Good behavior in federal prison by the disgraced founder of the now-defunct clinical laboratory company earned her the reduction in her original sentence of 11 years
Elizabeth Holmes, founder of failed clinical laboratory blood analysis company Theranos, continues to serve a lengthy term in prison after being convicted of multiple counts of fraud in 2022. However, now comes news that good behavior at her federal prison has shortened her sentence by nearly two years, according to NBC News.
The latest reduction took Holmes’ release from December 2032 to August 2032 in her “11-plus-year (135 month) prison sentence for wire fraud and conspiracy,” NBC reported, adding that Holmes, though Theranos, “defrauded investors out of hundreds of millions of dollars.”
Holmes entered FPC Bryan, a federal prison camp in Bryan, Texas, to begin serving her term in May 2023.
“Holmes had her sentence computation done within the first 30 days of arriving at Bryan,” Forbes reported. Given Good Conduct Time (GCT), Holmes was given 608 days off calculated from the start of her sentence. “If she were to incur a disciplinary infraction, some of those days can be taken away. Most all prisoners receive 54 days per year of GCT based on the sentence imposed,” Forbes added.
The Federal Bureau of Prisons (BOP) can additionally shave off up to a year through its Residential Drug Abuse Program (RDAP). “To qualify, the prisoner must not have a disqualifying offense, such as terrorism or gun charge, and voluntarily provided information that they had a drug or alcohol problem prior to their arrest. This disclosure has to be done prior to sentencing during the pre-sentence interview and must be also documented in the Presentence Report, a detailed report used by the BOP to determine things like classification and programming for the prisoner,” Forbes noted.
Additionally, the federal First Step Act, which President Trump signed into law in 2018, enables Holmes to “earn up to 365 days off any imposed sentence by participating in prison programming such as a self-improvement classes, a job, or religious activities,” Forbes reported.
Given the opportunities to shave time off her sentence, Holmes may ultimately serve just 66 months of her original 135 month sentence in federal prison.
Elizabeth Holmes (above) taken backstage at TechCrunch Disrupt San Francisco 2014 when Holmes was at the height of her fame and popularity. At this point, Theranos’ Edison blood testing device had not yet been shown to be a fake. But evidence was mounting as clinical laboratory scientists and anatomic pathologists became aware of the technology’s shortcomings. (Photo copyright: Max Morse/Wikimedia Commons.)
Fall of a Silicon Valley Darling
Theranos boasted breakthrough technology and became an almost overnight sensation in Silicon Valley when it burst onto the scene in 2003. Holmes, a then 19-year-old Stanford University dropout, claimed Theranos would “revolutionize the world of blood testing by reducing sample sizes to a single pin prick,” Quartz reported.
The height of the company saw Theranos valued at $9 billion, which came crashing down when the Wall Street Journal reported in 2015 that questionable accuracy and procedures were being followed by the company, CNN reported.
“From the moment Holmes concluded her presentation and stepped off the podium on Monday afternoon, she, her company, and her comments became the number one subject discussed by attendees in the halls between sessions and in the AACC exhibit hall,” Michel wrote, adding, “The executive team and the investors at Theranos have burned through their credibility with the media, the medical laboratory profession, and the public. In the future, the company’s claims will only be accepted if presented with scientific data developed according to accepted standards and reviewed by credible third parties. Much of this data also needs to be published in peer-reviewed medical journals held in highest esteem.”
Ultimately, investors who had jumped in early with financial support for Theranos were defrauded of hundreds of millions of dollars and Holmes was sentenced to 11 years/three months behind bars.
“Theranos had only ever performed roughly a dozen of the hundreds of tests it offered using its proprietary technology, and with questionable accuracy. It also came to light that Theranos was relying on third-party manufactured devices from traditional blood testing companies rather than its own technology,” CNN added.
The company shut down in 2018.
And so, the Elizabeth Holmes saga continues with reductions in her prison sentence for “good behavior.” The irony will likely not be lost on the anatomic pathologists, clinical laboratory scientists, and lab managers who followed the federal trials.
Palmetto GBA’s Chief Medical Officer will cover how clinical laboratories billing for genetic testing should prepare for Z-Codes at the upcoming Executive War College in New Orleans
After multiple delays, UnitedHealthcare (UHC) commercial plans will soon require clinical laboratories to use Z-Codes when submitting claims for certain molecular diagnostic tests. Several private insurers, including UHC, already require use of Z-Codes in their Medicare Advantage plans, but beginning June 1, UHC will be the first to mandate use of the codes in its commercial plans as well. Molecular, anatomic, and clinical pathologist Gabriel Bien-Willner, MD, PhD, who oversees the coding system and is Chief Medical Officer at Palmetto GBA, expects that other private payers will follow.
“A Z-Code is a random string of characters that’s used, like a barcode, to identify a specific service by a specific lab,” Bien-Willner explained in an interview with Dark Daily. By themselves, he said, the codes don’t have much value. Their utility comes from the DEX Diagnostics Exchange registry, “where the code defines a specific genetic test and everything associated with it: The lab that is performing the test. The test’s intended use. The analytes that are being measured.”
The registry also contains qualitative information, such as, “Is this a good test? Is it reasonable and necessary?” he said.
Molecular, anatomic, and clinical pathologist Gabriel Bien-Willner, MD, PhD (above), Palmetto GBA’s Chief Medical Officer, will speak about Z-Codes and the MolDX program during several sessions at the upcoming Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management taking place in New Orleans on April 30-May 1. Clinical laboratories involved in genetic testing will want to attend these critical sessions. (Photo copyright: Bien-Willner Physicians Association.)
Palmetto GBA Takes Control
Palmetto’s involvement with Z-Codes goes back to 2011, when the company established the MolDX program on behalf of the federal Centers for Medicare and Medicaid Services (CMS). The purpose was to handle processing of Medicare claims involving genetic tests. The coding system was originally developed by McKesson, and Palmetto adopted it as a more granular way to track use of the tests.
In 2017, McKesson merged its information technology business with Change Healthcare Holdings LLC to form Change Healthcare. Palmetto GBA acquired the Z-Codes and DEX registry from Change in 2020. Palmetto GBA had already been using the codes in MolDX and “we felt we needed better control of our own operations,” Bien-Willner explained.
In addition to administering MolDX, Palmetto is one of four regional Medicare contractors who require Z-Codes in claims for genetic tests. Collectively, the contractors handle Medicare claims submissions in 28 states.
Benefits of Z-Codes
Why require use of Z-Codes? Bien-Willner explained that the system addresses several fundamental issues with molecular diagnostic testing.
“Payers interact with labs through claims,” he said. “A claim will often have a CPT code [Current Procedural Technology code] that doesn’t really explain what was done or why.”
In addition, “molecular diagnostic testing is mostly done with laboratory developed tests (LDTs), not FDA-approved tests,” he said. “We don’t see LDTs as a problem, but there’s no standardization of the services. Two services could be described similarly, or with the same CPT codes. But they could have different intended uses with different levels of sophistication and different methodologies, quality, and content. So, how does the payer know what they’re paying for and whether it’s any good?”
When the CPT code is accompanied by a Z-Code, he said, “now we know exactly what test was done, who did it, who’s authorized to do it, what analytes are measured, and whether it meets coverage criteria under policy.”
The process to obtain a code begins when the lab registers for the DEX system, he explained. “Then they submit information about the test. They describe the intended use, the analytes that are being measured, and the methodologies. When they’ve submitted all the necessary information, we give the test a Z-Code.”
The assessment could be as simple as a spreadsheet that asks the lab which cancer types were tested in validation, he said. On the other end of the scale, “we might want to see the entire validation summary documentation,” he said.
Commercial Potential
Bien-Willner joined the Palmetto GBA in 2018 primarily to direct the MolDX program. But he soon saw the potential use of Z-Codes and the DEX registry for commercial plans. “It became instantly obvious that this is a problem for all payers, not just Medicare,” he said.
Over time, he said, “we’ve refined these processes to make them more reproducible, scalable, and efficient. Now commercial plans can license the DEX system, which Z-Codes are a part of, to better automate claims processing or pre-authorizations.”
In 2021, the company began offering the coding system for Medicare Advantage plans, with UHC the first to come aboard. “It was much easier to roll this out for Medicare Advantage, because those programs have to follow the same policies that Medicare does,” he explained.
As for UHC’s commercial plans, the insurer originally planned to require Z-Codes in claims beginning Aug. 1, 2023, then pushed that back to Oct. 1, according to Dark Daily’s sister publication The Dark Report.
Then it was pushed back again to April 1 of this year, and now to June 1.
“The implementation will be in a stepwise fashion,” Bien-Willner advised. “It’s difficult to take an entirely different approach to claims processing. There are something like 10 switches that have to be turned on for everything to work, and it’s going to be one switch at a time.”
For Palmetto GBA, the commercial plans represent “a whole different line of business that I think will have a huge impact in this industry,” he said. “They have the same issues that Medicare has. But for Medicare, we had to create automated solutions up front because it’s more of a pay and chase model,” where the claim is paid and CMS later goes after errors or fraudulent claims.
“Commercial plans in general just thought they could manually solve this issue on a claim-by-claim basis,” he said. “That worked well when there was just a handful of genetic tests. Now there are tens of thousands of tests and it’s impossible to keep up.
They instituted programs to try to control these things, but I don’t believe they work very well.”
Bien-Willner is scheduled to speak about Palmetto GBA’s MolDX program, Z-Codes, and related topics during three sessions at the upcoming 29th annual Executive War College conference. Clinical laboratory and pathology group managers would be wise to attend his presentations. Visit here (or paste this URL into your browser: https://www.executivewarcollege.com/registration) to learn more and to secure your seat in New Orleans.
Forces in play will directly impact the operations and financial stability of many of the nation’s clinical laboratories
With significant regulatory changes expected in the next 18 to 24 months, experts are predicting a “Perfect Storm” for managers of clinical laboratories and pathology practices.
Currently looming are changes to critical regulations in two regulatory areas that will affect hospitals and medical laboratories. One regulatory change is unfolding with the US Food and Drug Administration (FDA) and the other regulatory effort centers around efforts to update the Clinical Laboratory Improvement Amendments of 1988 (CLIA).
The major FDA changes involve the soon-to-be-published Final Rule on Laboratory Developed Tests (LDTs), which is currently causing its own individual storm within healthcare and will likely lead to lawsuits, according to the FDA Law Blog.
In a similar fashion—and being managed under the federal Centers for Medicare and Medicaid Services (CMS)—are the changes to CLIA rules that are expected to be the most significant since 2003.
The final element of the “Perfect Storm” of changes coming to the lab industry is the increased use by private payers of Z-Codes for genetic test claims.
In his general keynote, Robert L. Michel, Dark Daily’s Editor-in-Chief and creator of the 29th Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management, will set the stage by introducing a session titled, “Regulatory Trifecta Coming Soon to All Labs! Anticipating the Federal LDT Rule, Revisions to CLIA Regulations, and Private Payers’ Z-Code Policies for Genetic Claims.”
“There are an unprecedented set of regulatory challenges all smashing into each other and the time is now to start preparing for the coming storm,” says Robert L. Michel (above), Dark Daily’s Editor-in-Chief and creator of the 29th Executive War College on Diagnostics, Clinical Laboratory, and Pathology Management, a national conference on lab management taking place April 30-May 1, 2024, at the Hyatt in New Orleans. (Photo copyright: The Dark Intelligence Group.)
Coming Trifecta of Disruptive Forces to Clinical Laboratory, Anatomic Pathology
The upcoming changes, Michel notes, have the potential to cause major disruptions at hospitals and clinical laboratories nationwide.
“Importantly, this perfect storm—which I like to describe as a Trifecta because these three disruptive forces that will affect how labs will conduct business—is not yet on the radar screen of most lab administrators, executives, and pathologists,” he says.
Because of that, several sessions at this year’s Executive War College conference, now in its 29th year, will offer information designed to give attendees a better understanding of how to manage what’s coming for their labs and anatomic pathology practices.
“This regulatory trifecta consists of three elements,” adds Michel, who is also Editor-in-Chief of Dark Daily’s sister publication The Dark Report, a business intelligence service for senior level executives in the clinical laboratory and pathology industry, as well in companies that offer solutions to labs and pathology groups.
According to Michel, that trifecta includes the following:
Element 1
FDA’s Draft LDT Rule
FDA’s LDT rule is currently the headline story in the lab industry. Speaking about this development and two other FDA initiatives involving diagnostics at the upcoming Executive War College will be pathologist Tim Stenzel, MD, PhD, former director of the FDA’s Office of In Vitro Diagnostics. It’s expected that the final rule on LDTs could be published by the end of April.
Stenzel will also discuss harmonization of ISO 13485 Medical Devices and the FDA’s recent memo on reclassifying most high-risk in vitro diagnostics to moderate-risk to ease the regulatory burden on companies seeking agency review of their diagnostic assays.
Salerno will also cover the CDC’s efforts to foster closer connections with clinical labs and their local public health laboratories, as well as the expanding menu of services for labs that his department now offers.
Element 3
Private Payer Use of Z-Codes for Test Claims
On the third development—increased use by private payers of Z-Codes for genetic test claims—the speaker will be pathologist Gabriel Bien-Willner, MD, PhD. He is the Medical Director of the MolDX program at Palmetto GBA, a Medicare Administrative Contractor (MAC). It is the MolDX program that oversees the issuance of Z-Codes for molecular and diagnostic tests.
UnitedHealthcare (UHC) was first to issue such a Z-Code policy last year, although it has delayed implementation several times. Other major payers are watching to see if UHC succeeds with this requirement, Michel says.
Other Critical Topics to be Covered at EWC
In addition to these need-to-know regulatory topics, Michel says that this year’s Executive War College will present almost 100 sessions and include 148 speakers. Some of the other topics on the agenda in New Orleans include the following and more:
Standardizing automation, analyzers, and tests across 25 lab sites.
Effective ways to attract, hire, and retain top-performing pathologists.
Leveraging your lab’s managed care contracts to increase covered tests.
“Our agenda is filled with the topics that are critically important to senior managers when it comes to managing their labs and anatomic pathology practices,” Michel notes.
“Every laboratory in the United States should recognize these three powerful developments are all in play at the same time and each will have direct impact on the clinical and financial performance of our nation’s labs,” Michel says. “For that reason, every lab should have one or more of their leadership team present at this year’s Executive War College to understand the implications of these developments.”
Visit here to learn more about the 29th Executive War College conference taking place in New Orleans.
Some hospital organizations are pushing back, stating that the new regulations are ‘too rigid’ and interfere with doctors’ treatment of patients
In August, the Biden administration finalized provisions for hospitals to meet specific treatment metrics for all patients with suspected sepsis. Hospitals that fail to meet these requirements risk the potential loss of millions of dollars in Medicare reimbursements annually. This new federal rule did not go over well with some in the hospital industry.
Sepsis kills about 350,000 people every year. One in three people who contract the deadly blood infection in hospitals die, according to the Centers for Disease Control and Prevention (CDC). Thus, the federal government has once again implemented a final rule that requires hospitals, clinical laboratories, and medical providers to take immediate actions to diagnose and treat sepsis patients.
The effort has elicited pushback from several healthcare organizations that say the measure is “too rigid” and “does not allow clinicians flexibility to determine how recommendations should apply to their specific patients,” according to Becker’s Hospital Review.
Perform blood tests within a specific period of time to look for biomarkers in patients that may indicate sepsis, and to
Administer antibiotics within three hours after a possible case is identified.
It also mandates that certain other tests are performed, and intravenous fluids administered, to prevent blood pressure from dipping to dangerously low levels.
“These are core things that everyone should do every time they see a septic patient,” said Steven Simpson, MD, Professor of medicine at the University of Kansas told Fierce Healthcare. Simpson is also the chairman of the Sepsis Alliance, an advocacy group that works to battle sepsis.
Simpson believes there is enough evidence to prove that the SEP-1 guidelines result in improved patient care and outcomes and should be enforced.
“It is quite clear that this works better than what was present before, which was nothing,” he said. “If the current sepsis mortality rate could be cut by even 5%, we could save a lot of lives. Before, even if you were reporting 0% compliance, you didn’t lose your money. Now you actually have to do it,” Simpson noted.
“We are encouraged by the increased attention to sepsis and support CMS’ creation of a sepsis mortality measure that will encourage hospitals to pay more attention to the full breadth of sepsis care,” Chanu Rhee, MD (above), Infectious Disease/Critical Care Physician and Associate Hospital Epidemiologist at Brigham and Women’s Hospital told Healthcare Finance. The new rule, however, requires doctors and medical laboratories to conduct tests and administer antibiotic treatment sooner than many healthcare providers deem wise. (Photo copyright: Brigham and Women’s Hospital.)
Healthcare Organizations Pushback against Final Rule
“By encouraging the use of broad spectrum antibiotics when more targeted ones will suffice, this measure promotes the overuse of the antibiotics that are our last line of defense against drug-resistant bacteria,” the AHA’s letter states.
In its recent coverage of the healthcare organizations’ pushback to CMS’ final rule, Healthcare Finance News explained, “The SEP-1 measure requires clinicians to provide a bundle of care to all patients with possible sepsis within three hours of recognition. … But the SEP-1 measure doesn’t take into account that many serious conditions present in a similar fashion to sepsis … Pushing clinicians to treat all these patients as if they have sepsis … leads to overuse of broad-spectrum antibiotics, which can be harmful to patients who are not infected, those who are infected with viruses rather than bacteria, and those who could safely be treated with narrower-spectrum antibiotics.”
CMS’ latest rule follows the same evolutionary path as previous federal guidelines. In August 2007, CMS announced that Medicare would no longer pay for additional costs associated with preventable errors, including situations known as Never Events. These are “adverse events that are serious, largely preventable, and of concern to both the public and healthcare providers for the purpose of public accountability,” according to the Leapfrog Group.
In 2014, the CDC suggested that all US hospitals have an antibiotic stewardship program (ASP) to measure and improve how antibiotics are prescribed by clinicians and utilized by patients.
Research Does Not Show Federal Sepsis Programs Work
He points to analysis which showed that though use of broad-spectrum antibiotics increased after the original 2015 SEP-1 regulations were introduced, there has been little change to patient outcomes.
“Unfortunately, we do not have good evidence that implementation of the sepsis policy has led to an improvement in sepsis mortality rates,” Rhee told Fierce Healthcare.
Rhee believes that the latest regulations are a step in the right direction, but that more needs to be done for sepsis care. “Retiring past measures and refining future ones will help stimulate new innovations in diagnosis and treatment and ultimately improve outcomes for the many patients affected by sepsis,” he told Healthcare Finance.
Sepsis is very difficult to diagnose quickly and accurately. Delaying treatment could result in serious consequences. But clinical laboratory blood tests for blood infections can take up to three days to produce a result. During that time, a patient could be receiving the wrong antibiotic for the infection, which could lead to worse problems.
The new federal regulation is designed to ensure that patients receive the best care possible when dealing with sepsis and to lower mortality rates in those patients. It remains to be seen if it will have the desired effect.
Nationwide, hospital losses are in the billions of dollars, which affects access to medical care including clinical laboratory testing
Hospitals and health systems across the United States continue to report substantial financial losses. At some institutions, this might severely restrict access to physicians and clinical laboratory testing for patients in those areas. The latest state to announce its hospitals were in trouble is Minnesota. The Minnesota Hospital Association (MHA) announced its hospitals are in “financial crisis” revealing that the state’s health systems experience hundreds of millions of dollars in operating losses annually.
The MHA stated that two out of three surveyed hospitals in Minnesota reported losing money in the cumulative amount of more than $400 million during the first half of 2023, KARE 11 reported. The MHA surveyed more than 70 health system members which represented facilities of all sizes and in all geographical regions of the state.
Rahul Koranne, MD, President and CEO of MHA told KARE 11 that part of the problem is that a larger proportion of patients rely on federal programs such as Medicare and Medicaid to pay hospital costs. Those programs provide lower reimbursement rates when compared to private insurers. In some facilities, almost 75% of patients are on one of these government programs.
“Those reimbursements, or payments, are fixed. So, we can’t raise prices. These two programs are paying significantly below the cost of providing care to our patients,” he noted. “So, if you have 70% of your patients covered by these governmental programs, we can’t raise prices, and they’re paying you below the cost of care—that’s what causes [the problem].”
He went on to state that workforce staffing represents a significant challenge for hospitals and urged the state legislature to address the needs of health professionals and facilities.
“We need to really resource it in this upcoming session and many sessions to come, so that we can have workers and staff we need,” Koranne said. “If we don’t have the money, and if we don’t have the workers, we will not be providing care and that would be sad.”
“This is a pretty grave state and, I would say, quite a crisis,” Rahul Koranne, MD (above), President and CEO of the Minnesota Hospital Association, told KARE 11. “Our not-for-profit hospitals and healthcare systems are hanging dangerously from this cliff and they’re getting tired.” Access to medical laboratory testing can be greatly affected by hospital financial losses. (Photo copyright: Twin Cities Business.)
Other US Healthcare Systems in Crisis as Well
Minnesota is not the only state with healthcare systems in financial crisis. Last year, the Washington State Hospital Association (WSHA) announced that hospitals in that state reported cumulative losses of $2 billion for 2022. Cassie Sauer, President and CEO of WSHA told the media that the massive deficits are “clear and incredibly concerning” to the state’s healthcare leaders.
In “Hospitals, Pharmacies Struggle to Be Profitable,” we reported that the WSHA survey determined that the state’s hospitals suffered collective operating losses of $750 million during the first six months of 2023.
“The financial losses that our hospitals are experiencing continue to be enormous,” Sauer told The Seattle Times. “Revenues simply are not keeping up with rapidly escalating costs. It’s most concerning as these large losses are putting patient care at risk in many communities across the state.”
The WSHA findings were based on a survey of 81 acute-care hospitals that represented about 98% of the state’s hospital beds. Of those facilities, 69 reported losing money mostly due to rising costs for supplies, labor, and other expenses as well as the need for longer hospital stays due to more complicated care and a larger percentage of patients on government programs, which offer lower reimbursement rates for care.
“When hospitals are not financially viable and over time sustain heavy losses, you must either increase revenue or reduce healthcare services,” Chelene Whiteaker, Senior Vice President, Government Affairs at WSHA, told The Seattle Times. “Reducing healthcare services is an option nobody wants on the table. So, that leaves increasing revenues.”
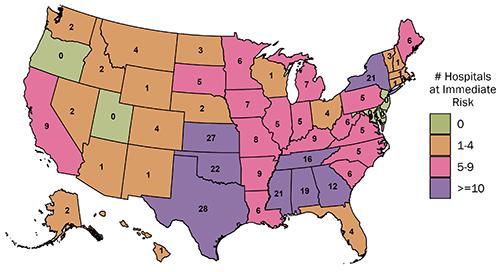
The graphic above from the Center for Healthcare Quality and Payment Reform (CHQPR) shows the number and location of rural hospitals in America that are at “immediate” risk of closure. The number of hospitals simply “at risk” of closure is substantially higher. Patients who depend on these hospitals would lose access to critical healthcare services including clinical laboratory testing. (Graphic copyright: Center for Healthcare Quality and Payment Reform.)
Becker’s Hospital Review reported last year that many hospitals across the country reported substantial losses in 2022. Three of the hospital systems in that article reported losses in the billions. They were:
In another article, Becker’s reported that 72 hospitals across the US closed departments or ended services in 2023. These cuts included the shuttering of health and urgent care clinics, the closure of outpatient cancer and pulmonary clinics, the reduction of certain surgical services and behavioral health services, and the ending of home healthcare services.
Some states are taking measures to prevent further hospital closures. But is it too late? In “California Doles Out $300 Million in No-Interest Loans to Save its Financially Struggling Hospitals,” The Dark Report’s sister publication Dark Daily covered how that state had launched an interest-free loan program to ensure local communities have access to community hospitals, their physicians, and clinical laboratories. No report on how many hospitals have been temporarily saved from closing thanks to this program.
If US hospitals continue to lose money at this rate, access to critical care—including clinical laboratory and anatomic pathology services—could be further restricted and facilities closed. These actions may also result in increased staff layoffs and have an even greater effect on patient care in Minnesota, Washington State, and throughout the US.