Data was used to create a transmission map that tracked the spread of infections among school athletes and helped public health officials determine where best to disrupt exposure
Genomic sequencing played a major role in tracking a SARS-CoV-2 outbreak in a Minnesota school system. Understanding how and where the coronavirus was spreading helped local officials implement restrictions to help keep the public safe. This episode demonstrates how clinical laboratories that can quickly sequence SARS-CoV-2 accurately and at a reasonable cost will give public health officials new tools to manage the COVID-19 pandemic.
Officials in Carver County, Minn., used the power of genomic epidemiology to map the COVID-19 outbreak, and, according to the Star Tribune, revealed how the B.1.1.7 variant of the SARS-CoV-2 coronavirus was spreading through their community.
“The resulting investigation of the Carver County outbreak produced one of the most detailed maps of COVID-19 transmission in the yearlong history of the pandemic—a chart that looks like a fireworks grand finale with infections producing cascading clusters of more infections,” the Star Tribune reported.
Using genetic sequencing, the Minnesota Department of Health produced the above map of the spread of the COVID-19 through Carver County’s schools. The animated graph includes epidemiological data from “10 high school teams, 10 club teams, 12 teams in a sports association, and three fitness/rec centers.” According to the Star Tribune, “The cluster shows a high ‘attack rate’ of infected people spreading the virus to multiple close contacts. Genomic sequencing found the more infectious B.1.1.7 variant of the virus in about a quarter of cases so far.” Click here to access the interactive version of the map. To see details about specific persons and locations, tap or hover over each dot. (Graphic copyright: Minnesota Department of Health/Star Tribune.)
Private Labs, Academic Labs, Public Health Labs Must Work Together
For gene sequencing to guide policy and decision making as well as it did in Carver County, coordination, cooperation, and standardization among public, private, and academic medical laboratories is required. Additionally, each institution must report the same information in similar formats for it to be the most useful.
“Maintain Policies That Slow Transmission: Variants will continue to emerge as the pandemic unfolds, but the best chance of minimizing their frequency and impact will be to continue public health measures that reduce transmission. This includes mask mandates, social distancing requirements, and limited gatherings.
“Prioritize Contact Tracing and Case Investigation for Data Collection: Cases of variants of concern should be prioritized for contact tracing and case investigation so that public health officials can observe how the new variant behaves compared to previously circulating versions.
“Develop a Genomic Surveillance Strategy: To guide the public health response, maximize resources, and ensure an equitable distribution of benefits, the US Department of Health and Human Services (HHS) should develop a national strategy for genomic surveillance to implement and direct a robust SARS-CoV-2 genomic surveillance program, drawing on resources and expertise from across the US government.
“Improve Coordination for Genomic Surveillance and Characterization: There are several factors in creating a successful genomic surveillance and characterization network. Clear leadership and coordination will be necessary.”
Practical Application of Genomic Sequencing
Genomic epidemiology uses the genetic sequence of a virus to better understand how and where a given virus is spreading, as well as how it may be mutating. Pathologists understand that this information can be used at multiple levels.
Locally, as was the case in Carver County, Minn., it helps school officials decide whether to halt sports for a time. Nationally, it helps scientists identify “hot spots” and locate mutations of the coronavirus. Using this data, vaccine manufacturers can adjust their vaccines or create boosters as needed.
“This is some of the most amazing epidemiology I’ve ever seen,” epidemiologist Michael Osterholm, PhD, Regents Professor, and Director of the Center for Infectious Disease Research and Policy (CIDRAP) at the University of Minnesota, told the Star Tribune, which reported that “A public health investigation linked 140 COVID-19 cases among more than 50 locations and groups, mostly schools and sports teams in Carver County. (Photo copyright: University of Minnesota.)
Will Cost Decreases Provide Opportunities for Clinical Laboratories?
Every year since genomic sequencing became available the cost has decreased. Experts expect that trend to continue. However, as of now, the cost may still be a barrier to clinical laboratories that lack financial resources.
“Purchasing laboratory equipment, computer resources, and staff training requires significant up-front investments. However, the cost per sequence is far less today than it was under earlier methods,” the GAO noted. This is good news for public and independent clinical laboratories. Like Carver County, a significant SARS-CoV-2 outbreak in the future may be averted thanks to genetic sequencing.
“The first piece of the cluster was spotted in a private K-8 school, which served as an incubator of sorts because its students live in different towns and play on different club teams,” the Star Tribune reported.
Finding such clusters may provide opportunities to halt the outbreak. “We can try to cut it off at the knees or maybe get ahead of it,” epidemiologist Susan Klammer with Minnesota Public Health and for childcare and schools, told the Star Tribune.
This story is a good example of how genomic sequencing and surveillance tracking—along with cooperation between public health agencies and clinical laboratories—are critical elements in slowing and eventually halting the spread of COVID-19.
Though pathology salaries rank 16th among 29 medical specialties, it is in the top 10 among specialties that attract women and respondents say that comes with a lot of paperwork
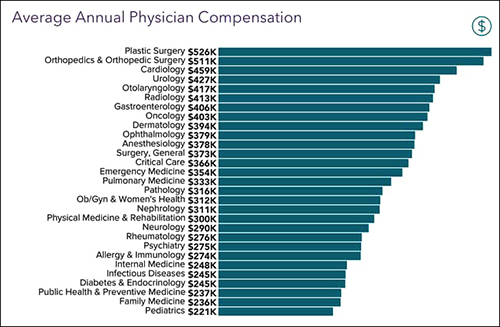
Despite “hardships” brought on by the COVID-19 pandemic, 18,000 physicians in more than 29 medical specialties who participated in Medscape’s 2021 Physician Compensation Report said that, overall, their 2020 income was similar to prior years. Pathologists reported earnings in 2020 of $316,000, $28,000 below the average specialist’s salary of $344,000.
The average pathologist’s salary ranked 16th among medical specialty salaries.
Compared to 2019, medical specialists on average made $2,000 less in 2020. The average salary for primary care doctors was $242,000 in 2020, down $1,000 from 2019, according to a Medscapenews release.
“Physicians experienced a challenging year on numerous fronts, including weathering the volatile financial impact of lockdowns,” said Leslie Kane, Senior Director, Medscape Business of Medicine, in the news release. “Our report shows that many were able to pivot to use telemedicine and focus on tactics that would protect their practices.”
Medscape, a health information provider that is part of the WebMD network, said that in addition to telehealth, doctors turned to MACRA (Medicare Access and CHIP Reauthorization Act of 2015) value-based payment reward programs and other strategies to minimize the effects of office closures last year.
“COVID took a terrible emotional toll on physicians and healthcare workers, and many are still struggling financially, but our findings showed that physicians will innovate and change quickly to meet the needs of patients through extremely difficult times,” said Leslie Kane (above), Senior Director, Medscape’s Business of Medicine, in the news release. Pathologists who were at the center of the nation’s COVID-19 pandemic response would likely echo her sentiments. (Photo copyright: Medscape.)
Pathology Salary Unchanged
To complete its study, Medscape asked physicians to take a 10-minute online survey. The reported findings included responses from 17,903 physicians (61% male, 36% female) practicing in more than 29 specialties between October 2020 and February 2021.
Pathologists who participated in the survey reported no change in their annual salary since 2019. Other specialties that reported no salary change include:
Family medicine,
Infectious diseases,
Ophthalmology, and
Orthopedics/orthopedic surgery.
Top 10 Medical Specialty Salaries
Medscape’s report listed these top-10 medical specialties as earning the highest salaries (see the graphic below for the full list of medical specialties surveyed):
Contrary to what many specialists reported, plastic surgeons did not experience slowdowns in appointments during the COVID-19 pandemic. In fact, not only did plastic surgeons earn the most, at 10% they are the medical specialists who got the biggest increase in pay of previous years as well.
According to the American Academy of Facial Plastic and Reconstructive Surgery (AAFPRS), which conducted its own salary survey of its member surgeons, “70% of AAFPRS surgeons report an increase in bookings and treatments over the course of the COVID-19 pandemic, with nine in 10 facial plastic surgeons indicating an increase of more than 10%. Surgical procedures are the most common procedures as part of this upsurge, perhaps cancelling out any decreases that might have resulted from the economic crisis and lockdowns.”
Other specialist salaries which Medscape found increased in 2020 include:
Oncology: up 7%
Rheumatology and cardiology: up 5%
Diabetes/endocrinology: up 4%
Neurology, critical care, psychiatry: up 3%
General surgery, urology, public health/preventive medicine: up 2%
Medical specialties that reported reductions in salary included:
Otolaryngology and allergy/immunology: down 9%
Pediatrics and anesthesiology: down 5%
Dermatology: down 4%
Pulmonary medicine, physical medicine, gastroenterology, and radiology: down 3%
Emergency medicine and internal medicine: down 1%
About 92% of physicians surveyed indicated that the COVID-19 pandemic caused their income to decline. Also, 22% of doctors noted they experienced loss of work hours.
Pathologists Received Low Average Bonuses
Reporting on receipt of incentive bonuses, Medscape ranked pathology in the bottom half of its list with $42,000 as an average bonus. The top incentive bonuses went to those practicing:
Orthopedics/orthopedics surgery: $116,000
Ophthalmology: $87,000
Otolaryngology: $72,000
About 59% of primary care physicians and 55% of specialists surveyed reported receiving an incentive bonus.
Pathologists Rank High in Job Satisfaction
In responding to a question about compensation, pathologists ranked near the top (seventh position) with 64% saying they are content with their pay. Others expressing salary satisfaction included:
Oncology: 79%
Psychiatry: 69%
Plastic surgery: 68%
Dermatology: 67%
Public health/preventive medicine: 66%
Radiology: 65%
Pathology: 64%
Pathology Popular Among Women MDs
Medscape found that women MDs chose certain medical specialties more often than others, including pathology, which ranked eighth. The top eight specialties employing female physicians are:
Pediatrics: 61%
Obstetrics/gynecology: 59%
Diabetes/endocrinology: 50%
Family medicine: 47%
Dermatology: 46%
Infectious diseases: 46%
Internal medicine: 44%
Pathology: 43%
Specialties with the fewest female physicians are:
Plastic and general surgery: 20%
Cardiology: 14%
Urology: 11%
Orthopedics/orthopedics surgery: 9%
Pathology a Leader in Paperwork
Medscape also surveyed physicians as to the estimated hours they spend per week on paperwork and administration. Here, pathology ranked the fifth highest with 19%, while radiologists and hospital-based physicians were third from the bottom with 11.6%.
Specialists that reported the highest hours spent on paperwork include:
Amid a trying year, the Medscape survey respondents made an encouraging point: 78% of them said they would choose medicine as a career again. And 85% of pathologists said they would choose the same specialty.
Medscape’s report may be helpful to hospital-based clinical laboratory leaders preparing salary budgets and to pathologists in salary negotiations and determining professional responsibilities.
On top of everything else during this pandemic, drug-resistant infections are threatening the most vulnerable patients in COVID-19 ICUs
New study by researchers at the University of Minnesota highlights the continuing need for microbiologists and clinical laboratories to stay alert for COVID-19 patients with drug-resistant infections. In their study, researchers highlighted CDC statistics about the number of Candida auris (C. auris) infections reported in the United States during 2020, for example.
In a paper, titled, “Three Cases of Worrisome Pan-Resistant C Auris Found in New York,” the Center for Infectious Disease Research and Policy (CIDRAP) at the University of Minnesota reported that “As of Dec 11, the CDC said 941 confirmed and probable C. auris cases have been reported in 13 states, and an additional 1,830 patients have been found to be colonized with the multidrug-resistant fungus. Most of the cases have been detected in the New York City area, New Jersey, and the Chicago area.”
Candida auris is a particularly nasty fungus. It spreads easily, is difficult to remove from surfaces, and can kill. Worst of all, modern drugs designed to combat this potentially deadly fungus are becoming less effective at eradicating it, and COVID-19 ICU patients appear especially vulnerable to C. auris infections.
COVID-19 and C. auris a Potentially Devastating Combination
Hospitals in many areas are at a critical capacity. Thus, hospital-acquired infections such as sepsis can be particularly dangerous for COVID-19 patients. Adding to the problem, C. auris requires special equipment to identify, and standard medical laboratory methods are not always enough. Misidentification is possible, even probable.
A paper in the Journal of Global Antimicrobial Resistance (JGAR), titled, “The Lurking Scourge of Multidrug Resistant Candida Auris in Times of COVID-19 Pandemic,” notes that “A particularly disturbing feature of COVID-19 patients is their tendency to develop acute respiratory distress syndrome that requires ICU admission, mechanical ventilation, and/or extracorporeal membrane oxygenation. … This haunting facet of COVID-19 pandemic has severely challenged even the most advanced hospital settings. Yet one potential confounder, not in the immediate attention of most healthcare professionals, is the secondary transmission of multidrug resistant organisms like the fungus Candida auris in COVID-19 ICUs. … C. auris outbreaks occur in critically ill hospitalized patients and can result in mortalities rates ranging from 30% to 72%. … Both C. auris and SARS-CoV-2 have been found on hospital surfaces including on bedrails, IV poles, beds, air conditioner ducts, windows and hospital floors. Therefore, the standard COVID-19 critical care of mechanical ventilation and protracted ventilator-assisted management makes these patients potentially susceptible to colonization and infections by C. auris.”
One study mentioned in the JGAR paper conducted in New Delhi, India, looked at 596 cases where patients were admitted to the ICU with COVID-19. Fifteen of them had infections caused by C. auris. Eight of those patients died. “Of note, four patients who died experienced persistent fungemia and despite five days of micafungin therapy, C. auris again grew in blood culture,” according to reporting on the study in Infection Control Today (ICT).
Some C. auris mortality rates are as high as 72%. And patients with weakened immune systems are at particular risk, “making it an even more serious concern when 8% to 9% of roughly 530,000 ICU patients in the United States have COVID-19,” ICT reported.
Apparently, the COVID-19 pandemic has created circumstances that are particularly suited for C. auris to spread. “Given the nosocomial transmission of SARS-CoV-2 by those infected, many hospital environments may serve as venues for C. auris transmission as it is a known environmental colonizer of ICUs,” wrote the JGAR paper authors.
CDC Reports and Recommendations
Along with being especially dangerous for people with weakened immune systems, C. auris infections also produce symptoms similar to those of COVID-19, “including fever, cough, and shortness of breath,” according to the CDC’s website. People admitted to ICUs with COVID-19 are especially vulnerable to bacterial and fungal co-infections. “These fungal co-infections are reported with increasing frequency and can be associated with severe illness and death,” says the CDC.
C. auris outbreaks in the United States have mostly been in long-term care facilities, but the pandemic seems to be changing that and more outbreaks have been detected in acute care facilities, the CDC reported. The lack of appropriate personal protective equipment (PPE), changes in infection control routines, and other factors could be to blame for the increase.
Just as community spread is an issue with COVID-19 variants, so too is it a concern with C. auris infections. “New C. auris cases without links to known cases or healthcare abroad have been identified recently in multiple states, suggesting an increase in undetected transmission,” the CDC noted.
As of January 19, 2021, according to the CDC the case count of C. auris infections in the US was 1,625, with California, Florida, Illinois, New Jersey, and New York having more than 100 cases each.
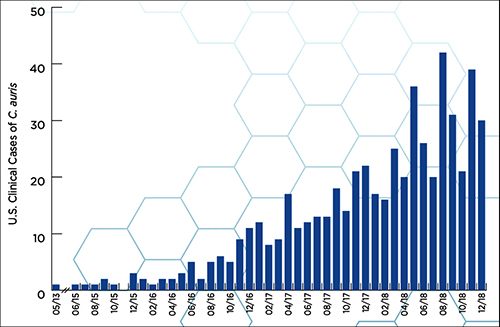
According to a CDC report, “Candida auris (C. auris) is an emerging multidrug-resistant yeast (a type of fungus). It can cause severe infections and spreads easily between hospitalized patients and nursing home residents.” The graphic above, taken from the report, illustrates how “C. auris began spreading in the United States in 2015. Reported cases increased 318% in 2018 when compared to the average number of cases reported in 2015 to 2017.” (Graphic copyright: Centers for Disease Control and Prevention.)
Using Clinical Laboratory Tests to Identify C. Auris
One of the big concerns about C. auris is that it is so difficult to detect, and that medical laboratories in some countries simply do not have the technology and resources to identify and tackle the infection.
“As C. auris diagnostics in resource-limited countries is yet another challenge, we feel that alerting the global medical community about the potential of C. auris as a confounding factor in COVID-19 is a necessity,” wrote the authors of the paper published in the Journal of Global Antimicrobial Resistance.
As if the COVID-19 pandemic has not been enough, drug resistant bacteria, viruses, and deadly fungi are threatening to wreak havoc among SARS-CoV-2 infected patients. Microbiologists and medical laboratory scientists know that testing for all types of infections is vitally important, but especially when it comes to infections caused by antibiotic-resistant bacteria (ARB) and other dangerous organisms that demonstrate antimicrobial resistance (AMR).
Microbiologists and clinical laboratory professionals will want to stay informed about the number of C. auris cases identified in the US and the locations and settings where the fungus was detected. They will want to be on the alert within their hospitals and health networks, as well as with the doctor’s offices served by their labs.
Pathologists and clinical laboratory scientists know that influenza vaccines typically produce short-lived protection and researchers have new clues as to why this is true
With so much interest in development of a COVID-19 vaccine, findings by researchers at Atlanta’s Emory Vaccine Center into why the vaccine for influenza (Flu) is so short-lived offer a new window on how the body’s immune system responds to invading viruses and what happens to the immunity over time.
Because the autumn influenza season is just weeks away, these insights into the body’s immune response to influenza will be of interest to clinical laboratories that provide testing for influenza, as well as SARS-CoV-2, the coronavirus that causes COVID-19.
Clinical laboratory managers recognize that an influenza vaccine is an annual imperative for people—especially the elderly and those with existing comorbidities—and medical laboratory tests are typically used to diagnose the illness and identify which strains of viruses are present. The flu vaccine is even more important amid the COVID-19 pandemic, infectious disease authorities say.
The scientists at the Emory Vaccine Center published their findings in the journal Science.
Not so with influenza vaccines. The immunity they impart generally only lasts for a single flu season and are “lost within one year,” the Emory study notes.
As Genetic Engineering and Biotechnology News (GEN) explains, the influenza genome has eight RNA segments which can change as the virus enters a cell. This antigenic shift creates new influenza strains that require updated vaccines, GEN noted.
However, the Emory researchers stated that “The fact that a small number did persist over one year raises prospects that the longevity of flu vaccines can be improved and provides key information for the development of universal vaccines against influenza.”
Bone Marrow Has Major Role in Producing New Flu Antibodies
The Emory study focused on the influenza vaccine’s role in how it affects the immune system and what needs to change to create a longer-lasting influenza vaccine. “Our results suggest that most bone marrow plasma cells (BMPC) generated by influenza vaccination in adults are short-lived. Designing strategies to enhance their persistence will be key,” the Emory researchers wrote in Science.
The scientists analyzed bone marrow from 53 healthy volunteers (age 20 to 45). An Emory news release states that bone marrow is the “home base for immune cells producing antibodies.”
Besides the bone marrow, the researchers also examined blood samples from the volunteers, all of which was collected between 2009 and 2018:
before influenza vaccination,
one month after influenza vaccination, and
one year post vaccination.
Through DNA sequencing the samples, the Emory researchers found the number of flu-specific cells increased from 0.8% to 1.9% after one month. They concluded that an annual vaccine does increase antibody-producing cells for influenza in bone marrow.
However, in follow-up visits one year after vaccination, they found that the number of cells present in the volunteers had fallen back to the starting point.
“Specific cells produced by the vaccine … produced unique antibodies that can be identified using sequencing techniques,” Carl Davis, PhD, postdoctoral fellow in the Rafi Ahmed Laboratory at Emory and first author of the paper, said in the news release, adding, “We could see that these new antibodies expanded in the bone marrow one month after vaccination and then contracted after one year.”
He continued, “On the other hand, antibodies against influenza that were in the bone marrow before the vaccine was given stayed at a constant level over one year.”
Vaccine Adjuvants Help Boost Immunity
A vaccine additive called an adjuvant could be the answer to extending the power of influenza vaccines, the Emory scientists noted.
“Just getting to the bone marrow is not enough. A plasma cell has to find a niche within the bone marrow and establish itself there and undergo gene expression and metabolism changes that promote longevity,” Rafi Ahmed, PhD, Director of the Emory Vaccine Center, said in the news release.
“It’s totally crazy (that the most commonly used influenza vaccines don’t include an adjuvant), Ahmed told Science. “I’m hoping that things will change in the influenza vaccine world, and 10 years from now, you will not be getting any nonadjuvanted vaccines.”
According to USA Today, about 20-million “essential” workers will likely be the first to receive the new COVID-19 vaccine and participate in check-in text messages with the Centers for Disease Control and Prevention (CDC) by the end of 2020.
In its COVID-19 vaccine testing, Novavax, a late-state biotechnology company, suggests that “an adjuvant is critical to its vaccine working well,” National Public Radio (NPR) reported in “The Special Sauce That Makes Some Vaccines Work.” However, vaccine developers may be reluctant to share their adjuvant research.
“Adjuvants end up being very proprietary. It’s kind of the secret sauce on how to make your protein vaccine work,” Barney Graham, MD, PhD, Deputy Director, Vaccine Research Center, National Institute of Allergy and Infectious Diseases, told NPR.
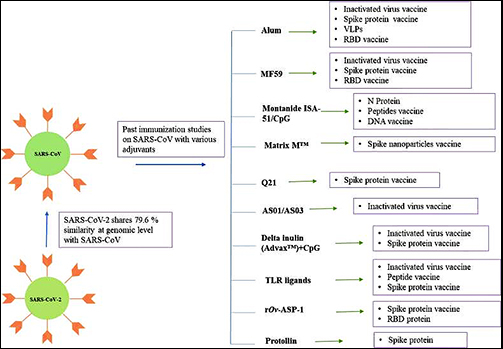
Still, a study published in Immunopharmacology revealed potential adjuvants for the COVID-19 vaccine based on vaccine studies of other coronaviruses. While there are many adjuvants available, not all have safety track records that can be leveraged to gain clearance from regulatory bodies, the researchers pointed out. But some do.
“CpG 1018, MF59, and AS03 are already approved for human vaccine and their inclusion may expedite the vaccine development process. Further, Protollin has shown promising results in pre-clinical studies,” the authors wrote.
Clinical laboratories that provide influenza testing will want to follow these types of research studies. Findings on immunity will affect development of vaccines that medical labs provide—including for COVID-19.