Under-resourced British healthcare system faces a record high backlog of care with 5.61 million people in England waiting for hospital-based medical procedures
Healthcare in the United Kingdom (UK) is about to become much more expensive. The UK government has announced plans to substantially increase payroll taxes to fund the surging demand for care due to the COVID-19 pandemic. But that may only be the part of the healthcare-funding iceberg visible above the surface. Below the surface is a healthcare system where wait times for access to many types of care—including cancer diagnoses—are already unacceptable.
Some pathologists and medical laboratory executives in the US who have long questioned healthcare reformers’ desire to introduce an NHS-like single-payer healthcare system in this country will not be surprised to learn that the UK’s notoriously underfunded National Health Service (NHS) is facing a record waitlist for hospital-based medical diagnostic tests and procedures.
Consequently, Reuters reported, the high cost of fighting the COVID-19 pandemic has pushed British Prime Minister Boris Johnson into breaking with election promises and announcing plans to raise payroll taxes to record levels so that more money can be funneled into the struggling government-run healthcare system.
Speaking to lawmakers in the House of Commons, British Prime Minister Boris Johnson (above) acknowledged his tax plan breaks his Conservative Party’s election year pledge to not raise VAT (value-added tax), income, or national insurance taxes. He insists that the COVID-19 pandemic created unprecedented challenges for the national health system. “I accept that this breaks a manifesto commitment, which is not something I do lightly, but a global pandemic was in no one’s manifesto,” he told lawmakers, Reuters reported. (Photo copyright: The Independent.)
5.6M People on Growing NHS Waiting List for Treatments and Procedures
When the COVID-19 pandemic struck the UK in March 2020, the NHS suspended elective surgeries such as hip or knee replacements and cataract removal and postponed many patients’ medical laboratory diagnostic tests.
In “Record 5.6M People in England Waiting for Hospital Treatment,” The Guardian estimated that 1.4 million patients were added to the waiting lists during the pandemic’s first 18 months. More than one-third of the 5.6 million people waiting for care in July 2021 had been on a waitlist for at least 18 months, the paper noted. Since then, the waiting list has grown by 150,000 people per month, as more people who did not seek or could not access NHS treatments during the pandemic returned to their doctors’ offices.
Johnson’s tax hike formula for fixing the record NHS backlog and improving social care for the elderly created shockwaves in the UK’s Conservative Party, which, like the Republican Party in this country, has championed low taxes. But Johnson maintains the government is out of options.
“It would be wrong for me to say that we can pay for this recovery without taking the difficult but responsible decisions about how we finance it,” Johnson told Parliament. “It would be irresponsible to meet the costs from higher borrowing and higher debt,” he added.
But Johnson’s proposal drew the wrath of some members of his own party and provided the opposition Labor Party with ammunition to denounce the prime minister’s leadership during the pandemic.
In “U.K. Is Among First Western Nations to Increase Taxes to Cover COVID-19 Costs,” The Wall Street Journal (WSJ) reported that Labor Party leader Keir Starmer compared Johnson’s tax increases to putting a bandage “on gaping wounds that his party inflicted,” and questioned why they weren’t levied more directly on the rich. The UK government says the wealthiest 14% will pay about half of the extra tax revenues, the WSJ noted.
“This is a tax rise that breaks a promise that the prime minister made at the last election … Read my lips, the Tories can never again claim to be the party of low tax,” Starmer told Reuters.
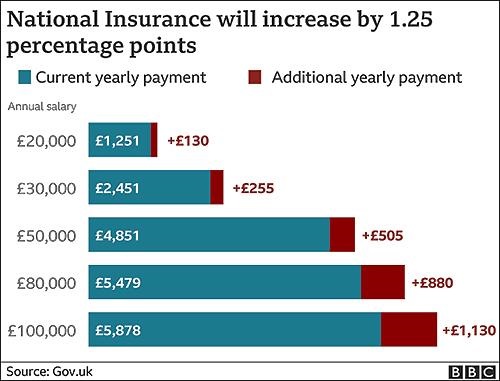
The BBC graphic above illustrates how the tax hikes, which were approved by the Parliament on September 8 by a 319 to 248 vote, will increase the national insurance payroll tax paid by workers and employers by 1.25% each. CNBC reported that the UK government projects the increased taxes will raise £36 billion (US$49.6 billion) over the next three years. (Graphic copyright: BBC.)
Politics versus Hard Facts
According to The Guardian, in 2023-2024, national insurance contributions will be rebranded as a health and social care levy, with more of the money raised going to social care. The added funding will enable the UK government to implement a new cap on total care costs so that no individual will pay more than £86,000 (US$117,142) over their lifetime for social-care programs. Currently, many seniors are forced to sell their homes to meet unexpected care costs, the newspaper noted.
“One message to voters and investors is that taxes are set to rise for years to come,” the WSJ editorial board wrote, predicting the cost of social care will escalate as the UK’s population ages, and that the planned diversion of future taxes for social care will be presented as a “cut” in NHS funding. They maintained that the danger in Johnson’s decision goes deeper than breaking an election campaign pledge or nationalizing more of the UK’s healthcare economy.
“The larger problem is that national healthcare and other entitlements become ever more unaffordable even as they are politically impossible to reform,” the newspaper stated. “The Tories are becoming tax collectors for the entitlement state, which is deadly for parties of the right.”
Bloomberg noted that the UK Institute for Fiscal Studies predicts the planned April 1 tax increase will “raise the UK tax burden to its highest-ever sustained level since records began in 1955—about 35% of national income.”
But, according to the UK-based The Health Foundation, at £2,646.95 (US$3,648.43) per person in 2019, the United Kingdom spends less on healthcare than many developed countries. Less per person than the:
US (£6,782.80),
Germany (£4,131.21),
France (£3,307.54),
Japan (£2,949.19) and
Canada (£2,823.07).
And when healthcare costs are viewed as a percentage of a country’s gross domestic product (GDP), the UK (8% GDP) lags behind the US (13.9%), Germany (9.9%), Japan (9.3%) and France (9.3%) and exceeds only Canada (7.6%) and Italy (6.4%).
While US hospitals, healthcare systems, and patients continue to struggle with ever-increasing healthcare costs, reformers who promote a single-payer healthcare system as an answer to this nation’s healthcare ills may want to take a hard look at the outcomes of the UK’s model.
Clinical laboratory managers and pathologists interested in how the US healthcare system can be improved might be well-served to study the experience of the National Health Service in the UK, that, like all other health systems in the world, has its own unique methods for how it serves its population.
How do you implement a digitization project in your lab? Learn from the success of two organizations.
Produced in partnership with Kapios
In clinical laboratory inspections, instrument maintenance and service visit documentation rank among common deficiencies cited by The Joint Commission, the College of American Pathologists (CAP), COLA, and the Centers for Medicare and Medicaid Services (CMS). While a majority of the time lab techs are diligent about the required maintenance and responsibilities of laboratory equipment, instruments, and analytical systems, the checkoffs are often left to finish later.
No one will dispute that accuracy in clinical lab test result reporting and precision of the total testing process stand paramount in providing quality laboratory services. Those who know the lab environment well would also probably acknowledge that an essential piece of a lab’s defensibility in a challenge is showing proper documentation of laboratory instrument maintenance logs and other required records.
Unfortunately, the reality is such that laboratory managers must run through miles of paper trails looking for evidence of regulatory compliant records of instrument maintenance and other checks.
The goal of this white paper is to demonstrate how some clinical lab directors and technical supervisors sought to relieve the unnecessary labor and hazards in one of the most common analog-world bottlenecks—and were successful. This white paper also identifies three commonly overlooked existing resources for taking the first steps to streamline instrument checks and documentation in the lab today.
Table of Contents
Part 1: Framing a Path to Digitization as Part of the Clinical Laboratory Quality Control Plan
Whether or not large-scale digital transformation of the clinical laboratory is on the immediate horizon or further in the distance, how does the conversion to digitization of lab equipment management processes materialize?
Part 2: Small-scale Digitization Projects: Where, How, and Why Other Labs Made Changes
Some hospital and health system laboratories have transitioned to paperless systems for projects and jobs such as quality assurance (QA) monitors, online quality control (QC) reviews, remote temperature monitoring, and cloud-based document management. Lima Memorial Health System in Lima, Ohio, is one such hospital laboratory operation.
The Dark Intelligence Group is committed to protecting and respecting your privacy, and we’ll only use your personal information to administer your account and to provide the products and services you requested from us. From time to time, we would like to contact you about our products and services, as well as other content that may be of interest to you. In exchange for providing this free content, we may share your information with the companies whose content you choose to view. By accessing the white paper, you’re agreeing to the above.
You can unsubscribe from these communications at any time. For more information on how to unsubscribe, our privacy practices, and how we are committed to protecting and respecting your privacy, please review our Privacy Policy.
Skin patch technologies could enable clinical laboratories to monitor patients’ vitals and report to medical professionals in real time
Pathologists and clinical laboratory leaders have read many Dark Daily ebriefings on the development of skin patches over the years that do everything from monitoring fatigue in the military to being a complete lab-on-skin technology. Now, researchers at the University of California San Diego (UCSD) have developed a wearable patch that can monitor cardiovascular signals and other various biochemical levels in the body simultaneously.
The researchers believe there is enormous potential for such a patch in helping patients monitor conditions such as hypertension or diabetes. They also foresee a scenario where the patch could be used in settings where vitals must be constantly monitored. They hope to develop future versions of the patch that can detect more biomarkers within the body.
“This type of wearable would be very helpful for people with underlying medical conditions to monitor their own health on a regular basis,” Lu Yin, a PhD student and co-first author of the study, told New Atlas. “It would also serve as a great tool for remote patient monitoring, especially during the COVID-19 pandemic when people are minimizing in-person visits to the clinic,” she added.
Combining Precision Medicine with Telehealth and the Internet of Things
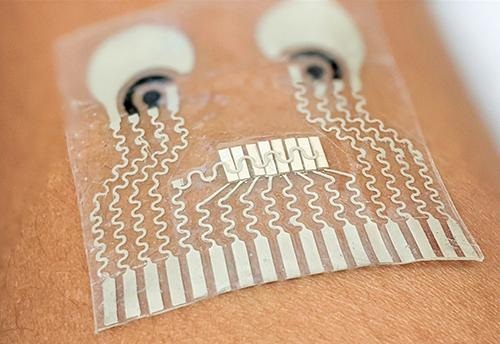
About the size of a postage stamp and consisting of stretchy polymers that conform to the skin, the UCSD patch monitors blood pressure and contains sensors that measure different biochemical levels in the body, such as:
The sensors are carefully arranged on the patch to eliminate interference between the signals, noted a UCSD press release.
In their published research, the UCSD researchers wrote of their new skin patch monitoring device, “Intertwined with concepts of telehealth, the internet of medical things, and precision medicine, wearable sensors offer features to actively and remotely monitor physiological parameters. Wearable sensors can generate data continuously without causing any discomfort or interruptions to daily activity, thus enhancing the self-monitoring compliance of the wearer, and improving the quality of patient care.” (Photo copyright: University of California San Diego.)
“Each sensor provides a separate picture of a physical or chemical change. Integrating them all in one wearable patch allows us to stitch those different pictures together to get a more comprehensive overview of what’s going on in our bodies,” said Sheng Xu, PhD, Principle Investigator, Xu Research Group at UCSD, Assistant Professor in the Department of NanoEngineering Department, and a co-first author of the study, in the press release.
The UCSD researchers developed their skin patch to monitor specific biomarkers that can affect blood pressure.
“Let’s say you are monitoring your blood pressure and you see spikes during the day and think that something is wrong,” co-first author Juliane Sempionatto, PhD, a postdoctoral researcher at California Institute of Technology (Caltech) and co-first author of the study, told New Atlas. “But a biomarker reading could tell you if those spikes were due to an intake of alcohol or caffeine. This combination of sensors can give you that type of information,” she added.
The blood pressure sensor sits near the center of the patch and consists of a set of small transducers welded to the patch via a conductive link. Voltage applied to the transducers send ultrasound waves through the body which bounce off arteries and create echoes that are detected by the sensor and converted into an accurate blood pressure reading.
The chemical sensor releases the drug pilocarpine into the skin to induce sweat and then measures the chemicals contained in the sweat to provide readings of certain biochemical levels.
The glucose sensor located in the patch emits a mild electrical current to the body that stimulates the release of interstitial fluid and then reads the glucose level in that fluid.
“The novelty here is that we take completely different sensors and merge them together on a single small platform as small as a stamp,” Joseph Wang, D.Sc, SAIC Endowed Chair, Distinguished Professor of NanoEngineering, Director of the Center for Wearable Sensors at UCSD, and co-author of the study told New Atlas. “We can collect so much information with this one wearable and do so in a non-invasive way, without causing discomfort or interruptions to daily activity.” (Photo copyright: University of Southern California San Diego.)
Skin Patch Measurements Closely Match Those of Traditional Devices
Test subjects wore the patch on their neck while performing various combinations of the following tasks:
exercising on a stationary bicycle,
eating a high-sugar meal,
drinking an alcoholic beverage, and
drinking a caffeinated beverage.
The results of the measurements taken from the patch closely matched measurements collected by traditional monitoring devices such as a:
For now, the patch must be connected to an external power source which transmits the reading to a counter-top machine, but the researchers hope to create a wireless version in the future.
“There are opportunities to monitor other biomarkers associated with various diseases,” Sempionatto said in the UCSD press release. “We are looking to add more clinical value to this device.”
Other Similar Skin Patch Monitoring Technologies
Though an important breakthrough, the UCSD’s device is not the first skin patch monitor to be developed.
Multiple research and clinical studies are underway that hope to prove the accuracy and safety of wearable devices at detecting and monitoring certain health conditions. It’s a worthy goal.
Skin patches, such as the one created at UCSD, could enable clinical laboratories to provide value-added service to medical professionals and patients alike. Medical labs could potentially monitor skin patch readings in real-time and notify physicians and patients of changes in biomarkers that require attention.
Further, as this technology is developed, it will likely find a ready market with the latest generation of consumers who are more willing than previous generations to buy their own diagnostic tests for home use. These “next-generation” healthcare consumers have demonstrated their willingness to use Apple watches, Fitbits, and similar wearable devices to monitor their condition during exercise and other health metrics.
Pathologists and clinical laboratory managers should not overlook the potential for robust consumer demand to accelerate development and market adoption of such skin patches.
It did not take long for fraudsters to pursue hundreds of billions of federal dollars designated to support SARS-CoV-2 testing and it is rare when federal prosecutors bring cases only a few months after illegal lab testing schemes are identified
As if the COVID-19 pandemic weren’t bad enough, unscrupulous clinical laboratory operators quickly sought to take advantage of the critical demand for SARS-CoV-2 testing and defraud the federal government.
Unfortunately for the many defendants in these cases, federal investigations into alleged cases of fraud were launched with noteworthy speed. As a result of these investigations into alleged healthcare fraud by clinical laboratories and other organizations during fiscal year (FY) 2020, the US Department of Justice (DOJ) announced the US government has recovered $1.8 billion.
The federal prosecutions involved dozens of medical laboratory owners and operators who paid back “hundreds of millions in alleged federal healthcare program losses,” Goodwin Life Sciences Perspectives explained.
When combined with similar efforts starting in prior years, the program has returned to the federal government and private individuals a total of $3.1 billion, the DOJ noted.
“In its 24th year of operation, the program’s continued success confirms the soundness of a collaborative approach to identify and prosecute the most egregious instances of healthcare fraud, to prevent future fraud and abuse, and to protect program beneficiaries,” the report states.
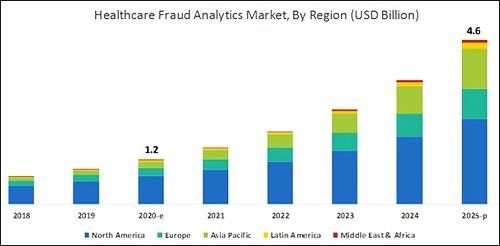
According to the graphic above, which is based on analysis by B2B research company MarketsandMarkets, “North America will dominate the healthcare fraud analytics market from 2020–2025.” As clinical laboratory testing represents a significant portion of the fraud, medical lab managers will want to remain vigilant. (Graphic copyright: MarketsandMarkets.)
COVID-19 Pandemic an Opportunity for Fraud
The HHS report notes that the COVID-19 pandemic required CMS to develop a “robust fraud risk assessment process” to identify clinical laboratory fraud schemes, such as offering COVID-19 tests in exchange for personal details and Medicare information.
“In one fraud scheme, some labs are targeting retirement communities claiming to offer COVID-19 tests but are drawing blood and billing federal healthcare programs for medically unnecessary services,” the HHS report notes.
Still other alleged schemes involved billing for expensive tests and services in addition to COVID-19 testing. “For example, providers are billing a COVID-19 test with other far more expensive tests such as the Respiratory Pathogen Panel (RPP) and antibiotic resistance tests,” the report says.
“Other potentially unnecessary tests being billed along with a COVID-19 test include genetic testing and cardiac panels CPT (current procedural terminology) codes. Providers are also billing respiratory, gastrointestinal, genitourinary, and dermatologic pathogen code sets with the not otherwise specified code CPT 87798,” the report states.
Different Types of Healthcare Organizations Investigated in 2020
Beyond clinical laboratories, the HHS’ 124-page report also shares criminal and civil investigations of other healthcare organizations and areas including:
clinics,
drug companies,
durable medical equipment,
electronic health records,
home health providers,
hospice care,
hospitals and healthcare systems,
medical devices,
nursing home and facilities,
pharmacies, and
physicians/other practitioners.
According to the DOJ, “enforcement actions” in 2020 included:
1,148 new criminal healthcare fraud investigations opened,
440 defendants convicted of healthcare fraud and related crimes,
1,079 civil healthcare fraud investigations opened, and
1,498 pending civil health fraud matters at year-end.
“Federal Bureau of Investigation (FBI) investigative efforts resulted in over 407 operational disruptions of criminal fraud organizations and the dismantlement of the criminal hierarchy of more than 101 healthcare fraud criminal enterprises,” the DOJ reported.
Furthermore, the report said OIG investigations in 2020 led to:
578 criminal actions against people or organizations for Medicare-related crimes,
781 civil actions such as false claims, and
2,148 people and organizations eliminated from Medicare and Medicaid participation.
Implications for Clinical Laboratories
In 2020, OIG issued 178 reports, completed 44 evaluations, and made 689 recommendations to HHS divisions.
Clinical laboratory leaders may be most interested in those related to patient identification as a means to combating fraud and Medicare Part B lab testing reimbursement.
The HHS report says, “Medicare Advantage (MA) encounter data continue to lack National Provider Identifiers (NPIs) for providers who order and/or refer … clinical laboratory services,” adding that, “Almost half of MA organizations believe that using NPIs for ordering providers is critical for combating fraud.”
Additionally, the report states, “Medicare Part B spending for lab tests increased to $7.6 billion in 2018, despite lower payment rates for most lab tests. The $459 million spending increase was driven by:
“increased spending on genetic tests,
“ending the discount for certain chemistry tests, and the
“move to a single national fee schedule.”
Medical laboratory leaders may be surprised to learn that federal healthcare investigators were so vigorous in their investigations, even during the worst of the COVID-19 pandemic.
Vigilance is critical to ensure labs do not fall under the DOJ’s scrutiny. This HHS report, which describes the types and dollars involved in fraudulent schemes by clinical labs and other providers, could help inform revisions to federal compliance regulations and statutes.
Court documents show Holmes’ defense strategy includes accusing ex-boyfriend and former COO Balwani of ‘intimate partner abuse’ that impacted her ‘state of mind’
It has started! The long-awaited criminal trial of former Theranos CEO Elizabeth Holmes is underway in a federal courthouse in Silicon Valley. Across the profession of medical laboratory medicine, there is keen interest in the story of Holmes and her now-defunct clinical laboratory company Theranos.
This next chapter in the drama began on September 8 with opening arguments. Federal prosecutors came out strong, claiming Holmes was “a manipulative fraudster who duped investors and patients alike and knew the whole time that she was hoodwinking them,” according to NPR.
“This is a case about fraud, about lying, and cheating to get money,” said Assistant US Attorney Robert Leach, NPR reported. “It’s a crime on Main Street, and it’s a crime in Silicon Valley,” he added.
Not surprisingly, Holmes’ defense team had a different take, claiming Holmes was simply “a hardworking, young startup executive who believed in the mission of the company, only to see it buckle in the face of business obstacles,” NPR reported. “They argued that she placed blind faith in the No. 2 executive at the company [Balwani] and overly trusted lab directors, who the defense team says were legally responsible for how the labs were run.”
Holmes Claims Abuse at the Hands of Former Theranos COO Balwani
Many pathologists and clinical laboratory managers are ready to watch and learn what unfolds in the opening stages of Holmes’ long-delayed federal criminal fraud trial. During the jury selection process, recently unsealed court documents showed that Holmes’ defense planned to include claims she was abused by her then boyfriend, Theranos Chief Operating Officer Ramesh Balwani.
This surprising development adds yet another twist to the tale of the disgraced Silicon Valley executive and her defunct clinical laboratory testing company.
The hype surrounding the once-high flying startup, which in 2015 reached a peak valuation of $9 billion, began unraveling that same year when a Wall Street Journal (WSJ) investigation exposed the company’s alleged deceptions and questionable practices related to its finger-prick blood-testing technology.
Fast-forward six years—Theranos is now gone but its top executive continues to make headlines, not as a laboratory science wunderkind, but as a criminal defendant.
Holmes, 37, has pleaded not guilty to all charges. Her former consort and ex-Theranos COO Ramesh Balwani also pleaded not guilty to all charges. He will be tried separately from Holmes.
Elizabeth Holmes, founder and former CEO of defunct clinical laboratory testing company Theranos, is seen leaving the Robert F. Peckham US Courthouse with husband William Evans following opening arguments in her federal trial on September 8. (Photo copyright: Reuters/Peter DaSilva.)
Dozens of Potential Jurors Removed for Alleged Bias
On August 31, in-person questioning of prospective jurors began in Holmes’ federal fraud trial in San Jose, California. The process did not go well. As CNBC reported, dozens of potential jurors were removed from the jury pool due to potential bias in the case.
“Thirty to forty of the remaining jurors have consumed substantial, and I mean lengthy extrajudicial material, about the case and about the defendant,” defense attorney Kevin Downey, JD of Washington, D.C.-based Williams and Connolly, LLP, told Judge Edward Davila, CNBC reported. “We’re very vulnerable to any of the jurors commenting in some ways as either the court or lawyers conduct voir dire about the content of the media they’ve seen.”
Voir dire is the legal term for preliminary examinations of jurors, which in this initial screening was done by reviewing potential juror questionnaires.
Holmes’ defense attorneys, according to CNBC, previously expressed concerns about “inflammatory” media coverage of the case. However, Assistant US Attorney Jeffrey Schenk maintained, “Less than half of the individuals that filled out the questionnaire had prior exposure to Holmes and Balwani. One juror saying something during the voir dire process that could be overheard is a risk in every court case,” CNBC reported.
Holmes Claims ‘Mental Condition Bearing on Guilt’
A report by the Independent notes that newly unsealed court documents which were first reported by NPR reveal that Holmes will mount a defense that includes claims of “intimate partner abuse” by Balwani, 56, during their past relationship.
“The documents show that Ms. Holmes will describe how Mr. Balwani controlled what she ate and drank, how she dressed, and who she spoke to, while also alleging he threw ‘sharp’ objects at her,” the Independent reported.
NPR reported that court documents indicate Holmes is likely to take the stand and testify at her trial. She will not be presenting an insanity defense but will put forth a “defense of a mental condition bearing on guilt” that was the result of partner abuse and that impacted her “state of mind” at the time of the alleged crimes.
Court documents filed by Balwani’s defense attorneys label Holmes’ allegations as “salacious and inflammatory.”
“In truth, Ms. Holmes’ allegations are deeply offensive to Mr. Balwani, devastating personally to him and highly and unfairly prejudicial to his defense of this case,” defense attorney Jeffrey Coopersmith, JD, Principle and founder of Coopersmith Law and Strategy, wrote in the filing.
CNBC reported that Holmes gave birth on July 10, 2021, in Redwood, California. The baby’s father is William Evans, heir to the Evans Hotels chain in California, The Sun reported.
Balwani’s criminal fraud trial is scheduled to begin with jury selection on January 11, 2022. Both Holmes and Balwani face maximum penalties of 20 years in jail and a nearly $3 million fine, plus possible restitution if found guilty on all counts.
It is a rare thing for owners of a clinical laboratory company accused of fraud to come to trial and receive so much media attention. In the weeks leading up to the trial, medical laboratory managers and pathologists could read a wide variety of news stories about the impending trial and the legal strategies expected by the attorneys for both the plaintiffs and the defendants.
Thus, everyone interested in this trial and its outcome will likely have the equivalent of a front row seat because so many journalists are covering this trial.