In an out-of-court settlement, two commercial clinical laboratory companies also agreed to reduce their prices for rapid antigen tests as well
How clinical laboratory companies were pricing their COVID-19 tests caught the attention of government authorities in South Africa. Government agencies in that country are establishing what they view as fair clinical laboratory pricing for private COVID-19 PCR (polymerase chain reaction) and rapid antigen tests without turning to litigation or fines.
The Competition Commission (Commission) is an organization charged with reviewing and acting on business practices in South Africa. In a December 11, 2021, news release, the Commission said it had reached a “ground-breaking agreement” with two private laboratories—Ampath and Lancet—to reduce their COVID-19 PCR test prices from 850 South African rand (R850) to R500 (from US$54.43 to US$31.97).
As of December 12, a third private laboratory company that also had been investigated, PathCare, had not agreed to the court settlement, Daily Maverick reported.
Also effective are lower prices for rapid antigen tests, the Commission said in a separate December 23 news release.
COVID Test Prices ‘Unfairly Inflated’
The changes in PCR test prices in South Africa followed a formal complaint by the Council for Medical Schemes which alleged the private pathology labs [the term for clinical laboratories in South Africa] were “supplying” COVID-19 PCR tests at “unfairly inflated, exorbitant, and/or unjustifiable” prices, Daily Maverick reported.
The clinical laboratory companies “exploited consumers by earning excessive profits on essential products or services,” Tembinkosi Bonakele (above), Commissioner of the South Africa Competition Commission, told the Daily Maverick. “It is always encouraging for companies to voluntarily consider reducing prices, especially where the public is detrimentally affected by the prices, as to avoid protracted litigation,” he added. (Photo copyright: Sowetan Live.)
According to the Daily Maverick, as part of the investigation, which began in October 2021, the Commission asked the private clinical laboratory companies for financial statements and costs of COVID-19 testing.
“We did, then, further interrogation in order to strip out what we saw was potentially padding the costing and unrelated costs. And on the basis of that, we came to the figure of R500,” James Hodge, told the Daily Maverick. Hodge is Chief Economist, Economic Research Bureau, and Acting Deputy Commissioner at the Competition Commission South Africa.
For its part, Lancet, Johannesburg, said in a statement that it “Appreciates the spirit of constructive engagement with the Commission which has resulted in an outcome that best serves the people of South Africa as they confront the fourth COVID wave. We are sensitive to the plight of the public and agree that reducing the COVID-19 PCR price is in best national interest.”
Clinical Laboratory Test Prices: Market Dynamics
So, were the prices too high? In the US, clinical laboratories are reimbursed considerably more by Medicare for COVID-19 testing (about $100), as compared to the South Africa private clinical lab prices.
Also, the Centers for Medicare and Medicaid Services (CMS) said in a statement that effective January 2021 it included in that rate an incentive of $25 to labs that provide results within 48 hours.
Medical laboratories are reimbursed $75 for a high throughput COVID-19 test when results are reported beyond 48 hours, CMS added.
Antigen Tests Prices Also Reduced
The Commission said that during its review of COVID-19 PCR test pricing it received a Department of Health Republic of South Africa complaint about prices for rapid antigen test pricing as well.
After another Commission review, PathCare, Lancet, and Ampath agreed to reduce prices for rapid antigen tests to a maximum of R150 or $9.74 (from a range of R250 to R350 or $16.28 to $22.79), a news release noted.
“The reduction of COVID-19 rapid antigen test prices will help alleviate the plight of consumers and widen accessibility and affordability of COVID-19 rapid antigen testing, which is a critical part of the initiatives to avoid escalation of the pandemic,” said Bonakele in the news release, which also stated that the Commission would receive financial statements from the three labs every few months.
The Commission also is reviewing a “large retail pharmacy chain’s” rapid antigen prices, which “follows a complaint lodged by the Department of Health (DOH), on December 14 2021, against service providers delivering COVID-19 Rapid Antigen tests in South Africa to consumers,” Cape Town Etc reported. The specific pharmacy chain was not identified.
Data Show COVID Plight in South Africa
More than 21.6 million COVID-19 tests have been offered by healthcare providers in South Africa, and 3.5 million cases were detected, according to the Department of Health, Republic of South Africa.
Considering those data, one wonders if the South African government acted fast enough on test pricing.
For medical laboratory leaders, it’s important to recognize that not only are lab services in the spotlight during the COVID-19 pandemic, business practices and prices also are being monitored by officials in this country.
Four-star general Jim Mattis testified that he eventually “didn’t know what to believe about Theranos anymore,” The Wall Street Journal reported
Former-Theranos CEO Elizabeth Holmes was known for her obsession with Steve Jobs, imitating not only the late Apple CEO’s well-known management style, but also his wardrobe choices. However, clinical laboratory managers and pathologists will not be surprised to learn that—in testimony during Holmes’ federal fraud trial—Theranos’ former laboratory director told jurors Holmes’ “confident demeanor” disappeared when she was told her revolutionary blood-testing technology “didn’t work,” KPIX5 TV reported.
During two days of testimony in San Jose, Calif., pathologist Adam Rosendorff, MD, told jurors that in the days leading up to the 2013 launch of the Edison blood-testing device he warned Holmes in emails and in person that the product wasn’t ready to be deployed commercially.
“I told her that the potassium was unreliable, the sodium was unreliable, the glucose was unreliable, [and] explained why,” testified the clinical pathologist. “She was very nervous. She was not her usual composed self. She was trembling a bit, her knee was tapping, her voice was breaking up. She was clearly upset,” he added.
KPIX5 TV reported that Holmes had told Rosendorff the laboratory could substitute conventional federal Food and Drug Administration (FDA)-approved devices as needed.
Rosendorff left his position with Theranos in November 2014. According to KPIX5, he told jurors, “I felt pressured to vouch for [medical laboratory] tests that I did not have confidence in. I came to believe that the company believed more about PR and fundraising than about patient care. The platform was not allowing me to function effectively as a lab director.”
Former Theranos Laboratory Director Adam Rosendorff, MD (above), testified in the federal fraud trial of Theranos founder and ex-CEO Elizabeth Holmes that he considered filing a whistleblower lawsuit against his employer because of his concerns about the Edison blood-testing device’s lack of reliability and accuracy of test results. “I wanted to get the word out about what was happening at Theranos,” the clinical pathologist told jurors, the Wall Street Journal reported. (Photo copyright: LinkedIn.)
In continuing testimony, Rosendorff acknowledged that tension increased between himself and Holmes and Theranos’ Chief Operating Officer Ramesh “Sunny” Balwani over Rosendorff’s concerns about the reliability and accuracy of the lab’s test results. At one point, he asked Balwani in an email if his name could be removed from the Theranos CLIA lab license so he would not be legally responsible for the lab’s problems.
Balwani’s own fraud trial begins in January 2022.
Former Theranos Lab Director Considered Filing a Qui Tam Lawsuit
According to the Wall Street Journal (WSJ), Rosendorff testified he forwarded work emails to his personal email account to protect himself in case the federal government investigated Theranos. He also considered filing a whistleblower lawsuit against the company.
“I wanted to get the word out about what was happening at Theranos,” he testified, the Wall Street Journal reported.
The government’s first witnesses were former Theranos employees:
Gangakehedkar testified that Holmes knew about reliability issues with the Edison blood-testing device, yet pressured staff to move forward with the Walgreens roll out.
Theranos’ partnership with Walgreens ended in 2016, after Theranos voided years of test results performed on its machines.
In “Former Theranos Chemist Says Elizabeth Holmes Was Aware of Testing Failures,” the WSJ reported that Gangakhedkar resigned from Theranos in September 2013, taking with her Theranos documents and copies of emails in which she expressed her concerns to Holmes and others about continuing problems with Theranos’ lab tests.
“I was scared that things would not go well,” Gangakhedkar testified, her voice breaking at one point. “I was afraid I would be blamed.”
As foreshadowed during the trial’s opening statements, Holmes’ defense team plans to argue that their client did not intend to defraud investors but believed her blood-testing technology—portrayed as capable of running more than 200 tests using a finger-stick sample of blood—would revolutionize the healthcare industry.
In his opening remarks to the jury, Lance Wade, JD, a member of the Holmes defense team from Williams and Connolly LLP, told jurors that evidence will show Theranos investors were “incredibly sophisticated and knew the risks” and were actually pushing to invest in Theranos. The reality of the case, he said, is “far more human and real, and oftentimes, I hate to say it, technical and complicated and boring” than what the federal government has suggested, Forbes reported.
Four-star General Jim Mattis (ret.) Testifies
According to the Wall Street Journal, former Defense Secretary Jim Mattis testified he joined the Theranos board in the summer of 2013, at which time he invested $85,000 in the company. He said he had first met Holmes in San Francisco in 2011. At the time, Mattis, a Marine Corps four-star general, was leading the US military’s Central Command (CENTCOM) and that, according to testimony, he recognized the Edison device’s potential for use on the battlefield.
Mattis testified he and other Theranos board members were surprised to learn in 2015 that Theranos was using blooding testing equipment from competing companies.
“There came a time when I didn’t know what to believe about Theranos anymore,” he told jurors, according to the WSJ. Mattis resigned from the board in 2016, after learning he would be nominated as Secretary of Defense in the Trump administration.
The courtroom sketch above shows former Defense Secretary four-star general Jim Mattis testifying Wednesday at the criminal trial of Theranos founder Elizabeth Holmes in San Jose, Calif. (Graphic copyright: Vicki Behringer.)
The trial is expected to last until mid-December, with jurors hearing testimony on Tuesdays, Wednesdays, and Fridays. For clinical laboratory scientists, each day of testimony should bring a new round of surprises so stay tuned.
It did not take long for fraudsters to pursue hundreds of billions of federal dollars designated to support SARS-CoV-2 testing and it is rare when federal prosecutors bring cases only a few months after illegal lab testing schemes are identified
As if the COVID-19 pandemic weren’t bad enough, unscrupulous clinical laboratory operators quickly sought to take advantage of the critical demand for SARS-CoV-2 testing and defraud the federal government.
Unfortunately for the many defendants in these cases, federal investigations into alleged cases of fraud were launched with noteworthy speed. As a result of these investigations into alleged healthcare fraud by clinical laboratories and other organizations during fiscal year (FY) 2020, the US Department of Justice (DOJ) announced the US government has recovered $1.8 billion.
The federal prosecutions involved dozens of medical laboratory owners and operators who paid back “hundreds of millions in alleged federal healthcare program losses,” Goodwin Life Sciences Perspectives explained.
When combined with similar efforts starting in prior years, the program has returned to the federal government and private individuals a total of $3.1 billion, the DOJ noted.
“In its 24th year of operation, the program’s continued success confirms the soundness of a collaborative approach to identify and prosecute the most egregious instances of healthcare fraud, to prevent future fraud and abuse, and to protect program beneficiaries,” the report states.
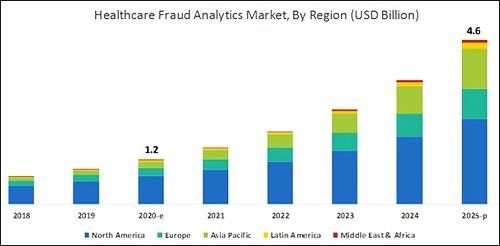
According to the graphic above, which is based on analysis by B2B research company MarketsandMarkets, “North America will dominate the healthcare fraud analytics market from 2020–2025.” As clinical laboratory testing represents a significant portion of the fraud, medical lab managers will want to remain vigilant. (Graphic copyright: MarketsandMarkets.)
COVID-19 Pandemic an Opportunity for Fraud
The HHS report notes that the COVID-19 pandemic required CMS to develop a “robust fraud risk assessment process” to identify clinical laboratory fraud schemes, such as offering COVID-19 tests in exchange for personal details and Medicare information.
“In one fraud scheme, some labs are targeting retirement communities claiming to offer COVID-19 tests but are drawing blood and billing federal healthcare programs for medically unnecessary services,” the HHS report notes.
Still other alleged schemes involved billing for expensive tests and services in addition to COVID-19 testing. “For example, providers are billing a COVID-19 test with other far more expensive tests such as the Respiratory Pathogen Panel (RPP) and antibiotic resistance tests,” the report says.
“Other potentially unnecessary tests being billed along with a COVID-19 test include genetic testing and cardiac panels CPT (current procedural terminology) codes. Providers are also billing respiratory, gastrointestinal, genitourinary, and dermatologic pathogen code sets with the not otherwise specified code CPT 87798,” the report states.
Different Types of Healthcare Organizations Investigated in 2020
Beyond clinical laboratories, the HHS’ 124-page report also shares criminal and civil investigations of other healthcare organizations and areas including:
clinics,
drug companies,
durable medical equipment,
electronic health records,
home health providers,
hospice care,
hospitals and healthcare systems,
medical devices,
nursing home and facilities,
pharmacies, and
physicians/other practitioners.
According to the DOJ, “enforcement actions” in 2020 included:
1,148 new criminal healthcare fraud investigations opened,
440 defendants convicted of healthcare fraud and related crimes,
1,079 civil healthcare fraud investigations opened, and
1,498 pending civil health fraud matters at year-end.
“Federal Bureau of Investigation (FBI) investigative efforts resulted in over 407 operational disruptions of criminal fraud organizations and the dismantlement of the criminal hierarchy of more than 101 healthcare fraud criminal enterprises,” the DOJ reported.
Furthermore, the report said OIG investigations in 2020 led to:
578 criminal actions against people or organizations for Medicare-related crimes,
781 civil actions such as false claims, and
2,148 people and organizations eliminated from Medicare and Medicaid participation.
Implications for Clinical Laboratories
In 2020, OIG issued 178 reports, completed 44 evaluations, and made 689 recommendations to HHS divisions.
Clinical laboratory leaders may be most interested in those related to patient identification as a means to combating fraud and Medicare Part B lab testing reimbursement.
The HHS report says, “Medicare Advantage (MA) encounter data continue to lack National Provider Identifiers (NPIs) for providers who order and/or refer … clinical laboratory services,” adding that, “Almost half of MA organizations believe that using NPIs for ordering providers is critical for combating fraud.”
Additionally, the report states, “Medicare Part B spending for lab tests increased to $7.6 billion in 2018, despite lower payment rates for most lab tests. The $459 million spending increase was driven by:
“increased spending on genetic tests,
“ending the discount for certain chemistry tests, and the
“move to a single national fee schedule.”
Medical laboratory leaders may be surprised to learn that federal healthcare investigators were so vigorous in their investigations, even during the worst of the COVID-19 pandemic.
Vigilance is critical to ensure labs do not fall under the DOJ’s scrutiny. This HHS report, which describes the types and dollars involved in fraudulent schemes by clinical labs and other providers, could help inform revisions to federal compliance regulations and statutes.
CMS says it is responding to hospitals’ plea for relief from burdensome reporting requirements, but not altering federal price transparency laws
Despite federal price transparency law that went into effect January 1 after a year-long court battle, some hospitals continue to balk at sharing their payer-negotiated rates for healthcare goods and services—including medical laboratory testing—claiming a variety of challenges due to the COVID-19 pandemic, vaccine distribution, and other difficulties, Modern Healthcare reported.
This requirement was originally part of the Hospital Price Transparency Final Rule (84 FR 65524), passed in 2019 during the Trump administration, which required hospitals to “establish, update, and make public a list of their standard charges for the items and services that they provide,” including clinical laboratory test prices. This reporting requirement did not sit well with the AHA.
In a statement, Ashley Thompson, Senior Vice President for Public Policy Analysis and Development for the American Hospital Association, said, “This policy will require hospitals to divert critically needed resources during this historic pandemic to administrative tasks that will not benefit patients.” She added, “We do not believe CMS has the authority to compel the disclosure of these terms and our legal challenge remains ongoing.”
However, if the new proposed rule goes into effect, CMS would no longer expect hospitals to report the rates they have negotiated with each Medicare Advantage plan, RevCycleIntelligence reported.
“Hospitals are often the backbone of rural communities—but the COVID-19 pandemic has hit rural hospitals hard, and too many are struggling to stay afloat,” HHS Secretary Xavier Becerra (above) said in an announcement, RevCycleIntelligence reported. “This rule will give hospitals more relief and additional tools to care for COVID-19 patients and it will also bolster the healthcare workforce in rural and underserved communities.” (Photo copyright: Modern Healthcare.)
CMS Relieving a Burden, Not Eliminating a Requirement
In the fact sheet, CMS wrote that it “is proposing to repeal the requirement that a hospital report on the Medicare cost report the median payer-specific negotiated charge that the hospital has negotiated with all of its MA organization payers, by MS-DRG (Medicare-severity diagnosis related group), for cost reporting periods ending on or after January 1, 2021. CMS estimates this will reduce administrative burden on hospitals by approximately 64,000 hours.”
Experts noted that CMS is attempting to reduce providers’ administrative burdens, while keeping federal price transparency requirements in effect.
“The repeal of this requirement more falls into the bucket of easing hospitals’ burden as opposed to the agency’s stance on hospital price transparency,” Caitlin Sheetz, Director and Head of Analytics at ADVI Health, LLC, told Fierce Healthcare.
Still, the recent CMS action could be a sign that price transparency requirements for hospitals will not intensify, she added. “I would think it is very unlikely that [CMS] would put out a rule that is easing up hospital administrative burden [and] they would then ramp up audits for the hospital price transparency rule.”
AHA Supports CMS’ Latest Proposed Rule on Hospital Reporting
The AHA said the new proposed rule moves in the right direction.
In a statement, Tom Nickels, Executive Vice President of the AHA, said, “We have long said that privately negotiated rates take into account any number of unique circumstances between a private payer and a hospital and their disclosure will not further CMS’ goal of paying market rates that reflect the cost of delivering care.” He added, “We once again urge the agency to focus on transparency efforts that help patients access their specific financial information based on their coverage and care.”
Though federal price transparency rules are evolving, medical laboratories are encouraged to accept that consumer demand is one powerful force driving this trend. Thus, clinical laboratories that currently make it easy for patients to see the prices for common medical laboratory tests in advance of service should gain competitive advantage from this feature over time.
Clinical laboratories may see increase in flu and COVID-19 specimen processing as people return to pre-pandemic social behaviors, experts predict
While SARS-CoV-2 infections continue to ravage many parts of the world, influenza (flu) cases in North America have hit a historic low. As winter approached last year, infectious disease experts warned of a “twindemic” in which the COVID-19 outbreak would combine with seasonal influenza to overwhelm the healthcare system. But this did not happen, and many doctors and medical laboratory scientists are now investigating this unexpected, but welcomed, side-effect of the pandemic.
From the start of the current flu season in September 2020, clinical laboratories in the US reported that 1,766 specimens tested positive for flu out of 931,726—just 0.2%—according to the CDC’s Weekly US Influenza Surveillance Report. That compares with about 250,000 positive specimens out of 1.5 million tested in the 2019-2020 flu season, the CDC reported. Public health laboratories reported 243 positive specimens out of 438,098 tested.
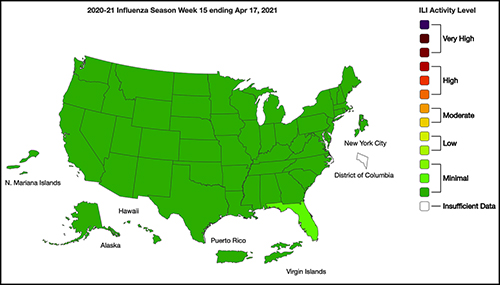
The graphic above taken from the CDC’s Weekly Influenza Surveillance Report for the week ending April 17, 2021, illustrates how “Nationwide during week 15, 1.1% of patient visits reported through ILINet were due to ILI [Influenza-like Illness].” This percentage, according to the CDC, is below the national baseline of 2.6%. “Seasonal influenza activity in the United States remains lower than usual for this time of year.” (Graphic copyright: Federal Centers for Disease Control and Prevention.)
Fear of COVID-19 Linked to Fewer Flu Deaths in Children
WebMD reported that just one child in the US has died from the flu this year, compared with 195 in 2020. Why the low numbers?
Precautions people take to avoid COVID-19 transmission, including masking, social distancing, and handwashing.
Reduced human mobility, including less international travel.
Higher-than-usual flu vaccination rates. As of February 26, the CDC reported that nearly 194 million doses of flu vaccine had been distributed in the US.
WebMD noted this could be a record, but that the CDC data doesn’t indicate how many doses were actually administered.
However, Schaffner told WebMD that efforts to keep kids home from school and away from social gatherings were likely a bigger factor. “Children are the great distributors of the influenza virus in our society,” he said. But due to fears about COVID-19 transmission, kids “weren’t even playing together, because mothers were keeping them off the playground and not having play dates.”
Repercussions for Fighting Flu Next Year
Public health experts welcomed the low flu levels, however, Politico reported that limited data about flu circulation this year could hamper efforts to develop an effective vaccine for next season’s flu strains.
Each February, Politico explained, experts convened by the World Health Organization (WHO) look at data from the current and previous flu seasons to predict which strains are likely to predominate in the Northern Hemisphere next winter. That includes data about which strains are currently circulating in the Southern Hemisphere. The WHO uses these predictions to recommend the composition of flu vaccines. In the US, the final decision is made by an FDA advisory committee.
A similar WHO meeting in September guides vaccine development in the Southern Hemisphere.
The WHO issued this year’s Northern Hemisphere recommendations on Feb. 26. The advisory includes recommendations for egg-based and cell- or recombinant-based vaccines, and for quadrivalent (four-strain) or trivalent (three-strain) vaccines.
In a document accompanying the recommendations, the WHO acknowledged concerns about this year’s limited pool of data.
“The volume of data available from recently circulating influenza viruses, and the geographic representation, have been significantly lower for this northern hemisphere vaccine recommendation meeting than is typical,” the document stated. “The reduced number of viruses available for characterization raises uncertainties regarding the full extent of the genetic and antigenic diversity of circulating influenza viruses and those likely to pose a threat in forthcoming seasons.”
The report notes that experts identified changes in circulating Influenza A(H3N2) viruses this year, and that the changes are reflected in the new vaccine recommendation.
But Paul A. Offit, MD, who serves on the FDA’s vaccine advisory panel, downplayed worries about the vaccine. “The belief is that there was enough circulating virus to be able to pick what is likely to be the strains that are associated with next year’s flu outbreak,” he told Politico. Offit is a Professor of Vaccinology and Pediatrics at the Perelman School of Medicine at the University of Pennsylvania and Director of the Vaccine Education Center at the Children’s Hospital of Philadelphia.
Pediatrician and internationally recognized expert in the fields of virology and immunology, Paul A. Offit, MD (above), told Politico that the low level of flu circulation this year, along with the resulting uncertainty, “is unprecedented.” Clinical laboratories might not have noticed the severe decrease in influenza specimens sent for processing due to being hyper-focused on COVID-19 testing. But as the pandemic subsides, loss of flu testing revenues will likely become more apparent. (Photo copyright: University of Pennsylvania.)
Offit suggests that efforts to mitigate the COVID-19 outbreak could be useful to combat other infectious disease outbreaks. However, both Offit and Gostin expressed doubt about that prospect.
“I mean, could we reasonably in a winter month, wear masks just at least when we’re outside in large crowds? … Or are we comfortable having hundreds of 1000s of cases of hospitalizations for flu and 10s of 1000s [of] deaths? I suspect the answer is B. We’re comfortable with that, we’re willing to have that even though we just learned, there’s a way to prevent it,” Offit told Politico.
“Remember after the 1918 flu pandemic, most people don’t realize what happened when that was over. But what happened was the roaring ‘20s,” Gostin told Politico. “People started congregating, mingling, hugging, kissing. All the things they missed. They crowded into theaters and stadiums and went back to church. That’s what’s likely to happen this fall and that makes the influenza virus very happy.”
So, what should clinical laboratories expect in future flu and COVID-19 vaccines? That is not yet clear. One thing is certain, though. New lab test panels that test for influenza and the SARS-CoV-2 coronavirus will be arriving in the marketplace.