Medical laboratories may find opportunities guiding hospital telehealth service physicians in how clinical lab tests are ordered and how the test results are used to select the best therapies
Telehealth is usually thought of as a way for patients in remote settings to access physicians and other caregivers. But now comes a pair of studies that indicate use of telehealth in inpatient settings is outpacing the growth of telehealth for outpatient services.
This is an unexpected development that could give clinical laboratories new opportunities to help improve how physicians in telehealth services use medical laboratory tests to diagnose their patients and select appropriate therapies.
Dual Surveys Compare Inpatient and Outpatient Telehealth
Service Use
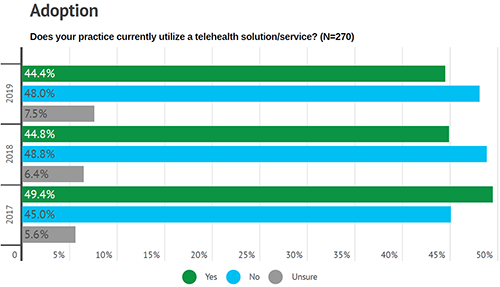
Definitive Healthcare (DH) of Framingham, Mass., is an analytics company that provides data on hospitals, physicians, and other healthcare providers, according to the company’s website. A survey conducted by DH found that use of telehealth solutions—such as two-way video webcams and SMS (short message service) text—has increased by inpatient providers from 54% in 2014 to 85% in 2019, a news release stated.
Meanwhile, a second Definitive Healthcare survey suggests
use of telehealth in outpatient physician office settings remained essentially
flat at 44% from 2018 to 2019, according to another news
release.
For the inpatient report, Definitive Healthcare polled 175 c-suite
providers and health
information technology (HIT) directors in hospitals and healthcare systems.
For the outpatient survey, the firm surveyed 270 physicians and outpatient
facilities administrators.
DH’s research was aimed at learning the status of telehealth
adoption, identifying the type of telehealth technology used, and predicting possible
further investments in telehealth technologies.
Most Popular Inpatient Telehealth Technologies
On the inpatient side, 65% of survey respondents said the most used telehealth mode is hub-and-spoke teleconferencing (audio/video communication between sites), Healthcare Dive reported. Also popular:
Fierce
Healthcarereports that the telehealth technologies showing the largest
increase by hospitals and health networks since 2016 are:
Two-way video/webcam between physician and
patient (70%, up from 47%);
Population health management tools, such as SMS
text (19%, up from 12%);
Remote patient monitoring using clinical-grade
devices (14%, up from 8%);
Mobile apps for concierge services (23%, up from
17%).
“Organizations are finding new and creative ways through telehealth to fill gaps in patient care, increase care access, and provide additional services to patient populations outside the walls of their hospital,” Kate Shamsuddin, Definitive Healthcare’s Senior Vice President of Strategy, told Managed Healthcare Executive.
DH believes investments in telehealth will increase at
hospitals as well as physician practices. In fact, 90% of respondents planning
to adopt more telehealth technology indicated they would likely start in the
next 18 months, the news releases state.
Most Popular Outpatient Telehealth Technologies
In the outpatient telehealth survey, 56% of physician
practice respondents indicated patient portals as the
leading telehealth technology, MedCity
News reported. That was followed by:
Hub-and-spoke teleconferencing (42%);
Concierge services (42%);
Clinical- and consumer-grade remote patient
monitoring products (21% and 12%).
While adoption of telehealth technology was flat over the
past year, 68% of physician practices did use two-way video/webcam technology
between physician and patient, which is up from 45% in 2018, Fierce
Healthcare reported.
The graph above, taken from the Definitive Healthcare 2019 survey, shows the percentage of telehealth use among surveyed outpatient settings. “The results show how telehealth continues to be one of the core linchpins for providers,” Kate Shamsuddin, Definitive Healthcare’s Senior Vice President of Strategy, told Healthcare Dive. (Graphic copyright: Definitive Healthcare.)
MedCity News reports that other telehealth technologies in
use at physician practices include:
Mobile apps for concierge service (33%);
Two-way video between physicians (25%);
SMS population management tools (20%).
Telehealth Reimbursement and Interoperability Uncertain
Why do outpatient providers appear slower to adopt
telehealth, even though they generally have more patient encounters than
inpatient facilities and need to reach out further and more often?
Definitive Healthcare reports that 20% of physician practice
respondents are “satisfied with the practice’s current solutions and services,”
and though telehealth reimbursement is improving, 13% are unsure they will be
reimbursed for telehealth services.
The Centers
for Medicare and Medicaid Services (CMS) states that Medicare
Part B covers “certain telehealth services,” and that patients may be
responsible for paying 20% of the Medicare approved amount. CMS also states
that, effective in 2020, Medicare
Advantage plans may “offer more telehealth benefits,” as compared to
traditional Medicare.
“There is not only a need for more clarity around reimbursement policies, but also a need for more interoperable telehealth solutions that can be accessed through electronic health record or electronic medical record systems, as well as a better understanding about what types of telehealth options are available,” said Jason Krantz (above), CEO, Definitive Healthcare, in the outpatient telehealth survey news release. (Photo copyright: Definitive Healthcare.)
The increase in telehealth use at hospitals—as well as its
increased adoption by physician offices—may provide clinical laboratories with opportunities
to assist telehealth doctors with lab test use and ordering. By engaging in telehealth
technology, such as two-way video between physicians, pathologists also may be
able to help with the accuracy of diagnoses and timely and effective patient
care.
Journalists, researchers, and a growing number of consumers now recognize the often huge variability in the prices different medical laboratories charge for the same lab tests
One step at a time, the Medicare program, private health insurers, and employers are putting policies in place that require providers—including clinical laboratories and pathology groups—to allow patients and consumers to see the prices they charge for their medical services. Recent studies into test price transparency in hospitals and health networks have garnered the attention of journalists, researchers, and patients. These groups are now aware of enormous variations in pricing among providers within the same regions and even within health networks.
Now that hospitals’ medical laboratory test prices are
required to be easily accessible to patients, researchers are beginning to compile
test prices across different hospitals and in different states to document and
publicize the wide variation in what different hospital labs charge for the
same medical laboratory tests.
Journalists are jumping on the price transparency bandwagon
too. That’s because readers show strong interest in stories that cover the
extreme range of low to high prices providers will charge for the same lab
test. This news coverage provides patients with a bit more clarity than
hospitals and other providers might prefer.
Shocking Variations in Price of Healthcare
Services, including Medical Laboratory Tests
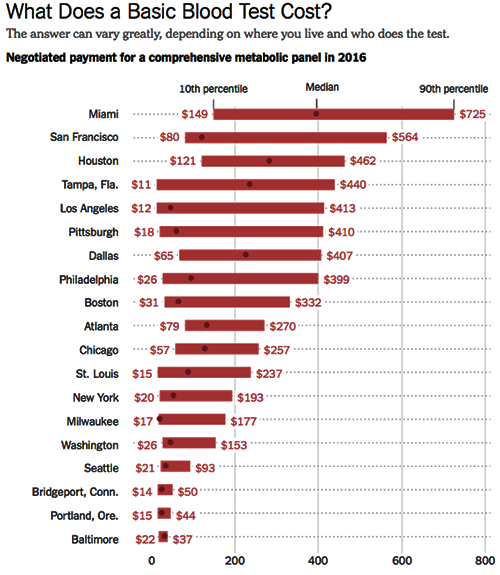
The Health Care Cost Institute (HCCI) in conjunction with the Robert Wood Johnson Foundation (RWJF), examines price levels of various procedures and medical laboratory tests at healthcare institutions across the United States in the first release of a series called Healthy Marketplace Index. According to the HCCI website, “a common blood test in Beaumont, Texas ($443) costs nearly 25 times more than the same test in Toledo, Ohio ($18).”
In April, the New
York Times (NYT) made the wide variation
in how clinical laboratories price their tests the subject of an article titled,
“They Want It to Be Secret: How a Common Blood Test Can Cost $11 or Almost
$1,000.” The article discusses the HCCI findings.
The coverage by these two well-known entities is increasing the
public’s awareness of the broad variations in pricing at clinical laboratories
around the country.
Aside from the large differences in medical laboratory test
prices in different regions, the HCCI found that there are sometimes huge price
variations within a single metro area for the same lab tests. “In just one
market—Tampa, Fla.—the most expensive blood test costs 40 times as much as the
least expensive one,” the NYT notes.
In other industries, those kinds of price discrepancies are
not common. The NYT made a comparatively outrageous example using
ketchup, saying, “A bottle of Heinz ketchup in the most expensive store in a
given market could cost six times as much as it would in the least expensive
store,” adding, however, that most bottles of ketchup tend to cost about the
same.
The graphic above is taken from the New York Times article on test price discrepancies in healthcare. The range of prices for the medical lab test known as a comprehensive metabolic panel are for metropolitan areas only. The data is sourced from the Health Care Cost Institute study. It’s easy to see why patients would be confused by clinical laboratory pricing that varies so widely. (Graphic copyright. The New York Times.)
The CMS mandate designed to make the prices of medical services accessible to healthcare consumers has, in many ways, made things more confusing. For example, most hospitals simply made their chargemaster available to consumers. Chargemasters can be confusing, even to industry professionals, and are filled with codes that make no sense to the average consumer and patient.
“This policy is a tiny step forward but falls far short of what’s needed. The posted prices are fanciful, inflated, difficult to decode and inconsistent, so it’s hard to see how an average person would find them useful,” Jeanne Pinder, Founder and Chief Executive of Clear Health Costs, a consumer health research organization, told the NYT in an article on how hospitals are complying with the mandate to publish prices.
In addition to the pricing information being difficult for
consumers to parse, it also may lead them to believe they would need to pay
much more for a given procedure than they would actually be billed, resulting
in patients opting to not get care they actually need.
Why Having a Strategy Is Critically
Important for Clinical Laboratories
Clinical laboratories are in a particularly precarious position in all of this pricing confusion. For one thing, most hospital-based medical laboratories don’t have a way to communicate directly with consumers, so they don’t have a way to explain their pricing. Additionally, articles and studies such as those in the NYT and from the HCCI, which describe drastic price variations for the same tests, tend to cast clinical laboratories in a somewhat sinister light.
To prepare for this, medical laboratory personnel should be
trained in how to address customer requests for pricing and how to explain
variations in test prices among labs, before such requests become problematic. Lab
staff should be able to explain how patients can find out the cost of a given
test, and what choices they have regarding specific tests.
In 2016, Dark Daily’s sister-publication, The Dark Report (TDR), dedicated an entire issue to the impact of reference pricing on the clinical laboratory industry. In that issue, TDR reported on how American supermarket chain Safeway helped guide their employees to lower-priced clinical laboratories for lab tests, resulting in $2.7 million savings for the company in just 24 months. Safeway simply implemented reference pricing; the company analyzed lab test prices of 285 tests for all of the labs in its network, and then set the maximum amount it would pay for any given test at the 60th percentile.
If a Safeway employee selected a medical laboratory with prices less than the 60th percentile, the normal benefits and co-pays applied. But if a Safeway employee went to clinical laboratories that charged more than the 60th percentile level, they were required to pay both their deductible and the amount above Safeway’s maximum.
Safeway’s strategy revealed wide variation in testing
prices, just as the HCCI report found. This means that employers can be added
to the list of those who are paying much closer attention to medical laboratory
test pricing than they have in the past. These are developments that should
motivate forward-looking pathologists and clinical laboratory executives to act
sooner rather than later to craft an effective strategy for responding to consumer
and patient requests for lab test price transparency.
EMPIs may help clinical laboratories ensure their patients and medical records are properly matched with medical laboratory test results and specimens
Mix-ups between patients and their medical records, known in
the healthcare industry as “patient mismatching,” happen far too frequently in
hospitals and clinics worldwide. When surgery is involved, such mismatches can lead
to deadly errors. However, clinical
laboratories and pathology
groups also must take steps to ensure patients, their medical records, and their
biological specimens remain properly matched.
Once horrific incident in 2016 involved Saint Vincent Hospital in
Worcester, Mass. Believing they were operating on a patient with a kidney
tumor, surgeons mistakenly removed a healthy kidney from the wrong patient. The
cause of the patient mismatch was a mix-up with CT scans. The two patients
shared similar names, Managed
Care reported.
Sadly, patient mismatching is not a new or rare problem. Patient
mismatches often lead to delays, extra costs to fix duplicate information, and
tragically, unnecessary surgery and inappropriate care, Healthcare
Dive noted.
According to Managed Care, organizations working on
solutions include:
“Incorrect matches could result in patients getting the
wrong medicine, and failure to link records could lead to treatment decisions
made without access to up-to-date laboratory test results,” Pew noted in an issues
brief.
Pew and the MAeHC interviewed 18 hospital, medical practice,
and health information technology exchange leaders. The respondents admitted
that they are uncertain about the extent of the matching problem.
“They don’t know all the records that should be related and
thus cannot understand what percentage of those are unlinked,” the researchers
wrote.
Nonetheless, the researchers found that patient/record match
rates fall “far below the desired level” for effective data exchange among
organizations, Healthcare Dive reported.
For pathologists and clinical laboratory managers, the
Pew/MAeHC study had several key takeaways, such as:
“Match rates are far below the desired level for
effective data exchange.
“An increased demand for interoperability—the
exchange of electronic data among different systems—is fueling the desire for
improvements.
“Match rates are difficult to measure.
“The methods in which records are received can
affect match results.
“Different types of healthcare providers vary in
their perspectives on the extent of the problem.
“Effective opportunities exist for organizations
to more accurately link individuals’ health records.”
About $1,950 in medical care costs per patient during a
hospital stay, and $1.5 million annually in denied claims per hospital, are
associated with inaccurate patient identification, reported a survey conducted
by Black
Book Research.
“Patient matching is a fundamental function of being able to get the right records, for the right person, at the right time, so that timely decisions can be made about his or her health. There has to be a mechanism to ensure that you’re actually getting a copy of the records for the right person,” Mariann Yeager (above), CEO of the Sequoia Project told Modern Healthcare. The Sequoia Project advocates for nationwide health information exchange (HIE). (Photo copyright: Value-based Care Summit.)
Why Patient-Matching is Difficult
Respondents to the Pew study reported that challenges to
correctly matching patients with their records include:
Receiving patient records that an organization
did not expect;
Urban health systems serving patients through
multiple sites;
High costs associated with matching solutions;
and
Differences in how organizations capture, use,
and link medical records.
When humans manually input patient data, Mary Elizabeth
Smith could be listed as M.E. Smith or Mary E. Smith or even Liz Smith. Such
data, when filed differently, can result in duplicate records for the same person,
or, as St. Vincent’s found out, patient mismatches that have dire consequences,
Managed Care noted.
“If there’s some kind of error in entering fields (name,
address, date of birth), either when the patient’s coming in or in a previous
entry, the matching can go awry,” Brendan Watkins,
Administrative Director of Enterprise Analytics at Stanford Children’s Health,
told Modern Healthcare.
Patient-Matching Solutions at Clinical Laboratories
Clinical laboratories also have tackled patient-mismatching
and have devised processing software solutions that ensure patients are
correctly identified and matched with the appropriate records and specimens.
Other solutions suggested by respondents to a previous 2018
Pew survey include:
Unique patient
identifier: Adoption of a patient identification number could help matching
efforts, though patients have expressed privacy concerns. The idea is to use
smartphones to validate patient data using digit codes. However, respondents
told Pew, not everyone has a smartphone.
Data
standardization: Respondents said standardization of data elements and
formatting could impact match rates. But agreement on which elements to use for
the match would be needed.
Referential
matching: Healthcare providers could follow the banking industry and use
outside sources, such as credit bureaus, to verify addresses and other data.
Respondents to the Pew survey balked at the cost.
With advancements in technology and interoperability,
medical laboratory leaders and other healthcare leaders may soon be expected to
achieve patient and record match rates of 100%. Pathology laboratories with
EMPIs and other solutions may be well prepared to meet those challenges.
“Pathologists and medical laboratories may have to demonstrate efficiency and effectiveness to stay in the insurer’s networks and get paid for their services
In recent years, Medicare officials have regularly introduced new care models that include quality metrics for providers involved in a patient’s treatment. Now comes news that a national health insurer is launching an innovative cancer-care model that includes quality metrics for medical laboratories and anatomic pathology groups that deliver diagnostic services to patients covered by this program.
Anatomic pathologists and clinical laboratories know that cancer patients engage with many aspects of healthcare. And that, once diagnoses are made, the continuum of cancer care for these patients can be lengthy, uncomfortable, and quite costly. Thus, it will be no surprise that health insurers are looking for ways to lower their costs while also improving the experience and outcomes of care for their customers.
To help coordinate care for cancer patients while simultaneously addressing costs, Humana, Inc., (NYSE:HUM) has started a national Oncology Model-of-Care (OMOC) program for its Medicare Advantage and commercial members who are being treated for cancer, Humana announced in a press release.
What’s important for anatomic pathologists and clinical
laboratories to know is that the program involves collecting performance
metrics from providers and ancillary services, such as clinical laboratory,
pathology, and radiology. These metrics will determine not only if doctors and
ancillary service providers can participate in Humana’s networks, but also if
and how much they get paid.
Anatomic pathologists and medical laboratory leaders will want to study Humana’s OMOC program carefully. It furthers Humana’s adoption of value-based care over a fee-for-service payment system.
How Humana’s OMOC Program Works
According to Modern Healthcare, “Humana will be looking at several measures to determine quality of cancer care at the practices including inpatient admissions, emergency room visits, medications ordered, and education provided to patients on their illness and treatment.”
As Humana initiates the program with the first batch of
oncologists and medical practices across the US, it also will test performance criteria
that anatomic pathologist groups will need to meet to participate in the
insurer’s network and be paid for services.
The insurer’s metrics address access to care, clinical status assessments, and patient education. Physicians can earn rewards for enhancing their patients’ navigation through healthcare, while addressing quality and cost of care, reported Health Payer Intelligence.
“The experience for cancer care is fragmented,” Bryan Loy, MD (above), Corporate Medical Director of Humana’s Oncology, Laboratory, and Personalized Medicine Strategies Group, told Modern Healthcare. Loy is board-certified in anatomic and clinical pathology, as well as hematology. “Humana wants to improve the patient experience and health outcomes for members. We are looking to make sure the care is coordinated.” (Photo copyright: National Lung Cancer Roundtable/American Cancer Society.)
Humana claims its OMOC quality and cost measurements are
effective in the areas of:
inpatient admissions,
emergency room visits,
medical and pharmacy drugs,
laboratory and pathology services, and
radiology.
To help cover reporting and other costs associated with
participation in the OMOC program, Humana is offering physician practices
analytics data and care coordinating payments, notes Modern Healthcare.
“The practices that improve their own performance over a one-year period will see the care coordination fee from Humana increase,” Julie Royalty, Humana’s Director of Oncology and Laboratory Strategies, told Modern Healthcare.
Value-Based Care Programs are Expensive
Due to the cost of collecting data and increasing staff capabilities to meet program parameters, participating in value-based care models can be costly for medical practices, according to Scottsdale, Ariz.-based Darwin Research Group (DRG), which studies emerging payer models.
Some of the inaugural medical practices in the Humana OMOC
include:
Southern Cancer Center, Alabama;
US Oncology Network, Arizona;
Cancer Specialists of North Florida;
Michigan Healthcare Professionals;
University of Cincinnati Physicians Company; and
Center for Cancer and Blood Disorders, Texas.
Other Payers’ Value-Based Cancer Care Programs
“Depending upon which part of the country you’re in,
alternative payment models in oncology are becoming the norm not the exception,”
noted the DRG study. “Humana is a little late to the party.”
Darwin Research added that Humana may realize benefits from
having observed other insurance company programs, such as:
Humana is not the only payer offering value-based cancer care programs. The Centers for Medicare and Medicaid Services (CMS) Oncology Care Model is a five-year model (2016 through 2021) involving approximately 175 practices and 10 payers throughout America (see above). The healthcare networks and insurers have made payment arrangements with their patients for chemotherapy episode-of-care services, noted a CMS fact sheet. (Graphic copyright: Centers for Medicare and Medicaid Services.)
Humana’s Other Special Pay Programs
Humana has developed other value-based bundled payment
programs as well. It has episode-based
models that feature open participation for doctors serving Humana Medicare
Advantage members needing:
total hip or knee joint replacement (available
nationwide since 2018); and
spinal fusion surgery (launched in 2019).
Humana also started a maternity episode-of-care bundled
payment program last year for its commercial plan members.
In fact, more than 1,000 providers and Humana value-based
relationships are in effect. They involve more than two-million Medicare
Advantage members and 115,000 commercial members.
Clearly, Humana has embraced value-based care. And, to
participate, anatomic pathology groups and medical laboratories will need to be
efficient and effective in meeting the payer’s performance requirements, while
serving their patients and referring doctors with quality diagnostic services.
Clinical laboratories could offer services that complement SDH programs and help physicians find chronic disease patients who are undiagnosed
Insurance companies and healthcare providers increasingly consider social determinants of health (SDH) when devising strategies to improve the health of their customers and affect positive outcomes to medical encounters. Housing, transportation, access to food, and social support are quickly becoming part of the SDH approach to value-based care and population health.
For clinical laboratory managers and pathologists this rapidly-developing trend is worth watching. They can expect to see more providers and insurers in their communities begin to offer these types of services to individuals and patients who might stay healthier and out of the hospital as a result of SDH programs. Clinical laboratories should consider strategies that help them provide medical lab testing services that complement SDH programs.
Medical laboratories, for example, could participate by offering
free transportation to patient
service centers for homebound chronic disease patients who need regular
blood tests. Such community outreach also could help physicians identify people
with chronic diseases who might otherwise go undiagnosed.
Anthem Offers Social
Determinants of Health Package
In fact, health benefits giant Anthem, Inc. (NYSE:ANTM) partly attributes its 2019 first quarter 14% increase of Medicare Advantage members to a new “social determinants of health benefits package” comprised of healthy meals, transportation, adult day care, and homecare, according to Forbes.
“Our focus on caring for the whole person is designed to deliver
better care and outcomes, reduce costs, and ultimately accelerate growth,” Gail Boudreaux,
Anthem President and CEO, stated in a call to analysts, Forbes reports.
An Anthem news release states that SDH priorities for payers, providers, and other stakeholders should focus on enhancing individuals’ access to food, transportation, and social support.
In the Anthem news release, which announced the publication of a white paper that “outlines key differences in how individuals and the public perceive social determinants of health,” Jennifer Kowalski (above), Vice President of the Anthem Public Policy Institute stated, “By better understanding how individuals view and talk about social determinants, payers and providers alike can identify new and improved ways to engage with them to more effectively improve their health and wellbeing and the delivery of healthcare.” (Photo copyright: LinkedIn.)
CMS Expands Medicare
Advantage Plans to Include Social Determinants of Health
The Centers for Medicare and Medicaid Services announced that, effective in 2019, Medicare Advantage plans can offer members benefits that address social determinants of health. Medicare Advantage members may be covered for services such as adult day care, meal delivery, transportation, and home environmental services that relate to chronic illnesses.
Humana’s ‘Bold Goal’
Humana, Inc. (NYSE:HUM) calls its SDH focus the BoldGoal. The program aims to improve health in communities it serves by 20% by 2020.
“The social barriers and health challenges that our Medicare Advantage members and others face are deeply personal. This requires us to become their trusted advocate that can partner with them to understand, navigate, and address these barriers and challenges,” said William Shrank, MD, Humana’s Chief Medical Officer, in a news release.
UnitedHealthcare
Investing More than $400 Million in Housing
Meanwhile, since 2011, UnitedHealthcare (NYSE:UNH) also has invested in affordable housing and social determinants of health, Health Payer Intelligence reported.
In a news release, UnitedHealthcare, the nation’s largest health insurer, described how it is investing more than $400 million in 80 affordable US housing communities, including:
$12 million, PATH Metro Villas, Los Angeles;
$11.7 million, Capital Studios, Austin;
$14.5 million allocated to Minneapolis military
veterans housing;
$7.9 million, New Parkridge (in Ypsilanti, Mich.)
affordable housing complex;
$21 million earmarked to Phoenix low- and moderate-income
families needing housing and supportive services;
$7.8 million, Gouverneur Place Apartments, Bronx,
New York; and
$7.7 million, The Vinings, Clarksville, Tenn.
“Access to safe and affordable housing is one of the
greatest obstacles to better health, making it a social determinant that
affects people’s well-being and quality of life. UnitedHealthcare partners with
other socially minded organizations in helping make a positive impact in our
communities,” said Steve Nelson,
UnitedHealthcare’s CEO, in the news
release.
According to the American Hospital Association (AHA) and the Health Research and Educational Trust (HRET), housing, or lack of it, impacts health. In “Housing and the Role of Hospitals,” the second guide in the organizations’ “Social Determinants of Health Series,” AHA and HRET state that 1.48 million people are homeless each year, and that unstable living conditions are associated with less preventative care, as well as the propensity to acquire diabetes, cardiovascular disease, chronic obstructive pulmonary disorder, and other healthcare conditions.
Social determinants of health programs are gaining in
popularity. And as they become more robust, proactive clinical laboratory
leaders may find opportunities to work with insurers and healthcare providers
toward SDH goals to help healthcare consumers stay healthy, as well as reducing
unnecessary hospital admissions and healthcare costs.