Customer relationship
management (CRM) plays a critical role in helping providers care for patients
with chronic diseases and clinical laboratories are part of those solutions
Home healthcare continues to boom in the US and more
technology companies each year—including Salesforce—strive to expand their
presence within the industry. This represents a significant shift in site of
service for a substantial and growing number of Americans. Equally true is that
home healthcare is an opportunity for clinical laboratories to serve this
increasing proportion of the American population.
Statistics tell the tale behind the boom in home healthcare.
The Centers
for Disease Control and Prevention (CDC) estimates that six in 10 adults in
the United States suffer from chronic diseases, such as cancer, and four in 10
adults live with two or more chronic illnesses.
This means that among medical laboratories and other
providers servicing the home healthcare industry demand for clinical laboratory
testing will increase.
Last year, approximately $103 billion was spent on home
healthcare services and that number is expected to reach $173 billion by 2026,
according to the Centers for Medicare and
Medicaid Services (CMS). Approximately 7.6 million people in the US now
require some level of in-home medical care. The overall employment of in-home
healthcare providers is projected to grow 41% between 2016 and 2026.
Efficient tools that assist home healthcare organizations and
their providers are critical. Customer
Relationship Management (CRM) platforms that combine data gathered during
office visits with patients’ living and economic situations are proving to be powerful
allies for treating chronic disease populations.
Social Determinants
of Health
One such CRM developer, Salesforce,
is rising to the demand by adding new features to its existing Health
Cloud platform. Originally introduced in 2016 as a way to improve how
healthcare and life sciences organizations connect with patients, this product
is one example of how Silicon Valley companies are attempting to make inroads
within the healthcare sector. Health Cloud’s newest functional upgrades include:
These social determinants of health are typically not
included in health records. But they can be vital information for healthcare
providers. Clinical laboratory managers should pay attention to “social
determinants of health” because this term describes a new dimension in medical
care and how patients with chronic diseases are managed.
“A lot of people in healthcare know about the importance of social determinants of health, but the volume of information is so great that being able to display things clearly and concisely in front of the [providers who] are using it—when they need it—makes it more operant and more prominent in the care of that patient,” Joshua Newman, MD, Chief Medical Officer at Salesforce, told MedCity News. (Photo copyright: San Francisco Business Times/Biz Journals.)
This is a critical factor. Healthcare providers who use Salesforce’s
Health Cloud can now record a patient’s social determinant information—such as,
transportation issues, housing status, and care network—directly into that
patient’s profile. Access to this type of information can give healthcare
professionals a more complete understanding of each patient’s unique situation.
Here are some examples from a Salesforce press
release that illustrate how social-determinants-of-health data can help
patients and care providers:
“A care provider that wants to limit a patient’s
risk for readmission can know if the patient has access to transportation or
the ability to purchase healthy meals.
“A life science organization that wants to help
patients adhere to their therapies, or properly use their medical devices, can
see a patient’s employment status and living arrangements, and thus offer the
necessary level of financial and in-home support.
“A payer organization can deliver personalized
preventative or wellness material to members based on the member’s education or
reading level.”
“Our industry continues to centralize and integrate patient
data, but it is critical that we stay focused on improving the patient
experience,” noted Ashwini
Zenooz, MD, in the press release. Zenooz is Salesforce’s Senior Vice
President and General Manager, Global Healthcare and Life Sciences. “By surfacing
critical factors of a patient’s life in a single view, we empower care
providers to personalize patient care experiences and improve outcomes.”
Many
existing CRM products cannot collect data from a variety of sources and then
sort and analyze that information to provide users with actionable
intelligence. Salesforce is attempting to fill that void among health and
medical software products with Health Cloud.
“Healthcare has been slower culturally, politically, and
socially to share their data. But what we’re seeing now is even those
organizations that have historically not shared their data are realizing they
can do a better job if they do,” Newman told MedCity News.
Outside Hospital Care
Increasing
Salesforce has also added a service it calls the Connected
Patient Journey to its Health Cloud platform. This service is an
integration between Health Cloud and Salesforce marketing, which can
personalize information given to patients based on their unique health needs.
Using this feature allows providers to build patient lists and use marketing techniques
to reach patients who would most benefit from specific campaigns and
information.
“The general overarching theme that unites all of these
innovations is that care is gravitating increasingly toward the home or outside
of the hospital and the doctor’s office,” said Newman.
Whether in-hospital or in-home, clinical laboratory tests play
a critical role in healthcare services. The ability for clinical laboratories
to enter patients’ test results data directly into CRM systems like Health
Cloud could help providers utilizing those systems better assist patients with
chronic diseases.
Mobile, wearable, mHealth monitoring devices are a key element of many employer fitness programs and clinical laboratories can play an important role in their success
For years Dark Daily has encouraged clinical laboratories to get involved in corporate wellness programs as a way to support their local communities and increase revenues. Now, leveraging the popularity of mobile health (mHealth) wearable devices, UnitedHealthcare (UHC) has found a new way to incentivize employees participating in the insurer’s Motion walking program. UHC is offering free Apple Watches to employees willing to meet or exceed certain fitness goals.
This is the latest wrinkle in a well-established trend of incentivizing
beneficiaries to meet healthcare goals, such as stopping smoking, losing
weight, reducing cholesterol, and lowering blood pressure.
It’s an intriguing gamble by UHC and presents another opportunity for medical laboratories that are equipped to monitor and validate participants’ progress and physical conditions.
How to Get a Free Apple
Watch and FIT at the Same Time
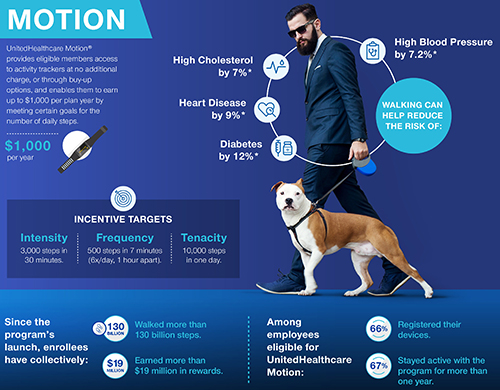
CNBC reported that UHC’s Motion program participants number in the hundreds of thousands. And, according to a UHC news release, they can earn cash rewards up to $1,000 per year. The idea is that participants pay off the cost of their “free” Apple Watch one day at a time by achieving activity goals set in UHC’s FIT tracking method. Those goals include:
Frequency:
500 steps in seven minutes; six times a day, at least one hour apart;
Intensity:
3,000 steps in 30 minutes; and,
Tenacity:
10,000 steps in one day.
“UnitedHealthcare Motion is part of our consumer-focused strategy that is driving toward a simple, integrated, mobile-centric ecosystem that delivers value to consumers,” said Steve Nelson, CEO of UnitedHealthcare, in a news release. “Smartwatches and activity trackers stand alongside transparency in physician selection and medical costs, easy virtual visits with healthcare professionals, and digital coaching and online wellness programs, all of which are designed to support consumers in enhancing their health and improving how they navigate the healthcare system.” Clinical laboratories play a key role in this healthcare strategy. (Graphic copyright: UnitedHealthcare.)
Though hundreds of thousands of beneficiaries are eligible to participate in UHC’s Motion program through their employers, only 45% of those eligible have enrolled in Motion, Fox Business reported.
UHC hopes the offer of a free Apple Watch (which has
applications to track minutes of exercise, a heart rate monitor, and more) will
encourage people to sign up and then progress toward the Motion program’s FIT
goals.
As people meet these goals, they earn $4/day toward the cost
of the Apple Watch. Participants, who do not take enough steps in a six-month period
could be required to repay a percentage of the cost of the smartwatch.
Motion participants who already own an Apple Watch can still
earn up to $1,000 per year in cash rewards for achieving the FIT goals.
“UnitedHealthcare Motion’s success affirms that wearables can play an important role in helping people enhance their well-being and supporting and motivating them to stay engaged in their health,” said Rebecca Madsen, Chief Consumer Officer of UnitedHealthcare, in the UHC news release. (Photo copyright: University of Pennsylvania.)
Impact of mHealth
Programs/Technology Not Clear
Chronic diseases, including diabetes and heart disease, annually cost the US healthcare system $190 billion and employers $126 billion in lost productivity, according to the Centers for Disease Control and Prevention (CDC).
However, some researchers say it’s too early for mHealth
wearables, medication apps, physician virtual engagement, and other digital tools
(many launched within the past five to seven years) to effect key indicators,
such as obesity, life expectancy, and smoking cessation.
“Some of the benefits of these new tools won’t be realized for a long time. It’s really hard to tease out the impact of digital health. Maybe we’re helping people, but we’re not detecting it,” James Murphy, MD, Associate Professor, University of California San Diego Health and radiation oncologist, told CNBC.
Nevertheless, it behooves medical laboratories to develop
procedures for analyzing and reporting data that could impact people who use
wearable mHealth devices to participate in employer wellness programs.
For example, labs could contact insurance companies with
information about biomarkers that provide views into an individual’s progress
toward personal health goals.
Data-driven recommendations from medical laboratories about
tests for chronic conditions such as heart disease and diabetes will likely be
welcomed by payers.
Pharmaceutical tourism, like medical tourism, casts light on healthcare’s true costs and identifies patient populations that bear the brunt of growing drug prices
You’ve heard of medical tourism, where patients travel to other countries to receive low-cost, high-quality medical care. Now the State of Utah is introducing “pharmaceutical tourism” to state employees, who will be paid to make trips to Mexico to purchase certain prescription drugs.
The State of Utah is not alone in its use of this strategy. Prescription medication costs are skyrocketing for many critical drugs. To reign in those costs, several organizations are incentivizing their employees to purchase those drugs less expensively outside of the US. Clinical laboratories and anatomic pathology groups that perform companion diagnostic tests associated with certain high-priced therapeutic drugs might see more of their patients decide to cross international borders to access the drugs they need.
This pharmaceutical tourism highlights how complex US laws
hide the true cost of prescription drugs from patients and their employers. It also
raises the question: how might pharmaceutical tourism impact retail pharmacies
in this country?
Saves Patients Money,
but at What Cost?
The Public Employees Health Plan (PEHP) for Utah state employees recently announced a pharmacy tourism program. Its members can receive free air travel and $500 in cash to fill 90-day prescriptions in Mexico for certain higher-cost medications.
“The prescription drugs received in Mexico are the same quality and from the same manufacturer as those sold in the US,” said Travis Tolley, Clinical Management Director at PEHP Health and Benefits, in a news release. “The difference is the price you pay. For example, a 90-day supply for the average cost of an eligible drug in the US is over $4,500 per month and is 40-60% less in Mexico. The substantial savings allow us to reward our members for seeking lower-cost options.”
Participants in the program receive round-trip airfare from Utah to San
Diego for themselves and a companion, followed by transportation to a clinic in
Tijuana where their prescriptions are filled. They also can receive a taxable
$500 cash bonus for each trip—up to four trips/year. The airfare from Salt Lake
City to San Diego typically costs around $300.
In 2018, Utah passed the “Health Insurance Right to Shop Amendments” bill (H.B. 19), which requires PEHP to offer incentives and a savings reward program to members who seek out and utilize low-cost options for healthcare. State Representative Norman Thurston (above right) sponsored the bill. “Why wouldn’t we pay $300 to go to San Diego, drive across to Mexico, and save the system tens of thousands of dollars? If it can be done safely, we should be all over that,” he told Becker’s Hospital Review. (Photo copyright: Daily Herald.)
PEHP, which covers 160,000 public employees and family
members, offers the pharmacy tourism program for 13 specific medications where
a vast disparity in cost exists between the US and Mexico.
The drugs that qualify for the program along with the most
common illnesses they treat are:
One of the more expensive drugs on the list, Avonex, costs
approximately $6,700 for a month’s supply in the US compared to only about
$2,200 at the contracted clinic in Tijuana. That’s a savings of approximately
$13,500 for a three-month supply, which compensates for the program’s $500 cash
reward and transportation costs.
Not the First Time
PEHP Tried Medical Tourism
PEHP previously offered free
airfare to members willing to fly to other countries for medical procedures and
prescriptions. However, without the cash incentives, participation was low. The
health plan hopes the lure of $500 per trip will increase participation rate.
UnitedHealthcare (UHC) also is experimenting with ways to lower prescription drug costs. Last year, they introduced My ScriptRewards. The program incentivizes members to opt for less expensive medications. Participants in this program receive up to $500 in prepaid debit cards to help defray their medical costs.
Currently, My ScriptRewards can only be used for select antiviral medications (Cimduo plus Isentress or Cimduo plus Tivicay) to treat human immunodeficiency virus (HIV). And, it’s only available to UHC commercial plan members who are covered by group plans. However, UHC plans to expand the program to include other high-cost specialty medications in the future.
According to the Centers for Disease Control and Prevention (CDC), prescription medications account for 9.8% of national health expenditures. And in 2017, Quintiles and IMS Health, Inc. (now IQVIA), a company that compiles data for the pharmaceutical industry, estimated that prescription spending in the US will reach an annual cost of $580-$610 billion by 2021.
And, with prescription costs soaring, it’s likely insurance
providers will continue to seek new ways to curtail costs. In an era when many medical
laboratory companies are charging sky-high prices for their proprietary tests
and test panels, might “clinical laboratory tourism” be the next trend to
emerge?
Contrary to CMS and Joint Commission programs implemented in 2017 to reduce them, incidents of hospital-acquired infections have risen for the past few years
Nevertheless, a recent Leapfrog Group report indicates hospitals are finding it increasingly difficult to remove infections all together. This has many healthcare leaders concerned.
The report, which was analyzed by Castlight Health, states that the number of hospitals reporting zero infections has declined significantly since 2015, according to a news release. According to the Leapfrog Group’s report:
Two million people acquire HAIs every year;
90,000 people die annually from HAIs;
HAI costs range from $1,000 to $50,000 depending on the infection.
Hospitals spend $28 to $45 billion annually on HAI costs, Healthcare Finance reported.
“I think it’s far too easy to let something slip, so it’s clear that there really needs to be a renewed focus on getting back to zero. We do still see some hospitals that are getting to zero, so it’s clearly possible,” Erica Mobley (above), Leapfrog Group’s Director of Operations, told Fierce Healthcare. (Photo copyright: LinkedIn.)
Regressing Instead of Progressing Toward Total HAI Elimination
Leapfrog Group’s report is based on 2017 hospital survey data submitted by 2,000 providers. The data indicates that in just two years the number of hospitals reporting zero HAIs dropped by up to 50%. The reported HAIs include:
Central line-associated bloodstream infections (CLABSI) occurring in Intensive Care and other units: 12.7% of hospitals reporting zero CLABSI infections in 2017, down from 25% in 2015;
The remaining infection measures studied by Leapfrog Group had less dramatic decreases over the same time period, according to Fierce Healthcare. Nevertheless, they are significant. They include:
Surgical site infections (SSI) following colon surgery: 19% zero infections compared to 23% previously;
Clostridium difficile (C. difficile) inpatient infections: 3% zero inpatient infections in 2017, compared to 5% in 2015.
Joint Commission Studies Antimicrobial Program Progress
Hospitals have revised their antimicrobial programs, which originally operated on a “top-down” structure, to programs that include clinicians from throughout entire provider organizations;
Health information technology (HIT) can enable real-time opportunities to launch antimicrobial therapy and treat patients; and,
Some barriers exist in getting resources to integrate technology and analyze data.
“These programs used expansion of personnel to amplify the antimicrobial stewardship programs’ impact and integrated IT resources into daily workflow to improve efficiency,” the researchers wrote. “Hospital antimicrobial stewardship programs can reduce inappropriate antimicrobial use, length of stay, C. difficile infection, rates of resistant infections, and cost.”
What Do CMS and Joint Commission Expect?
According to Contagion, while the Joint Commission program is part of medication management, CMS places its requirements for the antimicrobial stewardship program under “infection prevention.”
CMS requirements for an antimicrobial stewardship program include:
Developing antimicrobial stewardship program policies and procedures;
Implementing hospital-wide efforts;
Involving antimicrobial stakeholders for focus on antimicrobial use and bacterial resistance;
Setting evidence-based antimicrobial use goals; and,
Reducing effects of antimicrobial use in areas of C. difficile infections and antibiotic resistance.
Leapfrog Group’s data about fewer hospitals reporting zero infections offers opportunities for hospital laboratory microbiology professionals to get involved with hospital-wide antimicrobial program teams and processes and help their hospitals progress back to zero HAIs. Clinical laboratories, both hospital-based and independent, also have opportunities to contribute to improving the antimicrobial stewardship efforts of the physicians who refer them specimens.
CDC reports more than 93-million US adults are obese, and health issues related to obesity include heart disease, stroke, type 2 diabetes, and cancers
In recent years, the role of the human microbiome in weight loss or weight gain has been studied by different research groups. There is keen interest in this subject because of the high rates of obesity, and diagnostic companies know that development of a clinical laboratory test that could assess how an individual’s microbiome affects his/her weight would be a high-demand test.
This is true of a study published this year in Mayo Clinic Proceedings. Researchers at Mayo Clinic looked at obese patients who were in an active lifestyle intervention program designed to help them lose weight. It was determined that gut microbiota can have a role in both hindering weight loss and supporting weight loss.
Gut Microbiota More Complicated than Previously Thought
The Mayo researchers determined “an increased abundance of Phascolarctobacterium was associated with [successful weight loss]. In contrast, an increased abundance of Dialister and of genes encoding gut microbial carbohydrate-active enzymes was associated with failure to [lose] body weight. A gut microbiota with increased capability for carbohydrate metabolism appears to be associated with decreased weight loss in overweight and obese patients undergoing a lifestyle intervention program.”
How do bacteria impede weight loss? Vandana Nehra, MD, Mayo Clinic Gastroenterologist and co-senior author of the study, explained in a news release.
“Gut bacteria have the capacity to break down complex food particles, which provides us with additional energy. And this is normally is good for us,” she says. “However, for some individuals trying to lose weight, this process may become a hindrance.”
Put another away: people who more effectively metabolized carbohydrates were the ones who struggled to drop the pounds, New Atlas pointed out.
Vandana Nehra, MD (left), and Purna Kashyap, MBBS (right), are Mayo Clinic Gastroenterologists and co-senior authors of the Mayo study. “While we need to replicate these findings in a bigger study, we now have an important direction to pursue in terms of potentially providing more individualized strategies for people who struggle with obesity,” Nehra noted in the news release. Thus, precision medicine therapy for obese individuals could be based on Mayo Clinic’s research. (Photo copyright: Mayo Clinic.)
Mayo Study Provides Clues to Microbiota Potential in Weight Loss
The Mayo researchers wanted to know how gut bacteria behave in people who are trying to lose weight.
They recruited 26 people, ranging in age from 18 to 65, from the Mayo Clinic Obesity Treatment Research Program. Fecal stool samples, for researchers’ analysis, were collected from participants at the start of the three-month study period and at the end. The definition of successful weight loss was at least 5% of body weight.
Researchers found the following, according Live Science:
2 lbs. lost, on average, among all participants;
Nine people were successful, losing an average of 17.4 lbs.;
17 people did not meet the goal, losing on average just 3.3 lbs.; and,
More gut bacterial genes that break down carbohydrates were found in stool samples of the unsuccessful weight loss group, as compared to the successful dieters.
The researchers concluded that “An increased abundance of microbial genes encoding carbohydrate-active enzyme pathways and a decreased abundance of Phascolarctobacterium in the gut microbiota of obese and overweight individuals are associated with failure to lose at least 5% weight following a 3-month comprehensive lifestyle intervention program.”
Purna Kashyap, MBBS, Mayo Clinic Gastroenterologist and co-senior author of the study, told Live Science, “The study suggests there is a need to take the microbiome into account in clinical studies (on weight loss), and it also provides an important direction to pursue in terms of providing individualized care in obesity.” The very basis of precision medicine.
Future Weight-Loss Plans Based on Patient’s Microbiota
The Mayo Clinic researchers acknowledged the small sample size and need for more studies with larger samples over a longer time period. They also noted in their paper that Dialister has been associated with oral infections, such as gingivitis, and its role in energy expenditure and metabolism is unclear.
Still, the study suggests that it may soon be possible to give people individualized weight loss plans based on their gut bacteria. Clinical laboratory professionals and pathologists will want to stay abreast of follow-up studies and replication of findings by other research teams. A future medical laboratory test to analyze patients’ microbiomes could help obese people worldwide as well as lab business volume.