one year raises prospects that the longevity of flu vaccines can be improved and provides key information for the development of universal vaccines against influenza.”
Bone Marrow Has Major Role in Producing New Flu Antibodies
The Emory study focused on the influenza vaccine’s role in how it affects the immune system and what needs to change to create a longer-lasting influenza vaccine. “Our results suggest that most bone marrow plasma cells (BMPC) generated by influenza vaccination in adults are short-lived. Designing strategies to enhance their persistence will be key,” the Emory researchers wrote in Science.
The scientists analyzed bone marrow from 53 healthy volunteers (age 20 to 45). An Emory news release states that bone marrow is the “home base for immune cells producing antibodies.”
Besides the bone marrow, the researchers also examined blood samples from the volunteers, all of which was collected between 2009 and 2018:
before influenza vaccination,
one month after influenza vaccination, and
one year post vaccination.
Through DNA sequencing the samples, the Emory researchers found the number of flu-specific cells increased from 0.8% to 1.9% after one month. They concluded that an annual vaccine does increase antibody-producing cells for influenza in bone marrow.
However, in follow-up visits one year after vaccination, they found that the number of cells present in the volunteers had fallen back to the starting point.
“Specific cells produced by the vaccine … produced unique antibodies that can be identified using sequencing techniques,” Carl Davis, PhD, postdoctoral fellow in the Rafi Ahmed Laboratory at Emory and first author of the paper, said in the news release, adding, “We could see that these new antibodies expanded in the bone marrow one month after vaccination and then contracted after one year.”
He continued, “On the other hand, antibodies against influenza that were in the bone marrow before the vaccine was given stayed at a constant level over one year.”
Vaccine Adjuvants Help Boost Immunity
A vaccine additive called an adjuvant could be the answer to extending the power of influenza vaccines, the Emory scientists noted.
“Just getting to the bone marrow is not enough. A plasma cell has to find a niche within the bone marrow and establish itself there and undergo gene expression and metabolism changes that promote longevity,” Rafi Ahmed, PhD, Director of the Emory Vaccine Center, said in the news release.
“It’s totally crazy (that the most commonly used influenza vaccines don’t include an adjuvant), Ahmed told Science. “I’m hoping that things will change in the influenza vaccine world, and 10 years from now, you will not be getting any nonadjuvanted vaccines.”
According to USA Today, about 20-million “essential” workers will likely be the first to receive the new COVID-19 vaccine and participate in check-in text messages with the Centers for Disease Control and Prevention (CDC) by the end of 2020.
In its COVID-19 vaccine testing, Novavax, a late-state biotechnology company, suggests that “an adjuvant is critical to its vaccine working well,” National Public Radio (NPR) reported in “The Special Sauce That Makes Some Vaccines Work.” However, vaccine developers may be reluctant to share their adjuvant research.
“Adjuvants end up being very proprietary. It’s kind of the secret sauce on how to make your protein vaccine work,” Barney Graham, MD, PhD, Deputy Director, Vaccine Research Center, National Institute of Allergy and Infectious Diseases, told NPR.
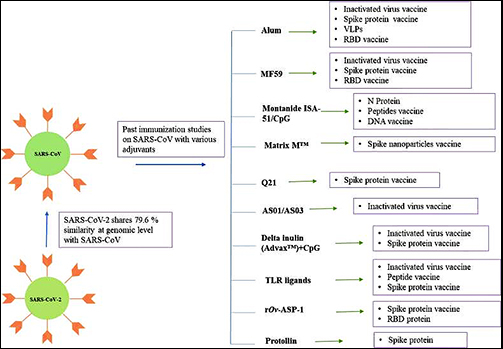
Still, a study published in Immunopharmacology revealed potential adjuvants for the COVID-19 vaccine based on vaccine studies of other coronaviruses. While there are many adjuvants available, not all have safety track records that can be leveraged to gain clearance from regulatory bodies, the researchers pointed out. But some do.
“CpG 1018, MF59, and AS03 are already approved for human vaccine and their inclusion may expedite the vaccine development process. Further, Protollin has shown promising results in pre-clinical studies,” the authors wrote.
Clinical laboratories that provide influenza testing will want to follow these types of research studies. Findings on immunity will affect development of vaccines that medical labs provide—including for COVID-19.
Though not a replacement for clinical laboratory testing, the CDC says the surveillance system will help slow spread of COVID-19 in vulnerable communities
Clinical laboratory testing for COVID-19 is receiving an ally. In mid-August, the Centers for Disease Control and Prevention (CDC) and the US Department of Health and Human Services (HHS) announced they were initiating a National Wastewater Surveillance System (NWSS) in response to the COVID-19 pandemic.
In collaboration with other federal agencies, the NWSS will work with state, local, territorial, and tribal health departments to collect data on wastewater (aka, sewage) samples throughout the United States.
The goal of the NWSS is to detect SARS-CoV-2, the coronavirus that causes COVID-19, before it spreads by detecting traces of it in local sewer systems. The level of the virus detected in wastewater can be a leading indicator of a worsening outbreak in a community, according to a CDC statement.
“Quantitative SARS-CoV-2 measurements in untreated sewage can provide information on changes in total COVID-19 infection in the community contributing to that wastewater treatment plant,” noted the CDC.
People infected with the coronavirus discard traces of it—whether they are symptomatic or asymptomatic—and levels of the virus in untreated sewage can provide scientists with information about the degree of outbreak in specific areas.
The NWSS will not include or monitor homes that use septic tanks or entities with decentralized systems that treat their own waste, such as hospitals, universities, and prisons.
Not a Replacement for Clinical Laboratory Testing
The CDC stressed that sewage testing is not meant to replace clinical laboratory testing, but it can be a valuable tool in communities where COVID-19 tests are underutilized or unavailable. Wastewater testing, CDC noted in its statement, could have an enormous reach as 80% of households in the US are connected to a municipal sewage system.
The CDC is not actively taking samples from wastewater, but relying on local partners to take samples, test them, and enter data into the NWSS portal for the purpose of summarizing and interpreting for public health action.
The agency predicts that participation in a national database will ensure data comparability across separate jurisdictions.
Could Testing Raw Sewage Be More Effective than Contact Tracing for Tracking COVID-19 Outbreaks?
A Yale University study published in Nature Biotechnology, titled, “Measurement of SARS-CoV-2 RNA in Wastewater Tracks Community Infection Dynamics,” detected SARS-CoV-2 concentrations in sewage sludge in New Haven, Conn., over a 10-week period earlier this year. The results of the study “show the utility of viral RNA monitoring in municipal wastewater for SARS-CoV-2 infection surveillance at a population-wide level,” the study authors noted.
The published study states that “SARS-CoV-2 RNA was detected throughout the more than 10-week study and, when adjusted for time lags, tracked the rise and fall of cases seen in SARS-CoV-2 clinical test results and local COVID-19 hospital admissions. Relative to these indicators, SARS-CoV-2 RNA concentrations in sludge were 0–2 [days] ahead of SARS-CoV-2 positive test results by date of specimen collection, 0–2 [days] ahead of the percentage of positive tests by date of specimen collection, 1–4 [days] ahead of local hospital admissions and 6–8 [days] ahead of SARS-CoV-2 positive test results by reporting date.”
The Yale researchers concluded, “Our results demonstrate that measurement of SARS-CoV-2 RNA concentrations in primary sludge provides an approach to estimate changes in COVID-19 prevalence on a population level. Sludge results were not a leading indicator compared to positive test results or percentage of positive tests by date of specimen collection. However, they led hospitalizations by 1–4 [days] and test results by report date by ~1 week. Thus, in communities where test reporting is delayed, sludge results, if analyzed and reported on the same day as sampling, can provide substantial advance notice of infection dynamics.”
Jordan Peccia, Jr., PhD (above), Professor of Chemical and Environmental Engineering at the Yale School of Engineering and Applied Science, and study author, told NBC News, “There’s still a lot more to do. We’re one of the earlier groups to have developed a robust relationship between wastewater and coronavirus cases, but this is just a first step.” He added, “It doesn’t replace contact tracing. [But] if we know a little bit ahead of time, we can raise the alarm.” (Photo copyright: Yale University.)
Sewage Testing for COVID-19 Around the World
Sewage testing can provide data to complement other collected information about COVID-19 and steer public health decision-making. However, the CDC notes that “it is not possible to reliably and accurately predict the number of infected individuals in a community based on sewage testing” and that “more data on fecal shedding by infected individuals over the course of disease are needed to better understand the limits of detection.”
Nevertheless, some experts have leaned heavily on sewage sample testing for their conclusions about the origination of the coronavirus. In August, Dark Daily reported on a theory based on finding remnants of SARS-CoV-2 in sewage systems that suggested the virus may not have originated in Wuhan, China. Analysis of sewage samples in Italy, Spain, and Brazil indicated the virus was present in those countries before the disease was known to exist outside of China. The controversy over these findings has motivated virologists to expand wastewater testing.
The creation of the NWSS by the CDC validates growing interest in new methods of testing for infectious disease. Lower cost, faster response time, more automation of genetic sequencing, and improved analytical software has enabled this type of testing to become a useful tool. It would be wise for clinical laboratory managers to monitor the expanded use of new testing technologies for infectious diseases.
Multiple recent studies reveal a substantial number of patients continue to delay needed healthcare in the months since the onset of the SARS-CoV-2 outbreak
Based on an analysis of hospital emergency department (ED) usage, federal researchers concluded that patients continue to be cautious when visiting healthcare providers, including clinical laboratories, and that people are altering how they seek and utilize emergency care due to the COVID-19 pandemic. This not only reduces the number of typical test orders from the ER to the hospital lab, but also reduces the source of inpatient admissions.
Between March 29 and April 25 of this year, facilities the CDC examined recorded 1.2 million visits to EDs, compared to 2.1 million visits between March 31 and April 27 of last year. The steepest decrease in patient demographics was for individuals under the age of 14, women, and people living in the Northeast region.
The CDC’s data showed that 12% of ED visits were for children in pre-pandemic 2019, which dropped to 6% during the 2020 pandemic period. The CDC included ED visits from hospitals in 47 states (excluding Hawaii, South Dakota, and Wyoming) and captured information from approximately 73% of ED visits in the US.
Delaying Healthcare Visits Worsens Medical Conditions, Reduces Revenues
ED visits are an important referral source for inpatient admissions. Fewer patients in EDs means lost revenue for hospitals. However, one positive aspect of the waning number of ED visits is that it may be keeping patients with non-emergency situations away from emergency departments, thus reducing the overuse of costly ED visits. But healthcare professionals are concerned that individuals also may be avoiding or delaying care when needed, which could worsen medical situations and outcomes.
“We saw people, with COVID-19 and without, coming into the ED who were very ill,” Vik Reddy, MD, Chief Medical Officer at Wellstar Kennestone Hospital and Wellstar Windy Hill Hospital in the Atlanta area, told Modern Healthcare. He noted that some patients delayed care for critical non-COVID-19 illnesses. “The good news is that we’re seeing that trend reverse this time around. It was scary in March when we knew that people weren’t coming into the ED for heart attacks.”
The NSSP’s analysis concluded that the report’s findings were subject to at least four limitations:
The number of hospitals reporting to NSSP changes over time as facilities are added or closed. For example, 3,173 hospitals reported data in April of 2019, while 3,467 reported data in April 2020.
Diagnostic categories rely on the use of specific codes, which were missing in 20% of the ED visits reported.
NSSP coverage is not uniform across or within all the participating states.
The analysis is limited only to ED visits and does not take into account patients who did not go to an ED, but instead received treatment in other healthcare environments, such as urgent care clinics.
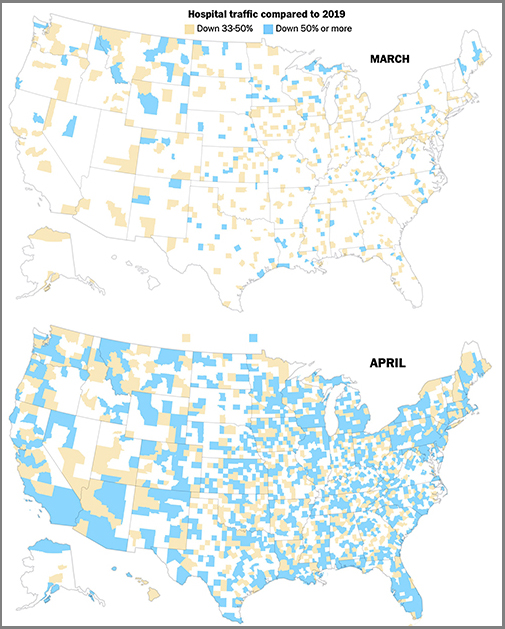
The graphics above are taken from a Washington Post article which reported that the newspaper’s analysis of smartphone location data of hospital traffic in 2020 showed the “drop” in hospital usage had turned into “a crash,” compared to the same two months last year, and that, “As in many other industries, those lost visits represented a widespread financial crisis for hospitals and other healthcare providers, even in places the novel coronavirus hardly touched.” (Graphics copyright: The Washington Post.)
Additional Studies Show Patients Avoiding Hospital EDs, Delaying Care
Other sources also are reporting similar findings regarding consumer attitudes towards seeking medical care during the COVID-19 pandemic. A PricewaterhouseCoopers survey released in May found that about 45% of 2,500 consumers surveyed plan to forgo their annual physical in 2020, due to the pandemic, Modern Healthcare reported.
In addition, an Optum Consumer Pulse Survey released in May found that nearly 20% of 700 surveyed individuals stated they were likely to avoid hospital EDs even if they were showing signs of a heart attack or appendicitis. Another 40% stated they were likely to avoid the ED if they had a cut that required stitches.
In “Americans Are Delaying Medical Care, and It’s Devastating Health-Care Providers,” The Washington Post analyzed hospital use during the pandemic based on smartphone tracking data. WaPo’s report found a significant drop in patients seeking in-person healthcare with many areas across the country reporting a 50% reduction in patients when compared to last year.
The article also states that almost 94 million people have delayed medical care due to the COVID-19 pandemic, and that 66 million of those individuals needed medical care unrelated to the virus but did not receive it.
These studies and others are showing a pattern. The COVID-19 pandemic has changed when and where patients access healthcare, and if the trend continues, it could have a long-term impact on clinical laboratories. Since fewer people are seeking medical care, fewer laboratory tests are being ordered and performed, which means less work and revenue for the nations’ hospital and independent clinical labs.
The CDC and US Navy study reveals common symptoms and suggests best protective measures to prevent spread in enclosed environments that clinical labs and pathology groups could use to protect their staff members
Results from a study conducted by the US Navy and the federal Centers for Disease Control and Prevention (CDC) of sailors onboard the USS Theodore Roosevelt during the recent COVID-19 outbreak aboard the ship may be useful for pathologists and clinical laboratory managers. The study also provides public health and infectious disease specialists with an opportunity to learn more about how the SARS-CoV-2 coronavirus spreads in enclosed environments.
The aircraft carrier garnered headlines in April due to a widespread outbreak of the coronavirus among its crew. The investigators asked crewmembers to complete a questionnaire and provide samples for a serological antibody test and molecular diagnostics test, reported the Navy’s Bureau of Medicine and Surgery (BUMED). The goal was to learn more about the disease and how it spreads in high-density environments. The COVID-19 tests were conducted April 20-24 while the ship was docked in Guam.
“This study paints a picture of current and prior SARS-CoV-2 infection among young adults living in close quarters,” said the study’s lead author Dan Payne, PhD, an epidemiologist at the CDC, in the BUMED statement. “This data will contribute to understanding COVID-19 in the US military, as well as among young adults in other close communal environments.”
Participation in the study was voluntary. At the time of testing, a total of 1,417 service members were still on the ship or at the base in Guam, the researchers wrote in their study. Among them, 383 crewmembers agreed to complete the survey and provide a blood sample for an enzyme-linked immunosorbent assay (ELISA) antibody test. Out of that group, 267 also provided nasal swab samples for a reverse transcription polymerase chain reaction (RT-PCR) molecular diagnostic test.
A clinical laboratory team from the Naval Hospital Guam and the Navy and Marine Corps Public Health Center are seen above collecting surveys, nasal swabs, and blood samples from sailors assigned to the aircraft carrier USS Theodore Roosevelt (CVN 71) during the investigation into the COVID-19 outbreak in April. The ship’s medical leaders established an emergency command center, initiated a roving and deep cleaning team, and continually educated the crew on social distancing and proper protective procedures and behaviors, to mitigate the spread of the SARS-CoV-2 coronavirus. (Photo copyright: US Navy.)
The questionnaire sought information about sailors’ demographic factors, health history, symptoms, and preventive behaviors, such as mask wearing and physical distancing. Crewmembers who tested positive for reactive antibodies received an additional test to detect presence of neutralizing antibodies that inhibit the virus.
The median age of participants was 30 years. About 75% were male. Only 28 (7.3%) reported comorbidities such as a history of asthma, diabetes, hypertension, or immunosuppression, which are considered risk factors for developing serious cases of the COVID-19 disease.
Key findings of the CDC/Navy’s study:
228 participants (59.7%) tested positive for reactive antibodies. Of those, 135 (59.2%) tested positive for neutralizing antibodies.
235 participants had previously tested positive in a SARS-CoV-2 diagnostic test. Of those, 212 (90.2%) tested positive for reactive antibodies.
A total of 238 participants had a previous or current SARS-CoV-2 infection. Of these, 18.5% reported no symptoms.
Of the 194 sailors who reported symptoms, 115 (59.3%) sought medical care, and two were hospitalized.
The most frequently reported symptoms were headache (66.5%), loss of taste or smell or both (61.3%); myalgia (56.2%); runny nose (55.7%); and fatigue (55.2%).
The most effective preventive measures were avoidance of common areas, increased physical distancing, and use of face coverings.
“What we saw was that most of the infections were actually mild, in addition to those that were asymptomatic,” Payne told reporters after the study was published, reported CNN. “And this is perhaps different from studies of older Americans, or maybe even those who were hospitalized already, and certainly much different from those with underlying health conditions.”
But with the high number of asymptomatic cases, “symptom-based surveillance might not detect all infections,” noted the researchers, who cautioned that “the analysis was conducted on a convenience sample of persons who might have had a higher likelihood of exposure, and all information was based on self-report, raising the possibility of selection and recall biases.”
In January, the crew of the Roosevelt totaled about 4,800 sailors, reported Defense One. However, after docking in Guam, many sailors were moved to hotel rooms for quarantine. As of May 5, at least 1,156 crewmembers had tested positive for infection, Stars and Stripes reported, and one had died.
Sailors aboard the USS Theodore Roosevelt were examined prior to reboarding the ship following off-ship quarantine or isolation. Only those found to be negative for the coronavirus, were allowed to board the ship. (Photo copyright: US Navy.)
Impact of COVID-19 on the USS Theodore Roosevelt’s Crew
As of April 6, 172 crew members had tested positive for COVID-19, including the ship’s captain Brett Crozier. At that time, 61% of the crew had received clinical laboratory testing and 1,999 sailors had been moved off the ship into quarantine, reported Defense One. By the next day, 270 sailors tested positive, a 57% increase from the previous day.
By April 14, 589 crew members were diagnosed positive for COVID-19. With 92% of the crew tested, 3,922 were found to be negative for the infection. Nevertheless, 4,024 sailors—nearly 83% of the crew—were moved into isolation quarters off-ship to prevent spread of the coronavirus.
In their study, the Navy/CDC researchers concluded: “In this convenience sample of young, healthy US service members experiencing close contact aboard an aircraft carrier, those with previous or current SARS-CoV-2 infection experienced mild illness overall, and nearly 20% were asymptomatic. Approximately one third of participants reported fever, myalgia, and chills and had higher odds of SARS-CoV-2 infection than did persons who reported cough and shortness of breath. Participants reporting anosmia (loss of sense of smell) or ageusia (loss of sense of taste) had 10 times the odds of having infection, compared with those who did not.
“In this sample of intensely exposed subjects, assessed at a single point in time, results demonstrated that antibodies developed and that, at the time of specimen collection, many of these were neutralizing antibodies. … This is a promising indicator of immunity, and in several participants, neutralizing antibodies were still detectable >40 days after symptom onset. Ongoing studies assessing the humoral antibody response over time will aid the interpretation of serologic results in an outbreak investigation such as this.
“These results provide new indications of symptomatology of SARS-CoV-2 infections and serologic responses among a cohort of young US adults living in a congregate environment and contribute to a better understanding of COVID-19 epidemiology in the US military. The findings reinforce the importance of nonpharmaceutical interventions such as wearing a face covering, avoiding common areas, and observing social distancing to lower risk for infection in similar congregate living settings.”
Not all the specific lessons learned from this COVID-19 outbreak aboard a US Navy vessel will be applicable to clinical laboratories and anatomic pathology groups. Nevertheless, it is probable that the data gleaned from the CDC/Navy study aboard the USS Theodore Roosevelt will someday mean civilian Americans can count on improved responses to disease outbreaks from the nation’s testing laboratories.
Washington Post investigation outlines scientists’ frustrations in the early days of the pandemic, as they worked to deploy laboratory-developed tests for the novel coronavirus
In the wake of the failed rollout of the Centers for Disease Control and Prevention’s (CDC) COVID-19 diagnostic test last February, many CLIA-certified academic and public health laboratories were ready, and had the necessary resources, to develop their own coronavirus molecular diagnostic tests to help meet the nationwide demand for clinical laboratory testing. However, the response from the US Food and Drug Administration (FDA) was, in essence, “not so fast.”
In this second part of Dark Daily’s two-part e-briefing, we continue our coverage of the Washington Post (WP) investigation that detailed the regulatory hurdles which blocked private laboratories from deploying their own laboratory-developed tests (LDTs) for COVID-19. The report is based on previously unreported email messages and other documents reviewed by the WP, as well as the newspaper’s exclusive interviews with scientists and officials involved.
The CDC’s COVID-19 test kits began arriving at public health laboratories on February 8, just 18 days after the first case of the novel coronavirus was confirmed in the US. As the WP noted in an earlier analysis, titled, “What Went Wrong with Coronavirus Testing in the US,” the CDC’s decision to develop its own test was not surprising. “The CDC will develop [its] own test that is suited to an American healthcare context and the regulations that exist here,” explained Jeremy Konyndyk, Senior Policy Fellow at the Center for Global Development. “That’s how we normally would do things.”
But state and local public health laboratories quickly discovered that the CDC test kits were flawed due to problems with one of the reagents. While numerous academic, research, and commercial labs had the capability to produce their own COVID-19 PCR tests, FDA rules initially prevented them from doing so without a federal Emergency Use Authorization (EUA).
The bureaucratic hurdles arose due to Health and Human Services Secretary Alex Azar’s January 31 declaration that COVID-19 was a “health emergency” in the US. By doing so, HHS triggered a mandate that requires CLIA-certified labs at universities, research centers, and hospitals to seek an EUA from the FDA before deploying any laboratory-developed tests.
Scientists, Clinical Laboratories Frustrated by Bureaucratic Delays and Red Tape
To make matters worse, the EUA process was neither simple nor fast, which exasperated lab scientists and clinical laboratory administrators. “In their private communications, scientists at academic, hospital, and public health labs—one layer removed from federal agency operations—expressed dismay at the failure to move more quickly, and frustration at bureaucratic demands that delayed their attempts to develop alternatives to the CDC test,” wrote the WP investigators.
In a Feb. 27 email to other microbiologists, Marc Couturier, PhD, Medical Director at ARUP Laboratories, a national reference laboratory network located in Utah, voiced his irritation with the red tape that stymied private laboratory development of COVID-19 tests. He wrote, “We have the skills and resources as a community, but we are collectively paralyzed by a bloated bureaucratic/administrative process,” reported the WP.
Keith Jerome, MD, PhD (above), Head of the Virology Division at the Fred Hutchinson Cancer Research Center in Seattle, maintains federal regulations muted one of the nation’s greatest assets in the fight against COVID-19. “The great strength the US has always had, not just in virology, is that we’ve always had a wide variety of people and groups working on any given problem,” he told MIT Technology Review. “When we decided all coronavirus testing had to be done by a single entity, even one as outstanding as CDC, we basically gave away our greatest strength.” (Photo copyright: Jonathan Hamilton/NPR.)
‘FDA Should Not Treat Labs Like They Are Creating Commercial Products’
According to Kaiser Health News (KHN), Greninger was able to identify one of the nation’s first cases of community-acquired COVID-19 by taking “advantage of a regulatory loophole that allowed the lab to test samples obtained for research purposes from UW’s hospitals.”
But navigating the EUA process was a different story, Greninger told the WP. He spent more than 100 hours filling out forms and collecting information needed for the EUA application. After emailing the application to the FDA, Greninger received a reply containing eCopy Guidance telling him he needed to resubmit the information to the Document Control Center (DCC) at the Center for Devices and Radiological Health (CDRH), a federal agency Greninger knew nothing about. Another FDA rule required that the submission be copied to a hard disk and mailed to the DCC.
In an interview with ProPublica, Greninger stated that after he submitted his COVID-19 test—which copies the CDC protocol—an FDA reviewer told him he would need to prove the test would not show a positive result for someone infected with either a SARS or MERS coronavirus. The first SARS coronavirus disappeared in mid-2003 and the only two cases of MERS in the US were diagnosed in 2014. Greninger told ProPublica it took him two days to locate a clinical laboratory that could provide the materials he needed.
Greninger maintains the FDA should not treat all clinical laboratories as though they are making a commercial product. “I think it makes sense to have this regulation when you’re going to sell 100,000 widgets across the US. That’s not who we are,” he told ProPublica.
FDA Changes Course
Under pressure from clinical laboratory scientists and medical doctors, by the end of February the FDA had issued new policy that enabled CLIA-certified laboratories to immediately use their validated COVID-19 diagnostics while awaiting an EUA. “This policy change was an unprecedented action to expand access to testing,” said the FDA in a statement.
Since then, the FDA has continued to respond—albeit slowly—to scientists’ complaints about regulations that hampered the nation’s COVID-19 testing capacity.
Clinical laboratory leaders and pathologists involved in testing for the SARS-CoV-2 coronavirus should monitor the FDA’s actions and be aware of when and if certain temporary changes the agency implemented during the early days of the COVID-19 pandemic become permanent.
To read part one of our two-part coverage of the Washington Post’s investigation, click here.