Lack of regular clinical laboratory screenings in this age group at least partially to blame, researchers say
While cervical cancer rates have seen a 50-year decline overall, that trend is shifting among 30- to 40 year-olds who have experienced a near 2% increase from 2012-2019. This finding comes from a 2024 American Cancer Society (ACS) report that is eyeing the timeline of the human papillomavirus (HPV) vaccines and the lack of clinical laboratory cancer screenings as possible contributors to this new trend.
Though a 2% increase is significant, the study, which was published in CA: ACancer Journal for Clinicians, titled “Cancer Statistics, 2024,” noted that these cancers were “mostly early, curable tumors,” epidemiologist Ahmedin Jemal DVM, PhD, Senior Vice President Surveillance and Health Equity Science at ACS, and senior author of the new report, told NBC News.
To understand how the increase in cancer rates impacts this age group, consider the numbers: “About 13,800 American women are diagnosed with cervical cancer each year and 4,360 die from the disease,” NBC reported.
US vaccination programs for youths have lagged behind nations that have embraced HPV vaccination to positive results.
Australia, for example, has vaccinated a high proportion of its youth since the vaccine was first released in 2006. In 2023, the nation created its National Strategy for the Elimination of Cervical Cancer in Australia program and expects cervical cancer to be fully eliminated there by 2035.
For lab professionals, this demonstrates how new technologies like the HPV test and vaccine can alter how individuals are screened for diseases, and how vaccines can reduce and even eliminate diseases that were once common.
“We need to make sure we are not forgetting about that generation that was a little too old for HPV vaccination,” Jennifer Spencer, PhD (above), Assistant Professor, Department of Population Health and Department Internal Medicine, Dell Medical School, University of Texas at Austin, told NBC News. “The onus is on the healthcare system to think about who is slipping through the cracks,” she added. Lack of clinical laboratory screenings among the 30-40 age group may be contributing to the increase in cervical cancer rates. (Photo copyright: Dell Medical School.)
Lack of Clinical Laboratory Screenings
Research points to a lag in cervical cancer screenings as a possible cause for the recent rise in cases. Timely screening allows doctors to both identify and remove any worrisome lesions before they become cancerous, Jennifer Spencer, PhD, Assistant Professor of the Department of Population Health, Dell Medical School, University of Texas at Austin, told NBC News.
Screenings for women ages 21-65 have fallen 15% since 2000, according to data from the National Cancer Institute. Also, more than half of women with cervical cancer have “either never been screened or haven’t been screened in the past five years, according to the Centers for Disease Control and Prevention,” NBC reported.
The US Preventative Services Task Force recommends that women 21-29 years of age should receive Pap smears every three years. Women 30-65 years of age should do the same, or every five years with an HPV test or combo test.
Despite a decrease in cervical cancer, 29% of women in their 20s are overdue to get screening, NBC noted. This was the age group most likely to be lagging on getting screened. Spencer says that this delay in screening could explain the resulting increase in cervical cancer among the 30-40 age group.
Causes for Lack in Screenings
Regardless of age group, women who were uninsured, in a rural area, non-white, or identifying as lesbian, bisexual, or gay were also more likely to be overdue on screenings, according to Spencer’s study.
In addition, women who just moved to the United States may have missed their screenings, thus increasing risk, epidemiologist Nicholas Wentzensen, MD, PhD, Deputy Director, Senior Investigator, and Head of the Clinical Epidemiology Unit at the National Cancer Institute, told NBCNews.
Additionally, Spencer found in her research that confusion exists by both patients and doctors on when cervical screening should take place. Some participants in her study did not have screening recommended by their doctors, while others simply did not recognize it was necessary.
“When women in one of Spencer’s studies were asked why they hadn’t been screened recently, they commonly said that they didn’t know they needed to be screened or that a health provider hadn’t recommended it. Only 1% [of] women ages 21 to 29 said they had skipped screening because they had received the HPV shot,” NBC News reported.
A 2022 Journal of American Medicine (JAMA) report also looked at screenings as a possible cause. Those researchers found that “only 73% of women with abnormal screening results received follow-up care,” NBC reported.
“If the increase (in cases) is real, it could be a result of missed screening opportunities at earlier ages, as suggested by the increase in squamous cell carcinoma and localized disease. It may also stem from a decrease in screening at younger ages,” the JAMA study authors wrote.
HPV Vaccine and Cervical Cancer Prevention
The HPV vaccine is another important area of research to be considered. Approved in 2006, HPV vaccines were beneficial because HPV “causes six types of cancer, including cervical cancer,” NBC reported.
Women in their early 20s at that time were the first generation to benefit from HPV vaccines, NBC noted. It may be that they continue to benefit in a decrease in cervical cancer among their cohort.
Countries that have emphasized HPV vaccines and stringent screenings in their cancer prevention efforts are reaping the benefits of that policy.
Though cancer screening and the HPV vaccine are important first steps women should take to prevent cervical cancer, follow-through clinical laboratory testing and diagnosis is crucial, Spencer added. This would include additional testing and treatment for any abnormal results of the cancer screening.
However, according to Spencer, “only 73% of women with abnormal screening results received follow-up care,” NBC reported.
Healthcare policymakers today are emphasizing the need for providers to identify and close gaps in care as a way to improve patient outcomes and help control the cost of care. Women who are overdue for a cervical cancer screening test—whether an HPV test or Pap smear—have this care gap. This creates an opportunity for clinical labs to add value.
Clinical laboratories could be helpful during this period by looking at patient files to note which patients are overdue for screenings and then alerting their doctors. Medical labs also could work directly with doctors to establish a program to reach out to patients. Labs would thus be adding value as well as benefitting patients.
Trifecta of forces at work that will affect the clinical laboratory and pathology industries have been described as a ‘perfect storm’ requiring lab and practice managers to be well informed
Digital pathology, artificial intelligence (AI) in healthcare, and the perfect storm of changing federal regulations, took centerstage at the 29th Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management in New Orleans this week, where more than 1,000 clinical laboratory and pathology leaders convened over three days.
This was the largest number of people ever onsite for what has become the world’s largest event focused exclusively on lab management topics and solutions. Perhaps the highlight of the week was the federal Food and Drug Administration’s (FDA’s) announcement of its final rule on Laboratory Developed Tests (LDTs). Overall, the conference featured more than 120 speakers, many of them national thought leaders on the topic of clinical lab and pathology management. More than 65% of the audience onsite were executive level lab managers.
“The level of interest in the annual Executive War College is testimony to the ongoing need for dynamic, engaging, and highly relevant conference events,” said Robert Michel (above), Editor-in-Chief of Dark Daily and its sister publication The Dark Report, and founder of the Executive War College. “These in-person gatherings present great opportunities for clinical laboratory and pathology managers and leaders to network and speak with people they otherwise might not meet.” (Photo copyright: Dark Intelligence Group.)
Demonstrating Clinical Value
For those who missed the action onsite, the following is a synopsis of the highlights this week.
Lâle White, Executive Chair and CEO of XiFin, spoke about the future of clinical laboratory testing and the factors reshaping the industry. There are multiple dynamics impacting healthcare economics and outcomes—namely rising costs, decreasing reimbursements, and the move to a more consumer-focused healthcare. But it is up to labs, she said, to ensure their services are not simply viewed as a commodity.
“Laboratory diagnostics have the potential to change the economics of healthcare by really gaining efficiencies,” she noted. “And it’s up to labs to demonstrate clinical value by helping physicians manage two key diagnostic decision points—what tests to order, and what to do with the results.”
But even as labs find ways to increase the value offered to clinicians, there are other disruptive factors in play. Consumer-oriented tech companies such as Google, Apple, and Amazon are democratizing access to patient data in unforeseen ways, and Medicare Advantage plans are changing the way claims are processed and paid.
Clinical labs are fundamental components of the public health infrastructure. So, the CDC plans on focusing on delivering high-quality laboratory science, supported by reliable diagnostics and informatics for disease outbreaks and exposures, and engaging with public and private sector partners.
The history of MolDX and Z-Codes were the topics discussed by Gabriel Bien-Willner, MD, PhD, Chief Medical Officer for healthcare claims and transaction processing company Palmetto GBA. Molecular testing is highly complex, and the lack of well-defined billing codes and standardization makes it difficult to know if a given test is reasonable and necessary.
Z-Codes were established to clarify what molecular testing was performed—and why—prompting payers to require both Z-Codes and Current Procedural Terminology (CPT) codes when processing molecular test claims. Medicare’s MolDX program further streamlines the claims process by utilizing expertise in the molecular diagnostics space to help payers develop coverage policies and reimbursement for these tests.
FDA Final Rule on LDT Regulation
Timothy Stenzel, MD, PhD, CEO of Grey Haven Consulting and former director of the FDA’s Office of In Vitro Diagnostics reviewed the latest updates from the FDA’s Final Rule on LDT (laboratory developed test) regulation. Prior to the FDA releasing its final rule, some experts suggested that the new regulations could result in up to 90% of labs discontinuing their LDT programs, impacting innovation, and patient care.
However, the final rule on LDTs is very different from the original proposed rule which created controversy. The final rule actually lowers the regulatory burden to the point that some labs may not have to submit their LDTs at all. The FDA is reviewing dozens of multi-cancer detection assays, some of which have launched clinically as LDTs. The agency is likely to approve those that accurately detect cancers for which there is no formal screening program.
Stenzel explained the FDA’s plan to down-classify most in vitro diagnostic tests, changing them from Class III to Class II, and exempting more than 1,000 assays from FDA review. He also discussed the highlights of the Quality Management System Regulation (QMSR). Launched in January, the QMSR bought FDA requirements in line with ISO 13485, making compliance easier for medical device manufacturers and test developers working internationally.
Looming Perfect Storm of Regulatory Changes
To close out Day 1, Michel took to the stage again with a warning to clinical laboratories about the looming “Perfect Storm” trifecta—the final FDA ruling on LDTs, Z-Code requirements for genetic testing, and updates to CLIA ’92 that could result in patient data being considered a specimen.
Laboratory leaders must think strategically if their labs are to survive the fallout, because the financial stress felt by labs in recent years will only be exacerbated by macroeconomic trends such as:
Staff shortages,
Rising costs,
Decreasing and delayed reimbursements, and
Tightening supply chains.
Lab administrators looking for ways to remain profitable and prosperous should look beyond the transactional Clinical Lab 1.0 fee-for-service model and adopt Clinical Lab 2.0, which embraces HEDIS (Healthcare Effectiveness Data and Information Set) scores and STAR ratings to offer more value to Medicare Advantage and other payers.
Wednesday’s General Session agenda was packed with information about the rise of artificial intelligence, big data, and precision medicine in healthcare. Taking centerstage on the program’s final day was Michael Simpson, President and CEO of Clinisys. Simpson gave a global perspective on healthcare data as the new driver of innovation in diagnostics and patient care.
“The timing of EWC with the release of this policy couldn’t be better,” CEO and founder of Momentum ConsultingValerie Palmieri told Dark Daily in an interview at Monday night’s opening reception. “It’s a great conference to not only catch up with colleagues but really hear and have those difficult discussions about where we are today, where we’re going, and where we need to be.”
Final LDT rule ‘radically’ different than draft
Tim Stenzel, MD, PhD, former director of the FDA’s Office of In Vitro Diagnostics called the finalized rule “radically different” from the proposed rule. In some ways it is less complex: “The bar is lower,” he said, noting that he was voicing his personal views and not those of the federal agency. “I was convinced that there would be lawsuits, but I’m now not sure if that’s advisable.”
Still, laboratory teams will have to parse the more than 500-page document to determine how the final rule relates to their specific circumstances. After that, it won’t be as challenging, Stenzel said.
His advice: First, read the rule. Second, reach out to FDA for help—he’s sure, he said, that the office is geared up to respond to a “ton of questions” about the implications for individual labs and are standing by to answer emails from labs. And, he added in a discussion session, emailing the agency is free.
The final rule will be in force 60 days after it’s published. Stenzel provided a timeline for some of the milestones:
1 Year: Comply with MD(AE) reporting and reporting of corrections and removals.
2 Years: Comply with labeling, registration and listing, and investigational use requirements.
3 Years: QS records and, in some cases, design controls and purchasing controls.
3.5 Years: Comply with high risk (class III) premarket review requirements.
4 Years: Comply with moderate and low-risk premarket review requirements.
Executive Chair and CEO of XiFin, Inc.Lâle White welcomed the audience with a morning keynote entitled “Big Changes in Healthcare” on new regulations and diagnostics players poised to reshape lab testing.
The diagnostics business is in constant flux, she noted, from payer requirements to greater regulatory and compliance burdens on labs. Other factors include the growing senior population and increasingly complex health conditions, rising costs throughout the healthcare ecosystem, falling funding and reimbursement, and staffing shortages.
As for the economic challenges, consumers are increasingly making decisions based on cost, convenience and quality. The population is shifting to Medicare advantage, which is more cost effective. But changes to the star ratings system will mean lower pay for payer organizations. Those companies will, in turn, mitigate their losses by making changes to pre-authorizations and tightening denials, even for clean claims.
Still, White said, more money isn’t the answer.
White urged the audience to use technology, including artificial intelligence and advances in genetic testing, to manage these and other industry changes.
“We need to optimize the tests we order,” she said. “And if we did that, lab diagnostics really has the potential to change the economics of health and improve outcomes.”
The FDA, Stenzel added, is “very interested” in stimulating innovation, building on the laboratory industry’s success in responding swiftly to the COVID pandemic and outbreaks of Monkey Pox, for example.
He shared lessons learned from recent public health emergencies, talked about CDC’s efforts to engage with clinical labs to improve future public health readiness and response and provided an overview of the CDC’s first laboratory-specific center.
“Laboratories are fundamental to public health,” he said. The industry is on the “front lines” when it comes to identifying threats, responding to them, and preparing for future responses.
Robert Michel, Editor-in-Chief of The Dark Report wrapped up the day’s regulatory discussions with a general session on the “regulatory trifecta” that includes the LDT final rule, CLIA regulations, and private payers’ policies for genetic claims.
The Office of Management and Budget (OMB) concluded its review of the final rule on April 22. Former FDA commissioner Scott Gottlieb, MD, and other regulatory experts expect the White House to send the final rule to Congress as early as late April and no later than May 22.
On Tuesday morning, Lâle White, executive chair and CEO of San Diego’s XiFin, Inc., will present a keynote on new regulations and diagnostics players that are “poised to reshape lab testing.” Her presentation is followed by a general session on Clinical Laboratory Improvement Amendments (CLIA) regulations featuring Salerno Reynolds, PhD., acting director at the U.S. Centers for Disease Control and Prevention (CDC) Center for Laboratory Systems and Response.
Robert Michel, Editor-in-Chief of The Dark Report will wrap day one with a general session on the regulatory trifecta coming soon to all labs, from LDT to CLIA to private payers’ policies for genetic claims.
Innovation in the spotlight
“It’s a rich mix of expert speakers, lab leaders who are doing innovative things in their own organizations, along with the consultants and the lab vendors who are pushing the front edge of laboratory management, operations, and clinical service delivery,” says Michel, who each year creates the agenda for EWC.
Several sessions, master classes, and speakers will look to the future with discussions about how healthcare data drives innovations in diagnostics and patient care, digital pathology adoption around the world, and hot topics such as artificial intelligence (AI), big data and precision medicine.
Panels offer a variety of viewpoints
“One valuable benefit of participating at the Executive War College is the various panel discussions,” Michel says. “Each panel brings together national experts in a specific area of the laboratory profession. As an example, our lab legal panel this year brings together four prominent and experienced attorneys who share opinions, insights, and commentary about relevant issues in compliance, regulations, and contractual issues with health plans and others.”
This allows attendees to experience a breadth of opinions from multiple respected experts in this area, he adds.
For example, a digital pathology panel will bring together representatives from labs, service providers, and the consultants that are helping labs implement digital pathology. The session will be especially helpful to labs that are deciding when to acquire digital pathology tools and how to deploy them effectively to improve diagnostic accuracy, Michel says.
And a managed care panel will feature executives from some of the nation’s biggest health plans—the ones that sit on the other side of the table from labs—to provide insights and guidance on how labs can work more effectively with them.
Networking opportunities abound
The event is about much more than politics and policy, however. There’s also a distinct social aspect.
“Everyone is welcome, and everyone appreciates the camaraderie, so don’t be shy about going up and introducing yourself to someone. The quality of the crowd is top-notch, yet I’ve always experienced a willingness for those of us who have been to this rodeo to always be welcoming,” she notes.
Michel agrees. “One of the special benefits of participation at the EWC is the superb networking interactions and collaboration that takes place,” he says.
“From the first moments that attendees walk into our opening reception on Monday night until the close of the optional workshops on Thursday, one can see a rich exchange happening amongst circles of attendees. Introductions are being made. Connections are developing into business opportunities. The sum of an attendee’s experience at the Executive War College is to gain as much knowledge from the networking and collaboration as they do from the sessions.”
Phages are miniscule, tripod-looking viruses that are genetically programmed to locate, attack, and eradicate a specific kind of pathogen. These microscopic creatures have saved lives and are being touted as a potential solution to superbugs, which are strains of bacteria, viruses, parasites, and fungi that are resistant to most antibiotics and other treatments utilized to counteract infections.
“These multi-drug-resistant superbugs can cause chronic infections in individuals for months to years to sometimes decades,” Dwayne Roach, PhD, Assistant Professor of Bacteriophages, Infectious Disease, and Immunology at SDSU told CNN. “It’s ridiculous just how virulent some of these bacteria get over time.”
Labs across the country are conducting research on phages in eradicating superbugs. Roach’s lab is currently probing the body’s immune response to phages and developing purification techniques to prepare phage samples for intravenous use in patients.
“There are a lot of approaches right now that are happening in parallel,” said Dwayne Roach, PhD (above), Assistant Professor of Bacteriophages, Infectious Disease, and Immunology at San Diego State University (SDSU), in a CNN interview. “Do we engineer phages? Do we make a phage cocktail, and then how big is the cocktail? Is it two phages or 12 phages? Should phages be inhaled, applied topically, or injected intravenously? There’s a lot of work underway on exactly how to best do this.” Clinical laboratories that test for bacterial infections may play a key role in diagnosis and treatment involving bacteriophages. (Photo copyright: San Diego State University.)
Building Libraries of Phages
When certain a bacterial species or its genotypes needs to be annihilated, a collection of phages can be created to attack it via methods that enter and weaken the bacterial cell. The bacteria will attempt to counter the intrusion by employing evasive actions, such as shedding outer skins to eliminate the docking ports utilized by the phages. These maneuvers can cause the bacteria to lose their antibiotic resistance, making them vulnerable to destruction.
Some research labs are developing libraries of phages, accumulating strains found in nature in prime breeding grounds for bacteria to locate the correct phage for a particular infection. Other labs, however, are speeding up the process by producing phages in the lab.
“Rather than just sourcing new phages from the environment, we have a bioreactor that in real time creates billions upon billions of phages,” Anthony Maresso, PhD, Associate Professor at Baylor College of Medicine in Houston told CNN. “Most of those phages won’t be active against the drug-resistant bacteria, but at some point, there will be a rare variant that has been trained, so to speak, to attack the resistant bacteria, and we’ll add that to our arsenal. It’s a next-generation approach on phage libraries.”
For the Baylor study, 12 patients were treated with phages customized to each individual’s unique bacterial profile. The antibiotic-resistant bacteria were exterminated in five of the patients, while several others showed improvement.
Clinical trials are currently being executed to test the effectiveness of phages against a variety of chronic health conditions, including:
Using a phage cocktail could be used to treat a superbug outbreak in real time, while preventing a patient from a future infection of the same superbug.
“The issue is that when patients have infections with these drug-resistant bacteria, they can still carry that organism in or on their bodies even after treatment,” Maroya Walters, PhD, epidemiologist at the federal Centers for Disease Control and Prevention (CDC) told CNN.
“They don’t show any signs or symptoms of illness, but they can get infections again, and they can also transmit the bacteria to other people,” she added.
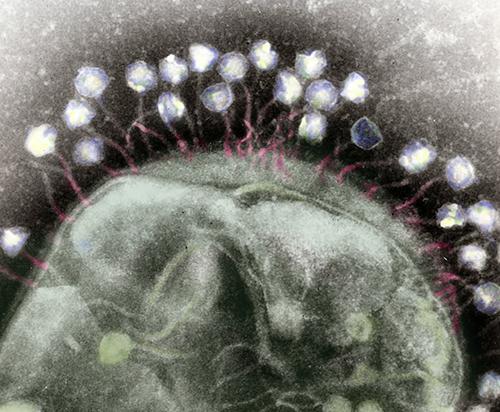
The colorized transmission electron micrograph above shows numerous phages attached to a bacterial cell wall. Phages are known for their unique structures, which resemble a cross between NASA’s Apollo lunar lander and an arthropod. (Caption and photo copyright: Berkeley Lab.)
More Studies are Needed
According to CDC data, more than 2.8 million antimicrobial-resistant (AMR) infections occur annually in the United States. More than 35,000 people in the country will die as a result of these infections.
In addition, AMR infections are a huge global threat, associated with nearly five million deaths worldwide in 2019. Resistant infections can be extremely difficult and sometimes impossible to treat.
More research is needed before phages can be used clinically to treat superbugs. But if phages prove to be useful in fighting antibiotic-resistant bacteria, microbiologists and their clinical laboratories may soon have new tools to help protect patients from these deadly pathogens.