Researchers used CRISPR-based assays to develop new clinical laboratory point-of-care blood test which boasts accuracy, affordability, and accessibility
According to UPI, the test can “distinguish between influenza A and influenza B—the two main types of seasonal flu—as well as identifying more virulent strains like H1N1 and H3N2.”
Many research teams are working to develop paper-based diagnostic screening tests because of their lower cost to produce and usefulness in remote locations. Should this near-patient point-of-care test become clinically viable, it could mean shorter times to answer, enabling speedier diagnoses and earlier start of treatment.
It also means patient specimens do not have to be transported to a clinical laboratory for testing. And reduced cost per test makes it possible to test more people. This serves the public health aspect of monitoring outbreaks of influenza and other diseases and gives hope for improved treatment outcomes.
“Being able to tease apart what strain or subtype of influenza is infecting a patient has repercussions both for treating them and public health interventions, said Jon Arizti Sanz, PhD, co-lead study author and postdoctoral researcher at the Broad Institute of Harvard and MIT, in a Broad Institute news release.
“Ultimately, we hope these tests will be as simple as rapid antigen tests, and they’ll still have the specificity and performance of a nucleic acid test that would normally be done in a laboratory setting,” Cameron A. Myhrvold, PhD (above), Assistant Professor of Molecular Biology at Princeton University in New Jersey, told CIDRAP. Influenza tests that can be performed at the point of care and in remote locations may reduce the number of screening tests performed by clinical laboratories. (Photo copyright: Michael James Butts/Hertz Foundation.)
Her team developed their tests using Streamlined Highlighting of Infections to Navigate Epidemics (SHINE), “a clustered regularly interspaced short palindromic repeats (CRISPR)-based RNA detection platform,” the researchers wrote in their Journal of Molecular Diagnostics paper.
“SHINE has a runtime of 90 minutes, can be used at room temperature and only requires an inexpensive heat block to heat the reaction. The SHINE technology has previously been used to identify SARS-CoV-2 and later to distinguish between the Delta and Omicron variants,” Bioanalysis Zone reported.
“The test uses genetically engineered enzymes to identify specific sequences of viral RNA in samples,” the researchers told UPI. Originally designed to detect COVID-19, the team adapted the technology to detect influenza in 2022 “with the aim of creating a screening tool that could be used in the field or in clinics rather than hospitals or high-tech diagnostic labs,” they said.
Influenza A and B as well as H1N1 and H3N2 subtypes were the targets of the four SHINE assays. “When tested on clinical samples, these optimized assays achieved 100% concordance with quantitative RT-PCR. Duplex Cas12a/Cas13a SHINE assays were also developed to detect two targets simultaneously,” the researchers wrote in their paper.
The team used “20 nasal swabs from people with flu-like symptoms during the 2020-2021 flu season, nasal fluid from healthy people as the control, and 2016-2021 influenza sequences downloaded from the National Center for Biotechnology Information Influenza (NICB) database. They compared the results with those from quantitative reverse transcription-polymerase chain reaction (RT-PCR) tests,” CIDRAP reported.
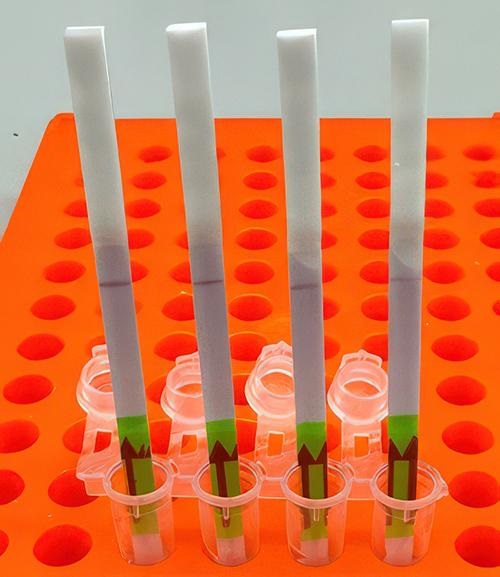
The original 2020 test (shown above) takes 90 minutes to develop at room temperature. The test developers aim to drop this down to 15 minutes. In comparison, typical polymerase chain reaction (PCR) testing requires medical laboratories to have specialized equipment, trained staff, and prolonged processing times, the Broad Institute news release notes. (Photo copyright: Broad Institute.)
Implications of the New Tests
The ease of the new tests is an important development since approximately only 1% of individuals who come down with the flu see doctors for testing, according to the news release. And researchers had this in mind, looking at speed, accuracy, and affordability as a means to “improve outbreak response and infection care around the world,” UPI reported.
There are great benefits to strain differentiation that be achieved with the new test. Doctors are hopeful the test will help dial in the best treatment plans for patients since some strains are resistant to the antiviral medication oseltamivir (Tamiflu), UPI noted. This is significant since Tamiflu “is a common antiviral,” said Sanz in the Broad Institute news release.
“These assays have the potential to expand influenza detection outside of clinical laboratories for enhanced influenza diagnosis and surveillance,” the Journal of Molecular Diagnostics paper noted. This allows for more strategic treatment planning.
“Using a paper strip readout instead of expensive fluorescence machinery is a big advancement, not only in terms of clinical care but also for epidemiological surveillance purposes,” said Ben Zhang, an MD candidate in the Health Sciences and Technology at Harvard and co-first author of the study, in the Broad Institute news release.
Future Plans for Tests
“With further development, the test strip could be reprogrammed to distinguish between SARS-CoV-2 and flu and recognize swine flu and avian flu, including the H5N1 subtype currently causing an outbreak in US dairy cattle,” the study authors told CIDRAP.
The team is also looking at ways to help prevent H5N1 from crossing into human contamination, Sanz told UPI.
The new Princeton/MIT/Harvard tests echo the trend to bring in affordability and ease-of-use with accurate results as an end goal. Faster results mean the best treatments for each person can start sooner and may render the transport of specimens to a clinical laboratory as a second step unnecessary.
As research teams work to develop paper-based viral tests for their plethora of benefits, clinical laboratories will want to pay close attention to this development as it can have a big implication on assisting with future outbreaks.
Additional research is needed before these tests are going to be commonplace in homes worldwide, but this first step brings inspiration and hope of what’s to come.
Another study in the United Kingdom that also used genomic analysis to understand drug-resistant Shigella produced findings that may be useful for microbiologists and medical laboratory scientists
From the onset of an infectious disease outbreak, public health officials, microbiologists, and clinical laboratory managers find it valuable to trace the origin of the spread back to the “index case” or “patient zero”—the first documented patient in the disease epidemic. Given the decreased cost of genomic analysis and improved accuracy of gene sequencing, infectious disease researchers are finding that task easier and faster than ever.
One recent example is a genomic study conducted at University of Washington (UW) in Seattle that enabled researchers to “retrace” the origin and spread of a “multidrug-resistant Shigellosis outbreak” from 2017 to 2022. “The aim of the study was to better understand the community transmission of Shigella and spread of antimicrobial resistance in our population, and to treat these multi-drug resistant infections more effectively,” the UW scientists stated in a new release.
Shigellosis (aka, bacillary dysentery) is a highly contagious disease of the intestines that can lead to hospitalization. Symptoms include fever, stomach cramps, diarrhea, dysentery, and dehydration.
“Additional analysis of the gut pathogen and its transmission patterns helped direct approaches to testing, treatment, and public health responses,” the UW news release states.
Usually prevalent in countries with public health and sanitation limitations, the “opportunistic” Shigella pathogen is now being seen in high-income countries as well, UW reported.
“You can’t really expect an infectious disease to remain confined to a specific at-risk population. [Shigella infections are] very much an emerging threat and something where our public health tools and therapeutic tools have significant limitations,” infectious disease specialist Ferric Fang, MD (above) told CIDRAP News. Fang is a UW professor of Microbiology and Clinical Laboratory Medicine and a corresponding author of the UW study. (Photo copyright: University of Washington.)
Generally, Shigella infects children, travelers, and men who have sex with men (MSM), the CDC noted.
The UW researchers were motivated to study Shigella when they noticed an uptick in drug-resistant shigellosis cases in Seattle’s homeless population in 2020 at the beginning of the COVID-19 pandemic, Center for Infectious Disease Research and Policy News (CIDRAP News) reported.
“Especially during the pandemic, a lot of public facilities were closed that homeless people were used to using,” infectious disease specialist Ferric Fang, MD, told CIDRAP News. Fang is Professor of Microbiology and Laboratory Medicine at University of Washington and corresponding author of the UW study.
The researchers studied 171 cases of Shigella identified from 2017 to 2022 by clinical laboratories at Harborview Medical Center and UW Medical Center in Seattle. According to CIDRAP News, the UW researchers found that:
46% were men who have sex with men (MSM).
51% were people experiencing homelessness (PEH).
Fifty-six patients were admitted to the hospital, with eight to an intensive care unit.
51% of isolates were multi-drug resistant (MDR).
Whole-Genome Sequencing Reveals Origin
The UW scientists characterized the stool samples of Shigella isolates by species identification, phenotypic susceptibility testing, and whole-genome sequencing, according to their Lancet Infectious Diseases paper. The paper also noted that 143 patients received antimicrobial therapy, and 70% of them benefited from the treatment for the Shigella infection.
Whole-genome sequencing revealed that two strains of Shigella (S. flexneri and S. sonnei) appeared first in Seattle’s MSM population before infecting the PEM population.
The genomic analysis found the outbreak of drug-resistant Shigella had international links as well, according to CIDRAP News:
One S. flexneri isolate was associated with a multi-drug resistant (MDR) strain from China, and
S. sonnei isolates resembled a strain characteristic of a current outbreak of MDR Shigella in England.
“The most prevalent lineage in Seattle was probably introduced to Washington State via international travel, with subsequent domestic transmission between at-risk groups,” the researchers wrote.
“Genomic analysis elucidated not only outbreak origin, but directed optimal approaches to testing, treatment, and public health response. Rapid diagnostics combined with detailed knowledge of local epidemiology can enable high rates of appropriate empirical therapy even in multidrug-resistant infection,” they continued.
UK Shigella Study Also Uses Genomics
Another study based in the United Kingdom (UK) used genomic analysis to investigate a Shigella outbreak as well.
Motivated by a UK Health Security Agency report of an increase in drug-resistance to common strains since 2021, the UK researchers studied Shigella cases from September 2015 to June 2022.
According to a paper they published in Lancet Infectious Diseases, the UK researchers “reported an increase in cases of sexually transmitted S. flexneri harboring blaCTX-M-27 (an antibiotic-resistant gene) in England, which is known to confer resistance to third-generation cephalosporins (antibiotics),” the researchers wrote.
Their analysis of plasmids (DNA with genes having antibiotic resistance) revealed a link in two drug-resistant Shigella strains at the same time, CIDRAP News explained.
“Our study reveals a worsening outlook regarding antimicrobial-resistant Shigella strains among MSM and highlights the value of continued integration of genomic analysis into surveillance and research,” the UK-based scientists wrote.
Current challenges associated with Shigella, especially as it evades treatment, may continue to demand attention from microbiologists, clinical laboratory scientists, and infectious disease specialists. Fortunately, use of genomic analysis—due to its ongoing improvements that have lowered cost and improved accuracy—has made it possible for public health researchers to better track the origins of disease outbreak and spread.
Data was used to create a transmission map that tracked the spread of infections among school athletes and helped public health officials determine where best to disrupt exposure
Genomic sequencing played a major role in tracking a SARS-CoV-2 outbreak in a Minnesota school system. Understanding how and where the coronavirus was spreading helped local officials implement restrictions to help keep the public safe. This episode demonstrates how clinical laboratories that can quickly sequence SARS-CoV-2 accurately and at a reasonable cost will give public health officials new tools to manage the COVID-19 pandemic.
Officials in Carver County, Minn., used the power of genomic epidemiology to map the COVID-19 outbreak, and, according to the Star Tribune, revealed how the B.1.1.7 variant of the SARS-CoV-2 coronavirus was spreading through their community.
“The resulting investigation of the Carver County outbreak produced one of the most detailed maps of COVID-19 transmission in the yearlong history of the pandemic—a chart that looks like a fireworks grand finale with infections producing cascading clusters of more infections,” the Star Tribune reported.
Using genetic sequencing, the Minnesota Department of Health produced the above map of the spread of the COVID-19 through Carver County’s schools. The animated graph includes epidemiological data from “10 high school teams, 10 club teams, 12 teams in a sports association, and three fitness/rec centers.” According to the Star Tribune, “The cluster shows a high ‘attack rate’ of infected people spreading the virus to multiple close contacts. Genomic sequencing found the more infectious B.1.1.7 variant of the virus in about a quarter of cases so far.” Click here to access the interactive version of the map. To see details about specific persons and locations, tap or hover over each dot. (Graphic copyright: Minnesota Department of Health/Star Tribune.)
Private Labs, Academic Labs, Public Health Labs Must Work Together
For gene sequencing to guide policy and decision making as well as it did in Carver County, coordination, cooperation, and standardization among public, private, and academic medical laboratories is required. Additionally, each institution must report the same information in similar formats for it to be the most useful.
“Maintain Policies That Slow Transmission: Variants will continue to emerge as the pandemic unfolds, but the best chance of minimizing their frequency and impact will be to continue public health measures that reduce transmission. This includes mask mandates, social distancing requirements, and limited gatherings.
“Prioritize Contact Tracing and Case Investigation for Data Collection: Cases of variants of concern should be prioritized for contact tracing and case investigation so that public health officials can observe how the new variant behaves compared to previously circulating versions.
“Develop a Genomic Surveillance Strategy: To guide the public health response, maximize resources, and ensure an equitable distribution of benefits, the US Department of Health and Human Services (HHS) should develop a national strategy for genomic surveillance to implement and direct a robust SARS-CoV-2 genomic surveillance program, drawing on resources and expertise from across the US government.
“Improve Coordination for Genomic Surveillance and Characterization: There are several factors in creating a successful genomic surveillance and characterization network. Clear leadership and coordination will be necessary.”
Practical Application of Genomic Sequencing
Genomic epidemiology uses the genetic sequence of a virus to better understand how and where a given virus is spreading, as well as how it may be mutating. Pathologists understand that this information can be used at multiple levels.
Locally, as was the case in Carver County, Minn., it helps school officials decide whether to halt sports for a time. Nationally, it helps scientists identify “hot spots” and locate mutations of the coronavirus. Using this data, vaccine manufacturers can adjust their vaccines or create boosters as needed.
“This is some of the most amazing epidemiology I’ve ever seen,” epidemiologist Michael Osterholm, PhD, Regents Professor, and Director of the Center for Infectious Disease Research and Policy (CIDRAP) at the University of Minnesota, told the Star Tribune, which reported that “A public health investigation linked 140 COVID-19 cases among more than 50 locations and groups, mostly schools and sports teams in Carver County. (Photo copyright: University of Minnesota.)
Will Cost Decreases Provide Opportunities for Clinical Laboratories?
Every year since genomic sequencing became available the cost has decreased. Experts expect that trend to continue. However, as of now, the cost may still be a barrier to clinical laboratories that lack financial resources.
“Purchasing laboratory equipment, computer resources, and staff training requires significant up-front investments. However, the cost per sequence is far less today than it was under earlier methods,” the GAO noted. This is good news for public and independent clinical laboratories. Like Carver County, a significant SARS-CoV-2 outbreak in the future may be averted thanks to genetic sequencing.
“The first piece of the cluster was spotted in a private K-8 school, which served as an incubator of sorts because its students live in different towns and play on different club teams,” the Star Tribune reported.
Finding such clusters may provide opportunities to halt the outbreak. “We can try to cut it off at the knees or maybe get ahead of it,” epidemiologist Susan Klammer with Minnesota Public Health and for childcare and schools, told the Star Tribune.
This story is a good example of how genomic sequencing and surveillance tracking—along with cooperation between public health agencies and clinical laboratories—are critical elements in slowing and eventually halting the spread of COVID-19.
On top of everything else during this pandemic, drug-resistant infections are threatening the most vulnerable patients in COVID-19 ICUs
New study by researchers at the University of Minnesota highlights the continuing need for microbiologists and clinical laboratories to stay alert for COVID-19 patients with drug-resistant infections. In their study, researchers highlighted CDC statistics about the number of Candida auris (C. auris) infections reported in the United States during 2020, for example.
In a paper, titled, “Three Cases of Worrisome Pan-Resistant C Auris Found in New York,” the Center for Infectious Disease Research and Policy (CIDRAP) at the University of Minnesota reported that “As of Dec 11, the CDC said 941 confirmed and probable C. auris cases have been reported in 13 states, and an additional 1,830 patients have been found to be colonized with the multidrug-resistant fungus. Most of the cases have been detected in the New York City area, New Jersey, and the Chicago area.”
Candida auris is a particularly nasty fungus. It spreads easily, is difficult to remove from surfaces, and can kill. Worst of all, modern drugs designed to combat this potentially deadly fungus are becoming less effective at eradicating it, and COVID-19 ICU patients appear especially vulnerable to C. auris infections.
COVID-19 and C. auris a Potentially Devastating Combination
Hospitals in many areas are at a critical capacity. Thus, hospital-acquired infections such as sepsis can be particularly dangerous for COVID-19 patients. Adding to the problem, C. auris requires special equipment to identify, and standard medical laboratory methods are not always enough. Misidentification is possible, even probable.
A paper in the Journal of Global Antimicrobial Resistance (JGAR), titled, “The Lurking Scourge of Multidrug Resistant Candida Auris in Times of COVID-19 Pandemic,” notes that “A particularly disturbing feature of COVID-19 patients is their tendency to develop acute respiratory distress syndrome that requires ICU admission, mechanical ventilation, and/or extracorporeal membrane oxygenation. … This haunting facet of COVID-19 pandemic has severely challenged even the most advanced hospital settings. Yet one potential confounder, not in the immediate attention of most healthcare professionals, is the secondary transmission of multidrug resistant organisms like the fungus Candida auris in COVID-19 ICUs. … C. auris outbreaks occur in critically ill hospitalized patients and can result in mortalities rates ranging from 30% to 72%. … Both C. auris and SARS-CoV-2 have been found on hospital surfaces including on bedrails, IV poles, beds, air conditioner ducts, windows and hospital floors. Therefore, the standard COVID-19 critical care of mechanical ventilation and protracted ventilator-assisted management makes these patients potentially susceptible to colonization and infections by C. auris.”
One study mentioned in the JGAR paper conducted in New Delhi, India, looked at 596 cases where patients were admitted to the ICU with COVID-19. Fifteen of them had infections caused by C. auris. Eight of those patients died. “Of note, four patients who died experienced persistent fungemia and despite five days of micafungin therapy, C. auris again grew in blood culture,” according to reporting on the study in Infection Control Today (ICT).
Some C. auris mortality rates are as high as 72%. And patients with weakened immune systems are at particular risk, “making it an even more serious concern when 8% to 9% of roughly 530,000 ICU patients in the United States have COVID-19,” ICT reported.
Apparently, the COVID-19 pandemic has created circumstances that are particularly suited for C. auris to spread. “Given the nosocomial transmission of SARS-CoV-2 by those infected, many hospital environments may serve as venues for C. auris transmission as it is a known environmental colonizer of ICUs,” wrote the JGAR paper authors.
CDC Reports and Recommendations
Along with being especially dangerous for people with weakened immune systems, C. auris infections also produce symptoms similar to those of COVID-19, “including fever, cough, and shortness of breath,” according to the CDC’s website. People admitted to ICUs with COVID-19 are especially vulnerable to bacterial and fungal co-infections. “These fungal co-infections are reported with increasing frequency and can be associated with severe illness and death,” says the CDC.
C. auris outbreaks in the United States have mostly been in long-term care facilities, but the pandemic seems to be changing that and more outbreaks have been detected in acute care facilities, the CDC reported. The lack of appropriate personal protective equipment (PPE), changes in infection control routines, and other factors could be to blame for the increase.
Just as community spread is an issue with COVID-19 variants, so too is it a concern with C. auris infections. “New C. auris cases without links to known cases or healthcare abroad have been identified recently in multiple states, suggesting an increase in undetected transmission,” the CDC noted.
As of January 19, 2021, according to the CDC the case count of C. auris infections in the US was 1,625, with California, Florida, Illinois, New Jersey, and New York having more than 100 cases each.
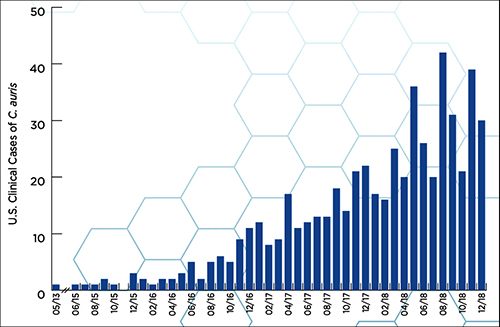
According to a CDC report, “Candida auris (C. auris) is an emerging multidrug-resistant yeast (a type of fungus). It can cause severe infections and spreads easily between hospitalized patients and nursing home residents.” The graphic above, taken from the report, illustrates how “C. auris began spreading in the United States in 2015. Reported cases increased 318% in 2018 when compared to the average number of cases reported in 2015 to 2017.” (Graphic copyright: Centers for Disease Control and Prevention.)
Using Clinical Laboratory Tests to Identify C. Auris
One of the big concerns about C. auris is that it is so difficult to detect, and that medical laboratories in some countries simply do not have the technology and resources to identify and tackle the infection.
“As C. auris diagnostics in resource-limited countries is yet another challenge, we feel that alerting the global medical community about the potential of C. auris as a confounding factor in COVID-19 is a necessity,” wrote the authors of the paper published in the Journal of Global Antimicrobial Resistance.
As if the COVID-19 pandemic has not been enough, drug resistant bacteria, viruses, and deadly fungi are threatening to wreak havoc among SARS-CoV-2 infected patients. Microbiologists and medical laboratory scientists know that testing for all types of infections is vitally important, but especially when it comes to infections caused by antibiotic-resistant bacteria (ARB) and other dangerous organisms that demonstrate antimicrobial resistance (AMR).
Microbiologists and clinical laboratory professionals will want to stay informed about the number of C. auris cases identified in the US and the locations and settings where the fungus was detected. They will want to be on the alert within their hospitals and health networks, as well as with the doctor’s offices served by their labs.
The guidelines are intended to improve safety specifically in diagnostic laboratories that handle specimens from humans and animals. Statistics indicate the clinical laboratory workers have infection rates for certain diseases that can be up to 20 times greater than that of the general population! It is believed current data understate the true rate of laboratory-acquired infections within the nation’s medical laboratories and pathology groups. (more…)