Fear that immunity-resistant mutations of SARS-CoV-2 will emerge are real and the scientific community is paying close attention
Detection of an increasing number of new variants of the SARS-CoV-2 coronavirus raises the possibility that a new strain of COVID-19 might emerge that brings new problems to the management of the pandemic. Public health officials and clinical laboratory scientists are on the alert to determine if any new COVID-19 variant is more virulent or more easily transmissible.
Pathologists, along with the rest of the scientific community worldwide, are following reports of increasing coronavirus mutations with growing concern. The Alpha variant (Lineage B.1.1.7) accounted for most of the COVID-19 cases in April of 2021 in the US, though it was first identified in the United Kingdom. That was followed by the Iota variant (Lineage B.1.526) first identified in New York City. A series of other variants were to follow. Scientists were not surprised. It is normal for viruses to mutate, so they logged and tracked the mutations.
Then, the Delta variant (Lineage B.1.617.2) emerged during a severe outbreak in India. At first, it did not seem more threatening than any other variant, but that changed very quickly. Delta was different.
“The speed with which it dominated the pandemic has left scientists nervous about what the virus will do next. The variant battles of 2021 are part of a longer war, one that is far from over,” The Washington Post reported, which added, “Today, [Delta] has nearly wiped out all of its rivals. The coronavirus pandemic in America has become a Delta pandemic. By the end of July, it accounted for 93.4% of new infections, according to the Centers for Disease Control and Prevention.”
Why is Delta the Worst COVID-19 Variant So Far?
The Delta variant has two advantages that scientists know about:
Stickier spike protein than the spike on the original SARS-CoV-2 coronavirus, as well as on the other, earlier variants. This means that the Delta variant stands a better chance of remaining in a person’s nose or throat long enough to reproduce.
Faster replication. When a virus mutation has more opportunity to reproduce, it quickly becomes the main viral strain. This is the case with the Delta variant. Experts say that the viral load in patients with Delta is around 1,000 times higher than in patients with the original virus.
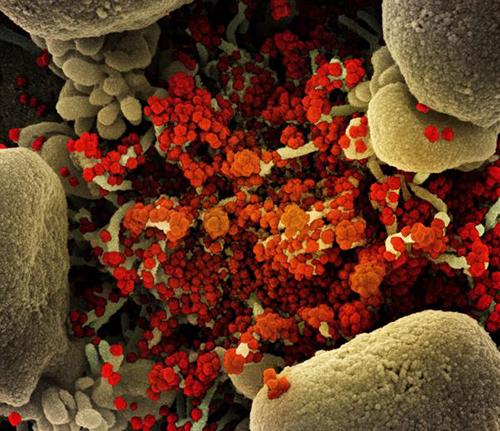
The image above is a “Colorized scanning electron micrograph of an apoptotic cell (tan) heavily infected with SARS-COV-2 virus particles (orange), isolated from a patient sample,” Newsweek reported. (Photo copyright: National Institute of Allergy and Infectious Diseases/Newsweek.)
Will More Dangerous SARS-CoV-2 Variants Appear?
“The great fear is that nature could spit out some new variant that completely saps the power of vaccines and upends the progress we’ve made against the pandemic. But to virologists and immunologists, such a possibility seems very unlikely,” STAT reported.
That is because, unlike Influenza, which is also a coronavirus, SARS-CoV-2 variants are not able to share genetic materials and recombine into deadlier variants. Thus, scientists are skeptical that a variant could appear and wipe out the progress made with vaccines and treatments.
One of the reasons the Flu vaccine changes every year is Influenza’s ability to recombine into variants that can evade immunity. Therefore, scientists are beginning to suspect that SARS-CoV-2, like the Flu, will likely be around for a while.
“I don’t think eradication is on the table. But I think we could come up with something that’s better than what we have for the flu,” Sharone Green, MD, Associate Professor of Medicine, Division of Infectious Diseases and Immunology and Infection Control Officer at University of Massachusetts Medical School, told Newsweek.
Limiting Infections and Replication
Several factors combined to create the COVID-19 pandemic. But SARS-CoV-2 was a novel coronavirus, meaning it was a new pathogen of a known virus. This meant every person on the planet was a potential host.
The situation now is different. Thanks to natural immunity, vaccines, and treatments that shorten the infection, the SARS-CoV-2 coronavirus has less chance to replicate.
“The pressure is there, but the opportunity is not. The virus has to replicate in order to mutate, but each virus doesn’t get many lottery tickets in a vaccinated person who’s infected,” Jeremy Kamil, PhD, Associate Professor of Microbiology and Immunology at LSU Health in Shreveport, La., told STAT.
Tracking Variants of Interest and Variants of Concern
The World Health Organization (WHO) has been monitoring the viral evolution of SARS-CoV-2 since the beginning of the pandemic. In late 2020, the WHO created categories for tracking variants:
VOIs are “A variant with specific genetic markers that have been associated with changes to receptor binding, reduced neutralization by antibodies generated against previous infection or vaccination, reduced efficacy of treatments, potential diagnostic impact, or predicted increase in transmissibility or disease severity.”
Current VOIs include:
Eta (Lineage B.1.525), detected in multiple countries, designated a VOI in March 2021.
Iota (Lineage B.1.526), US, first detected in November 2020, designated a VOI in March 2021.
Lambda (lineage C.37), Peru, first detected in December 2020, designated a VOI in June 2021.
VOCs, on the other hand, demonstrate all the characteristics of VOIs and also demonstrate “an increase in transmissibility, more severe disease (e.g., increased hospitalizations or deaths), significant reduction in neutralization by antibodies generated during previous infection or vaccination, reduced effectiveness of treatments or vaccines, or diagnostic detection failures.”
Current VOCs include:
Alpha (lineage B.1.1.7), first detected in the UK, September 2020.
Delta (lineage B.1.617.2), first detected in India, October 2020.
Will Vaccines Stop Working?
With each new variant, there tends to be a flurry of media attention and fearmongering. That a variant could emerge which would render our current vaccines ineffective has the scientific community’s attention.
“There is intense interest in whether mutations in the spike glycoprotein mediate escape from host antibodies and could potentially compromise vaccine effectiveness, since spike is the major viral antigen in the current vaccines,” wrote Adam S. Lauring, MD, PhD, and Emma B. Hodcroft, PhD, in “Genetic Variants of SARS-CoV-2—What Do They Mean?” published in the Journal of the American Medical Association (JAMA).
“Because current vaccines provoke an immune response to the entire spike protein, it is hoped that effective protection may still occur despite a few changes at antigenic sites in SARS-CoV-2 variants,” they added.
Future events may justify the optimism that the ongoing effectiveness of vaccines will help with many COVID-19 variants. But pathologists and clinical laboratory leaders may want to be vigilant, because as infection rates increase, so do workloads and demands on critical resources in their medical laboratories.
All-of-Us program is free to participants and provides data to more than 800 research studies for cancer, COVID-19, Alzheimer’s, and other diseases; findings will lead to new biomarkers for clinical laboratory tests
It is hard to say no to free. At least that is what the National Institutes of Health (NIH) is counting on to help increase the size and diversity of its database of genetic sequences. The NIH’s All-of-Us Research Program is offering free genetic testing for all participants in the program, as well as free wearable Fitbits for those selected to provide lifestyle and behavior data.
Many pathologists and clinical laboratory managers know that this group of researchers hope to build a database of more than one million genetic sequences to better understand “how certain genetic traits affect underrepresented communities, which could greatly affect the future of customized healthcare,” CBS affiliate 8 News Now reported.
“Customized healthcare” is a euphemism for precision medicine, and genetic sequencing is increasingly playing a key role in the development of personalized diagnostics and therapeutics for cancer and other deadly diseases.
In “VA’s ‘Million Veterans Program’ Research Study Receives Its 100,000th Human Genome Sequence,” Dark Daily described how the NIH’s All-of-Us program was launched in 2018 to aid research into health outcomes influenced by genetics, environments, and lifestyle. At that time, the program had biological samples from more than 270,000 people with a goal of one million participants.
Matthew Thombs, Senior Project Manager of Digital Health Technology at Scripps Research in La Jolla, Calif., joined the All-of-Us program after losing a family member “to a condition I believe could have been managed with changes to their lifestyle,” he told 8 News Now.
“What we are building will empower researchers with the information needed to make such conclusions (about possible need to change lifestyles) and forever alter how diseases are treated,” he added. “I hope that what we are doing here will help my son grow up in a world where healthcare is more of a priority, and many of the ailments we see today are things of the past.”
Such genetic testing could discover biomarkers for future personalized clinical laboratory diagnostics and drug therapies, a key aspect of precision medicine.
The photo above shows an All-of-Us participant being prepped to provide a biological sample for genetic testing. According to Matthew Thombs, Senior Project Manager of Digital Health Technology at Scripps Research, “participants can provide as much or as little information as they like, every single data point matters.” The collected data is shared anonymously with more than 800 research studies for COVID-19, Alzheimer’s, cancer, and other diseases, 8 News Now reported. (Photo copyright: KLAS-TV.)
Scripps Research Integrates Mobile Health Technology into All-of-Us Program
A critical aspect of the NIH’s research is determining how people’s behavior combined with their genetics may predispose them to certain diseases. Nonprofit research institution Scripps Research is working with the NIH’s All of Us Research Program to enroll and collect biological samples from one million US residents.
In addition, Scripps is fitting study participants with wearable mobile health devices to capture data on their habits and lifestyles.
“Until now, the treatment and prevention of disease has been based on a ‘one-size-fits-all’ approach, with most therapeutics tailored for the ‘average patient’. However, advances in genomic sequencing, mobile health technologies, and increasingly sophisticated informatics are ushering in a new era of precision medicine. This new approach takes into account differences in people’s genes, environment, and lifestyles giving medical professionals resources to design targeted treatments and prevention strategies for the individual,” Scripps states on its website.
Can wearable fitness devices and related data contribute to research on genetics and healthcare outcomes? Scripps aims to find out. It has fitted 10,000 people in the All-of-Us program with Fitbit devices (Fitbit Charge 4 tracker or Fitbit Versa 3 smartwatch) at no cost. Since February, Scripps has distributed 10,000 Fitbit wearable devices through the All-of-Us program.
“By sharing information about their health, habits, and environment, participants will help researchers understand why people get sick or stay healthy,” the Scripps website adds.
The Scripps researchers plan to analyze how the people use the wearable devices. They are also accumulating data about participants’ physical activity, heart rate, sleep, and other health metrics and outcomes “as part of the broader All of Us program,” a Scripps news release explained.
“This is the first time All of Us is distributing devices to participants. Our goal is to better understand how participants engage during research studies in order to continually improve user experience and participation. We also expect to learn more about how wearable data may inform the personalization of healthcare,” said Julia Moore Vogel, PhD, Director of The Participant Center at the All of Us Research Program at Scripps Research, in the news release.
All-of-Us Program Records ‘Significant Progress in Participant Diversity’
As of June, the NIH has enrolled 386,000 participants into the All-of-Us program, with 278,000 consenting to all of the program’s steps. Eighty percent of biological samples in the collection are from people in communities that have been under-represented in previous biomedical research an NIH new release noted. According to the NIH, that gives the All-of-Us research program “the most diverse dataset.”
What will all this research ultimately bring to clinical laboratories? Who knows? Nevertheless, if federal institutions like the NIH and non-profit research companies like Scripps believe precision medicine is worth investing in, then the All-of-Us program is worth watching.
A diverse database of a million genetic sequences combined with lifestyle and behavioral data may lead to new and improved personalized diagnostics and drug therapies.
The rapid diagnostic test costs less than $5 per unit and can be adapted for other diseases, the developers say, which opens a slew of possibilities for clinical laboratories
Just as the SARS-CoV-2 coronavirus spurred deployment of new vaccine technology based on messenger RNA (mRNA), the COVID-19 pandemic also could prove to be a watershed for in vitro diagnostics (IVD) innovation in ways that benefit clinical laboratories.
A Penn Medicine news release noted that “The RAPID technology … transforms the binding event between the SARS-CoV-2 viral spike protein and its receptor in the human body, the protein ACE2 (which provides the entry point for the coronavirus to hook into and infect human cells), into an electrical signal that clinicians and technicians can detect. That signal allows the test to discriminate between infected and healthy human samples. The signal can be read through a desktop instrument or a smartphone.”
Though still in its early stages, the technique potentially offers dramatically lower costs and faster results than traditional RT-PCR (reverse transcription polymerase chain reaction) molecular tests. Moreover, the RAPID technology might be useful for identifying other types of biomarkers and could be the basis for diagnostic tests that help reduce the cost-per-test in medical laboratory testing while providing comparable sensitivity and specificity to existing methodologies.
Clinical trials began on January 5, 2021, and the Penn Medicine researchers say the IVD test technology can be applied to other infectious diseases, which, if proven accurate, would be a boon to clinical laboratory testing.
Diagnostic Test Results in Four Minutes for Less than $5/Test
According to the news release, the RAPID 1.0 (Real-time Accurate Portable Impedimetric Detection prototype 1.0) biosensor test costs less than $5 and can deliver results in four minutes. The researchers reported overall accuracy of 87.1% on (139) nasal swab samples and 90% on (50) saliva samples.
The technology uses electrodes that can be mass-produced at low cost on commercially-available screen printers, the researchers said. Results can be read on electronic devices connected to a PC or smartphone.
RAPID 1.0 (above) is a low-cost COVID-19 diagnostic test developed at the César de la Fuente clinical laboratory at the Perelman School of Medicine University of Pennsylvania in Philadelphia. At less than $5/test, plus the ability to be adapted to other diseases, clinical laboratories performing disease screenings in rural or remote locations may have a new tool in the fight against infections. (Photo copyright: University of Pennsylvania.)
Does Penn Medicine’s RAPID 1.0 Test Replace Traditional RT-PCR Testing?
In their published study, the Penn Medicine researchers cited the need for “fast, reliable, inexpensive, and scalable point-of-care diagnostics.”
RT-PCR tests, they said, “are limited by their requirement of a large laboratory space, high reagent costs, multistep sample preparation, and the potential for cross-contamination. Moreover, results usually take hours to days to become available.”
Researchers who have studied the SARS-CoV-2 coronavirus know that it uses a spike-like protein to bind to angiotensin-converting enzyme 2 (ACE2) receptors on the surfaces of human cells.
As described in Penn Medicine’s published study, the biosensor contains ACE2 and other biochemical agents anchored to an electrode. When the SARS-CoV-2 coronavirus attaches to the ACE2, the biosensor transforms the chemical reaction into an electrical signal that can be measured on a device known as a potentiostat.
The researchers tested their RAPID 1.0 technology with two commercially available potentiostat models:
The researchers initially developed the electrode as a printed circuit board, which is relatively expensive. To reduce costs, they constructed a version that uses filter paper as the main component. The researchers noted that one screen printer in a lab can produce 35,000 electrodes per day, including time needed to incorporate the chemical elements. “However, it must be noted that these steps can be fully automated into a production line for industrial purposes, drastically reducing time requirements,” they wrote.
The test can be performed at room temperature, they added, and total cost per unit is $4.67. Much of that—$4.50—is for functionalizing the ACE2 recognition agent. The cost for the bare electrode is just seven cents.
“The overall cost of RAPID may be further reduced through recombinant production of ACE2 and ACE2 variants,” the researchers said, adding that the RAPID 1.0 test can detect the SARS-CoV-2 coronavirus at low concentrations correlating to the earliest stages of the COVID-19 disease.
The Penn Medicine research team was led by César de la Fuente, PhD (above), an Assistant Professor in Psychiatry, Microbiology, Chemical and Biomolecular Engineering and Bioengineering at the Perelman School of Medicine. “Prior to the pandemic, our lab was working on diagnostics for bacterial infections,” he said in the Penn Medicine news release. “But then, COVID-19 hit. We felt a responsibility to use our expertise to help—and the diagnostic space was ripe for improvements.” (Photo copyright: University of Pennsylvania.)
Testing Penn Medicine’s RAPID 1.0 Test
The researchers evaluated the technology in blinded tests with clinical samples from the Hospital of the University of Pennsylvania. The evaluation included 139 nasal swab samples, of which 109 were determined to be COVID-19 positive by RT-PCR tests and clinical assessments. Among these, the RAPID test successfully detected the SARS-CoV-2 coronavirus in 91 samples, for a sensitivity rate of 83.5%. One sample was from a patient diagnosed with the highly contagious SARS-CoV-2 Alpha variant B.1.1.7, which the test correctly identified as positive.
Among the 30 samples determined to be COVID negative, the RAPID test scored a specificity rate of 100%, meaning no false positives. Overall accuracy, including sensitivity and specificity, was 87.1%.
The researchers also analyzed 50 saliva samples: 13 COVID-positive and 37 COVID-negative. The test correctly identified all 13 positive samples but produced five false-positives among the 37 negative samples, for a specificity rate of 86.5%. The researchers speculated that this could be due to interactions between ACE2 and other biomolecules in the saliva but suggested that performance “will improve when using fresh saliva samples at the point-of-care.”
Are There Other Applications for the RAPID Test?
The Penn Medicine news release said the RAPID technology can be adapted to detect other viruses, including those that cause Influenza and sexually-transmitted diseases.
Robert Michel, Editor-in-Chief of Dark Daily and its sister publication The Dark Report, said the test points to one silver lining in the COVID-19 pandemic. “Researchers around the world intensified their work to find ways to identify the SARS-CoV-2 virus that are faster, cheaper, and more accurate than the diagnostic technologies that existed at the time of the outbreak. In this regard, the COVID-19 pandemic may have accelerated the development and refinement of useful diagnostic technologies that will disrupt long-established methods of testing.”
Marcelo Der Torossian Torres, PhD, postdoctoral researcher at Penn Medicine and lead author of the study, said in the news release, “Quick and reliable tests like RAPID allow for high-frequency testing, which can help identify asymptomatic individuals who, once they learn they are infected, will stay home and decrease spread.
“We envision this type of test being able to be used at high-populated locations such as schools, airports, stadiums, companies—or even in one’s own home,” he added.
Clinical laboratory managers may want to stay current on the development and possible commercialization of the RAPID 1.0 (Real-time Accurate Portable Impedimetric Detection prototype 1.0) biosensor test by the research team at Penn Medicine.
Four International Pandemics That Occurred Prior to COVID-19 and Contributed to Increased Clinical Laboratory Testing to Aid in Managing the Outbreaks
Since 1900, millions have died worldwide from previous viruses that were as deadly as SARS-CoV-2. But how much do pathologists and clinical laboratory scientists know about them?
SARS-CoV-2 continues to infect populations worldwide. As of May 28, 2021, the World Health Organization (WHO) reported that 168,599,045 people have been diagnosed with COVID-19 infections globally, and 3,507,377 individuals have perished from the coronavirus.
At the same time, federal Centers for Disease Control and Prevention (CDC) statistics show there have been 33,018,965 cases of COVID-19 in the United States, 589,547 of which resulted in death.
But COVID-19 is just the latest in a string of pandemics that spread across the planet in the past century. Since 1900, there have been four major international pandemics resulting in millions of deaths. But how many people even remember them? And how many pathologists, microbiologists, and clinical laboratory scientists working today experienced even the most recent of these four global pandemics?
Here is a summary/review of these major pandemics to give clinical laboratory professionals context for comparing the COVID-19 pandemic to past pandemics.
Spanish Flu of 1918
The 1918 influenza pandemic, commonly referred to as the Spanish Flu, was the most severe and deadliest pandemic of the 20th century. This pandemic was caused by a novel strand of the H1N1 virus that had avian origins. It is estimated that approximately one third of the world’s population (at that time) became infected with the virus.
According to a CDC article, the flu pandemic of 1918 was responsible for at least 50 million deaths worldwide, with about 675,000 of those deaths occurring in the United States. This pandemic had an unusually high death rate among healthy individuals between the ages of 15 and 34 and actually lowered the average life expectancy in the United States by more than 12 years, according to a CDC report, titled, “The Deadliest Flu: The Complete Story of the Discovery and Reconstruction of the 1918 Pandemic Virus.”
Interestingly, experts feel the 1918 flu strain never fully left us, but simply weakened and became less lethal as it mutated and passed through humans and other animals.
“All those pandemics that have happened since—1957, 1968, 2009—all those pandemics are derivatives of the 1918 flu,” he told The Washington Post. “The flu viruses that people get this year, or last year, are all still directly related to the 1918 ancestor.”
1957 Asian Flu
The H2N2 virus, which caused the Asian Flu, first emerged in East Asia in February 1957 and quickly spread to other countries throughout Asia. The virus reached the shores of the US by the summer of 1957, where the number of infections continued to rise, especially among the elderly, children, and pregnant women.
Between 1957-1958, the Asian Flu spread across the planet causing between one to two million deaths, including 116,000 deaths in the US alone. However, this pandemic could have been much worse were it not for the efforts of microbiologist and vaccinologist Maurice Hilleman, PhD, who in 1958 was Chief of the Department of Virus Diseases at Walter Reed Army Medical Center.
Concerned that the Asian flu would wreak havoc on the US, Hilleman—who today is considered the father of modern vaccines—researched and created a vaccine for it in four months. Public health experts estimated the number of US deaths could have reached over one million without the fast arrival of the vaccine, noted Scientific American, adding that though Hilleman “is little remembered today, he also helped develop nine of the 14 children’s vaccines that are now recommended.”
During his lifetime, Maurice Hilleman, PhD (above), developed a staggering 40 vaccines to help prevent everything from measles, mumps, rubella, pneumonia, meningitis, hepatitis A and B, and other infectious diseases. (Photo copyright: Scientific American.)
1968 Hong Kong Flu
The 1968 influenza pandemic known as the Hong Kong flu emerged in China and persisted for several years. Within weeks of its emergence in the heavily populated Hong Kong, the flu had infected more than 500,000 people. Within months, the highly contagious virus had gone global.
According to the Encyclopedia Britannica, this pandemic was initiated by the influenza A subtype H3N2 virus and is suspected to have evolved from the viral strain that caused the 1957 flu pandemic through a process called antigenic shift. In this case, the hemagglutinin (H) antigen located on the outer surface of the virus underwent a genetic mutation to manufacture the new H3 antigen. Persons who had been exposed to the 1957 flu virus seemed to retain immune protection against the 1968 virus, which, Britannica noted, could help explain the relative mildness of the 1968 outbreak.
It is estimated that the 1968 Hong Kong Flu killed one to four million people worldwide, with approximately 100,000 of those deaths occurring in the US. A vaccine for the virus was available by the end of 1968 and the outbreaks appeared to be under control the following year. The H3N2 virus continues to circulate worldwide as a seasonal influenza A virus.
2009 H1N1 Swine Flu
In the spring of 2009, the novel H1N1 influenza virus that caused the Swine Flu pandemic was first detected in California. It soon spread across the US and the world. This new H1N1 virus contained a unique combination of influenza genes not previously identified in animals or people. By the time the World Health Organization (WHO) declared this flu to be a pandemic in June of 2009, a total of 74 countries and territories had reported confirmed cases of the disease. The CDC estimated there were 60.8 million cases of Swine Flu infections in the US between April 2009 and April 2010 that resulted in approximately 274,304 hospitalizations and 12,469 deaths.
This pandemic primarily affected children and young and middle-aged adults and was less severe than previous pandemics. Nevertheless, the H1N1 pandemic dramatically increased clinical laboratory test volumes, as Dark Daily’s sister publication, The Dark Report, covered in “Influenza A/H1N1 Outbreak Offers Lessons for Labs,” TDR June 8, 2009.
“Laboratories in the United States experienced a phenomenal surge in specimen volume during the first few weeks of the outbreak of A/H1N1. This event shows that the capacity in our nation’s public health system for large amounts of testing is inadequate,” Steven B. Kleiboeker, DVM, PhD, told The Dark Report. At that time Kleiboeker was Chief Scientific Officer and a Vice-President of ViraCor Laboratories in Lee’s Summit, Mo.
1.7 Million ‘Undiscovered’ Viruses
As people travel more frequently between countries, it is unlikely that COVID-19 will be the last pandemic that we encounter. According to the World Economic Forum (WEF), there are 1.7 million “undiscovered” viruses that exist in mammals and birds and approximately 827,000 of those viruses have the ability to infect humans.
Thus, it remains the job of pathologists and clinical laboratories worldwide to remain ever vigilant and prepared for the next global pandemic.
Outspoken Wecht wants readers to understand ‘the multifaceted challenges of the interface of law and medicine’
Pathologists will recognize the name of nationally-acclaimed forensic pathologist Cyril Wecht, MD, JD, who for more than a half-century has been at the center of many of the country’s highest-profile civil and criminal cases. Thus, Dark Daily readers will be intrigued to learn the so-called “godfather of forensic pathology” has published a memoir that takes readers behind the scenes of many of his most controversial forensic pathology cases.
In his recently published memoir (above), forensic pathologist Cyril Wecht, MD, JD, offers readers an inside look at some of his most controversial cases, as well as a defense of his own brushes with the legal system. Anatomic and clinical pathologists may be especially intrigued by Wecht’s description of how “he was acquitted on charges of personally profiting from his office as Allegheny County Coroner” during a federal public corruption charge that was dismissed in 2008, the book’s description states. (Photo copyright: Exposit Books.)
A ‘No-Holds-Barred’ Account
According to TribLIVE, the book—written by Wecht and award-winning writer/filmmaker Jeff Sewald—is a “no-holds-barred account” of Wecht’s personal and professional life. Among the more interesting tidbits are details regarding Wecht’s 1972 discovery that JFK autopsy materials and specimens had gone missing.
“They had been in the government’s possession, so nobody could have touched them, but now the metal container which has held John Kennedy’s brain in formalin was no longer on the list of contents. In addition, various photographs and microscopic tissue slides were also no longer listed. The President’s brain was missing!” wrote Wecht, who argued Lee Harvey Oswald did not act alone in killing JFK and may not have fired the shots that killed him.
In 2006, Wecht faced an 84-count federal public corruption trial, which resulted in him resigning as Alleghany, Pa. medical examiner, the Pittsburgh Post-Gazette reported. In his memoir, Wecht wrote extensively about his public corruption trial. TribLIVE noted Wecht “expresses particular disgust” over the accusation that he supplied Pittsburgh’s Carlow University with cadavers in exchange for use of their laboratory space for his own practice. His trial ended in a hung jury.
“The body-snatching issue was seized upon by the media and was the subject of some of the most horrible cartoons ever,” Wecht wrote. “What made them especially horrible was the fact that I believe anti-Semitism was at their core. They made me look wicked and shadowy, like a ‘Shylock’ who was willing to stoop as low as selling human corpses for a handful of shekels. It was sickening.”
Wecht became known nationally through media appearances and his many decades of work as a medical-legal consultant in civil and criminal cases. At the 2000 Forensic Science and the Law Conference, television host and political commentator Geraldo Rivera, JD, stated, “I’ve known Cyril Wecht for most of my 30-year broadcasting career, and my respect for him has only grown over the decades. His skills as an attorney, as a pathologist, as a medical examiner are legendary.
“Dr. Wecht has guided my audiences through our coverage of crimes ranging from the Kennedy assassination to the O.J. Simpson trial to the JonBenet Ramsey murder mystery,” Rivera added. “And whether or not my audiences knew it, they were getting an education in forensic science—and a lesson in how medical science is applied to this country’s criminal laws.”
An ‘Expert’ and an ‘Irritant’
Though also certified in anatomic pathology and clinical pathology, Wecht has spent his career as a forensic pathologist focused on determining the cause of death. He has performed approximately 17,000 autopsies and has supervised, reviewed, or been consulted on approximately 30,000 additional postmortem examinations, the Cyrilwecht.com website states.
Cyril Wecht, MD, JD (above), told the Pittsburgh Jewish Chronicle that he wrote this memoir so readers could understand the “… complexity and the multifaceted challenges of the interface of law and medicine, specifically in the realm of pathology, and how important it is for justice to be served, with the input from forensic science, and how the system can be subverted, perverted, suppressed, and manipulated.” (Photo copyright: Pittsburg Business Times.)
Pathologists who followed Wecht’s career may know of his reputation “as both an expert and an irritant,” noted the Pittsburg Post-Gazette. For his part, Wecht stated, “If I had been a bit more diplomatic and patient, and a little less antagonistic and controversial, I might have achieved more,” the newspaper reported.
Anyone interested in forensic pathology will likely enjoy reading the behind-the-scenes stories from Wecht’s more than six decades of work. But Wecht’s memoir should be particularly intriguing and informative for clinical and anatomic pathologists, as well as all medical laboratory scientists.