Pathology groups and clinical laboratories experiencing shortages in management positions may want to consider on-demand healthcare leaders
Are “on-demand” leaders the answer to clinical laboratory and pathology group staff shortages? Perhaps. A new twist on management philosophies is gaining steam in hospitals: Hiring on-demand managers and executives to fill gaps in high-level staff. The practice is growing quickly and making its mark.
“[On-demand leadership] is really taking off,” said Adam Burns, Principal, Interim Leadership, at international executive search/leadership consulting firm WittKieffer, in a Newsweek article. “I think it’s something that’s going to be permanent in the industry. Once [health systems] start to think about all the different ways they could use somebody—when you take the org chart out of it and just think about the lists of challenges and projects and opportunities they have—it’s endless.”
Clinical lab administrators and pathologists should note that the trend of on-demand management assignments is distinctly different from the traditional locum tenens and temporary staffing that have been common in healthcare for decades. These arrangements are typically used to engage physicians and laboratory scientists to handle the daily delivery of clinical services. The on-demand management model engages individuals with proven management skills to address specific initiatives and projects that the institution would not otherwise be able to achieve.
Tight finances in many hospitals make hiring on-demand managers for short-term assignments versus long-term permanent positions a cost-effective way to deal with projects that need specific skills to be implemented. Another factor is experienced hospital administrators who retire but then want to return on a limited basis. They have desirable skills, knowledge, and energy worth retaining and on-demand positions may make that possible and affordable.
As hospitals warm up to on-demand engagements, clinical laboratories may also see benefits as the trend widens and gains more acceptance.
“The business challenges in healthcare are getting bigger every year. They’re very high stakes, because people’s lives are at stake,” Sandra Pinnavaia (above), Partner, Global Head, On-Demand Talent Strategy and Innovation at Heidrick and Struggles, told Becker’s Hospital Review. The Chicago-based global executive search and consulting firm has seen a strong increase in hospital placements and notes that healthcare is the “eighth most served industry sector in the US.” Pinnavaia says this growth helps hospitals keep up with “an evolving industry,” of leaning on temporary help. Might clinical laboratories benefit from filling empty leadership positions with on-demand leaders? (Photo copyright: Heidrick and Struggles.)
Who Are On-Demand Executives, What Positions Do They Fill?
According to Becker’s Hospital Review, an on-demand executive is “an independent and established business professional—ranging from the C-suite to the director level, or a management consultant,” who is often brought in to help with specific projects or fill gaps within an organization as needed during transitional times. Most provide temporary support without seeking full-time stability.
Top on-demand positions, Becker’s reported, include:
Financial controls,
Accounting and auditing,
Organizational design and workforce planning, and
Technology and systems implementation.
There has been a steady two-year increase of health systems “looking for senior leaders to solve specific problems rather than to hold specific titles,” Burns told Newsweek.
Occasionally, a “specialized eye” is needed for specific challenges, such as hiring a former Chief Information Security Officer (CISO) to establish an infrastructure that lasts beyond his or her stay, Newsweek noted.
“[Hiring an on-demand leader is] the most cost-effective option,” Burns said. “Organizations compare it to the cost of consulting firms, and when you compare hiring a senior leader in an on-demand capacity to hiring a consulting firm, many times it’s a third or half of the expense.”
Additionally, many hospital systems are still regrouping after the fallout from the COVID-19 pandemic. With all the consolidation that occurred to leadership teams as cost-savings efforts, many “systems lack the bench strength to source special projects from within,” Newsweek added.
Plusses for Hospitals
The benefits are numerous for hospitals according to Burns. “When health systems reflexively look inward for new projects, they can unconsciously build their tolerance for the status quo. On the other hand, a fresh, unbiased perspective can open new doors for the organization. On-demand leaders can make honest recommendations about what is best for the health system, free from internal politics or preexisting expectations,” he told Newsweek.
“The right on-demand leader can create momentum [on a project] without a long-term engagement with our system when there is no definitive construct of what an organization wants a function or role to look like,” Feby Abraham, PhD, Executive Vice President and Chief Strategy Officer at Memorial Hermann Health System in Houston, told Becker’s Hospital Review.
Further, “these roles provide opportunities for leaders with extensive healthcare experience, allow for a faster track to build momentum, and allow for developing a clearer vision for the long-term, full-time version of roles,” he added.
Plusses for On-Demanders
Pinnavaia told Becker’s Hospital Review, “[On-demand executives] are free agents, independent, and available to jump in and out of the organizations they serve, either by providing a proper coverage to a gap, like being an interim leader sitting in a gap, or to the augmentation of injecting skills and experience around a particular topic or movement in the business cycle.”
Burns notes that “numerous factors [are] fueling demand” for on-demand positions, Newsweek reported, adding that “Baby boomers are aging out of senior leadership roles and into retirement, leaving experience gaps in their wake. But after a year of vacationing and pursuing hobbies, many healthcare executives start itching for a new challenge. They become strong candidates for on-demand roles, which allow them to contribute their extensive knowledge without committing to an indefinite seat.”
It’s Not Magic
“This is a growing category, but it’s not magic,” Pinnavaia told Becker’s Hospital Review. “It takes an intermediary that advises both sides of the equation about how to make the project successful, how to structure the project, how to onboard someone, how to really make sure it’s going well. Secondly, it takes talent that has really done this before … it is a learning muscle,” she added.
Abraham agreed. “Many of the challenges revolved around crafting the role description up front, finding the right candidate, and then getting feedback to maximize the impact of that on-demand role itself,” he told Becker’s Hospital Review.
While hospitals warm to the notion of on-demand engagements, this trend may make its way into many clinical laboratories. Readers who work within hospital and healthcare settings should pay close attention. Understanding how these services are being used can provide a proper heads-up of what may come.
Do you have a story to share of your own experience? Hospital and health system laboratories using on-demand management assignments are invited to contact us to share their successes with this approach and the lessons learned.
Shortage could disrupt the ability of clinical laboratories in hospitals and health systems to run certain tests for bloodstream infections
US clinical laboratories may soon experience a “disruption of availability” of BACTEC blood culture media bottles distributed by Becton Dickinson (BD). That’s according to the federal Centers for Disease Control and Prevention (CDC) which issued a Health Alert Network (HAN) Health Advisory to all clinical laboratory professionals, healthcare providers and facility administrators, and other stakeholders warning of the potential shortfall of critical testing supplies.
“This shortage has the potential to disrupt patient care by leading to delays in diagnosis, misdiagnosis, or other challenges in the clinical management of patients with certain infectious diseases,” the CDC stated in the health advisory.
The CDC advises healthcare providers and health departments that use the bottles to “immediately begin to assess their situations and develop plans and options to mitigate the potential impact of the shortage on patient care.”
The advisory notes that the bottles are a key component in continuous-monitoring blood culture systems used to diagnose bloodstream infections and related conditions, such as endocarditis, sepsis, and catheter-related infections. About half of all US laboratories use the BD blood culture system, which is compatible only with the BACTEC bottles, the CDC advisory states.
Infectious disease specialist Krutika Kuppalli, MD (above), Chair of the Infectious Diseases Society of America (IDSA) and a Medical Officer for COVID-19 Health Operations at the World Health Organization, outlined the potential impact of the shortage on healthcare providers and clinical laboratories. “Without the ability to identify pathogens or [their susceptibility to specific antibiotics], patients may remain on broad antibiotics, increasing the risk of antibiotic resistance and Clostridium difficile-associated diarrhea,” she told STAT. “Shortages may also discourage ordering blood cultures, leading to missed infections that need treatment.” (Photo copyright: Loyola University Health System.)
FDA Advises Conservation of Existing BACTEC Supplies
The CDC advisory followed a July 10 notice from the US Food and Drug Administration (FDA) that also warned healthcare providers of “interruptions in the supply” of the bottles. The supply disruption “is expected to impact patient diagnosis, follow up patient management, and antimicrobial stewardship efforts,” the FDA’s letter states. “The FDA recommends laboratories and healthcare providers consider conservation strategies to prioritize the use of blood culture media bottles, preserving the supply for patients at highest risk.”
Hospitals have been warned that the bottle shortage could last until September, STAT reported.
BD issued a press release in which BD Worldwide Diagnostic Solutions President Nikos Pavlidis cast blame for the shortage on an unnamed supplier.
“We understand the critical role that blood culture testing plays in diagnosing and treating infections and are taking all available measures to address this important issue, including providing the supplier our manufacturing expertise, using air shipments, modifying BD manufacturing schedules for rapid production, and collaborating with the US Food and Drug Administration to review all potential options to mitigate delays in supply,” Pavlidis said. “As an additional stopgap measure, our former supplier of glass vials will restart production to help fill the intermittent gap in supply.”
Steps Clinical Laboratories Can Take
The CDC and FDA both suggested steps that clinical laboratories and other providers can take to conserve their supplies of the bottles.
Laboratories should strive to prevent contamination of blood cultures, which “can negatively affect patient care and may require the collection of more blood cultures to help determine whether contamination has occurred,” the CDC advised.
In addition, providers should “ensure that the appropriate volume is collected when collecting blood for culture,” the advisory states. “Underfilling bottles decreases the sensitivity to detect bacteremia/fungemia and may require additional blood cultures to be drawn to diagnose an infection.”
Laboratories should also explore alternative options, such as “sending samples out to a laboratory not affected by the shortage.”
The FDA advised providers to collect blood cultures “when medically necessary” in compliance with clinical guidelines, giving priority to patients exhibiting signs of a bloodstream infection.
In an email to STAT, Andrew T. Pavia, MD, Professor of Internal Medicine and Pediatrics at the University of Utah, offered examples of situations where blood culture tests are unnecessary according to clinical guidelines.
“There are conditions like uncomplicated community acquired pneumonia or skin infections where blood cultures are often obtained but add very little,” he told STAT. “It will be critical though that blood cultures are obtained from patients with sepsis, those likely to have bloodstream infections, and very vulnerable patients.”
Hospitals Already Addressing Shortage
STAT reported that some hospitals have already taken measures to reduce the number of tests they run. And some are looking into whether they can safely use bottles past their expiration dates.
Sarah Turbett, MD, Associate Director of Clinical Microbiology Laboratories at Massachusetts General Hospital in Boston, told STAT that her team tested bottles “that were about 100 days past their expiration date to see if they were still able to detect pathogens with the same efficacy as bottles that had not yet expired. They saw no difference in the time to bacterial growth—needed to detect the cause of an infection—in the expired bottles when compared to bottles that had not expired.”
Turbett pointed to a letter in the Journal of Clinical Microbiology and Infection in which European researchers found that bottles from a different brand “were stable for between four and seven months after their expiration dates,” STAT reported.
During a Zoom call hosted by the CDC and the IDSA, hospital representatives asked if the FDA would permit use of expired bottles. However, “a representative of the agency was not able to provide an immediate answer,” STAT reported.
With sepsis being the leading cause of death in hospitals, these specimen bottles for blood culture testing are essential in diagnosing patients with relevant symptoms. This is a new example of how the supply chain for clinical laboratory instruments, tests, and consumables—which was a problem during the SARS-CoV-2 pandemic—continues to be problematic in unexpected ways.
Taking a wider view of supply chain issues that can be disruptive to normal operations of clinical laboratories and anatomic pathology groups, the market concentration of in vitro diagnostics (IVD) manufacturers means fewer vendors offering the same types of products. Consequently, if a lab’s prime vendor has a supply chain issue, there are few options available to swiftly purchase comparable products.
A separate but related issue in the supply chain involves “just in time” (JIT) inventory management—made famous by Taiichi Ohno of Toyota back in the 1980s. This management approach was designed to deliver components and products to the user hourly, daily, and weekly, as appropriate. The goal was to eliminate the cost of carrying large amounts of inventory. This concept evolved into what today is called the “Lean Manufacturing” method.
However, as was demonstrated during the SARS-CoV-2 pandemic, manufacturers and medical laboratories that had adopted JIT found themselves with inadequate numbers of components and finished products.
In the case of the current shortage of BD blood culture media bottles, this is a real-world example of how market concentration limited the number of vendors offering comparable products. At the same time, if this particular manufacturer was operating with the JIT inventory management approach, it found itself with minimal inventories of these media bottles to ship to lab clients while it addressed the manufacturing problems that caused this shortage.
Patients concerns about the quality of care provided since Amazon acquired One Medical in 2022 can affect clinical laboratory testing for those providers
Recently, The Washington Post reported on leaked documents that appear to indicate Amazon’s One Medical primary care call center was not using trained, certified medical professionals to field patient phone calls and provide telehealth guidance. Instead, The Post reported, “[One Medical’s] call center is staffed by contractors who receive about two weeks of medical training before responding to patient concerns,” and that, “They have missed urgent issues like blood pressure spikes and sudden stomach pain with blood in one patient’s stool,” MSN’s Business Insider reported.
The Washington Post, which is owned by Amazon founder Jeff Bezos, went on to report, “Amazon’s primary care clinic One Medical circulated talking points telling workers to claim that in cases when its call center failed to escalate potentially urgent calls to medical staff, patients ‘received the care they needed,’ according to screenshots of internal messages seen by The Washington Post.”
The Post’s report highlights the challenges some telemedicine providers using “non-physician” personnel are having in delivering quality primary care.
During the COVID-19 pandemic, social distancing and hospital lockdowns kept many people indoors and unable to access their doctors and clinical laboratories when they needed. As the pandemic progressed, enterprising mega corporations like Amazon saw an opportunity and invested heavily in bringing healthcare to patients where they live and shop.
Amazon, for example, announced in 2022 that it would be purchasing One Medical and all of its primary care clinics nationwide for $3.9 Billion.
“There is an immense opportunity to make the healthcare experience more accessible, affordable, and even enjoyable for patients, providers, and payers,” said Amir Dan Rubin, One Medical’s CEO, in an Amazon press release announcing the acquisition at that time. “We look forward to innovating and expanding access to quality healthcare services, together,” he added.
But it turns out, developing alternative pathways to primary care is not such an easy thing. According to Business Insider, some patients with One Medical are struggling to get adequate care, major patient concerns have been missed, and there are concerns over the efficacy of the services.
“The opportunity to transform healthcare and improve outcomes by combining One Medical’s human-centered and technology-powered model and exceptional team with Amazon’s customer obsession, history of invention, and willingness to invest in the long-term is so exciting,” said Amir Dan Rubin (above), One Medical’s CEO, in an Amazon press release. Clinical laboratories that service One Medical’s providers may want to follow this developing story. (Photo copyright: LinkedIn.)
Call Center Contractors Spark Concerns
One Medical was started by Harvard-trained internist Thomas Lee, MD, in an effort to streamline medical services to the benefit of stakeholders and patients, according to Forbes. This subscription based service offered patients 24/7 virtual care with access to in-person appointments.
“One Medical was founded in 2007 as a concierge medical network before going public in 2020 and purchasing Iora Health, a value-based provider for seniors, in 2021. By the end of 2022, a majority of One Medical’s revenue came from capitated contracts. The company currently operates more than 200 clinics and a telehealth service in a membership model,” Healthcare Dive reported.
But according to reports reviewed by journalists at The Washington Post, on more than one occasion elderly patients have been failed by the One Medical call center in Tempe, Arizona. Patients began to be rerouted to this call center about a year after the Amazon acquisition.
The Post reported that several patients reported symptoms such as pain and swelling, blood in stool, a spike in blood pressure and sudden rib pain, and that the call center failed to escalate these calls to clinical staff—instead simply scheduling an appointment sometimes for days later.
The workers at the Tempe call center included newly hired contractors with what The Post described as “limited training and little to no medical experience.” Internal sources at One Medical are raising the alarm bell about the dangers of Amazon’s frugal approach. “There were a lot of things slipping through the cracks,” one anonymous source told The Post.
Quantity over Quality
In an interview with PBS, Caroline O’Donovan, the reporter at The Washington Post who broke this story said, “In the documents that were leaked to us, there’s a doctor who wrote a note saying, ‘I don’t think these call center people even realize that they’re triaging patients, which is not something that they’re qualified to do.’”
Amazon contends that no one was harmed in the cases where protocol was not followed.
In an email statement concerning the Washington Post report, Amazon spokesperson Dawn Brun wrote, “While the patients ended up receiving the care they needed (during in-person visits with their providers), the initial call could have been managed more effectively,” The Post reported.
“We take patients’ feedback seriously and the [Washington Post] story mischaracterizes the dedication we have to our patients and care teams,” she added.
However, O’Donovan says that the patients—and some employees—she spoke with challenged that idea. “The patients I spoke to again and again—and some of the One Medical employees I spoke to—said there’s a difference between getting your phone call answered faster, literally someone picking up the phone, and actually getting your problem solved,” she told PBS.
When data-driven companies like Amazon get involved in healthcare certain care standards may be sacrificed in the name of optimization.
This story shows that there is not an easy solution/answer to developing alternative primary care pathways. Clinical laboratories have a stake in the evolution and developments in the field of primary care and telemedicine because often these patients need lab tests.
Researchers used CRISPR-based assays to develop new clinical laboratory point-of-care blood test which boasts accuracy, affordability, and accessibility
According to UPI, the test can “distinguish between influenza A and influenza B—the two main types of seasonal flu—as well as identifying more virulent strains like H1N1 and H3N2.”
Many research teams are working to develop paper-based diagnostic screening tests because of their lower cost to produce and usefulness in remote locations. Should this near-patient point-of-care test become clinically viable, it could mean shorter times to answer, enabling speedier diagnoses and earlier start of treatment.
It also means patient specimens do not have to be transported to a clinical laboratory for testing. And reduced cost per test makes it possible to test more people. This serves the public health aspect of monitoring outbreaks of influenza and other diseases and gives hope for improved treatment outcomes.
“Being able to tease apart what strain or subtype of influenza is infecting a patient has repercussions both for treating them and public health interventions, said Jon Arizti Sanz, PhD, co-lead study author and postdoctoral researcher at the Broad Institute of Harvard and MIT, in a Broad Institute news release.
“Ultimately, we hope these tests will be as simple as rapid antigen tests, and they’ll still have the specificity and performance of a nucleic acid test that would normally be done in a laboratory setting,” Cameron A. Myhrvold, PhD (above), Assistant Professor of Molecular Biology at Princeton University in New Jersey, told CIDRAP. Influenza tests that can be performed at the point of care and in remote locations may reduce the number of screening tests performed by clinical laboratories. (Photo copyright: Michael James Butts/Hertz Foundation.)
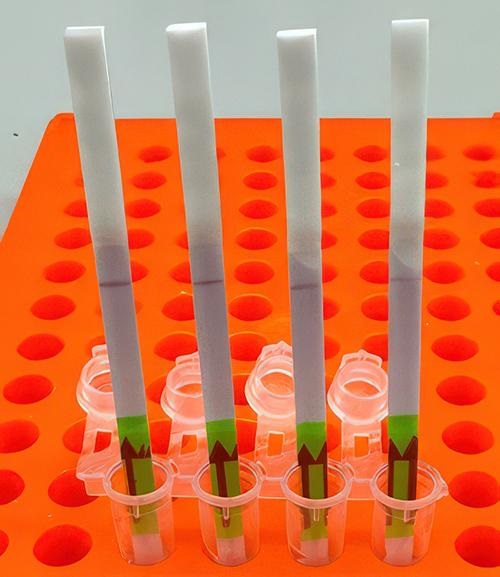
Her team developed their tests using Streamlined Highlighting of Infections to Navigate Epidemics (SHINE), “a clustered regularly interspaced short palindromic repeats (CRISPR)-based RNA detection platform,” the researchers wrote in their Journal of Molecular Diagnostics paper.
“SHINE has a runtime of 90 minutes, can be used at room temperature and only requires an inexpensive heat block to heat the reaction. The SHINE technology has previously been used to identify SARS-CoV-2 and later to distinguish between the Delta and Omicron variants,” Bioanalysis Zone reported.
“The test uses genetically engineered enzymes to identify specific sequences of viral RNA in samples,” the researchers told UPI. Originally designed to detect COVID-19, the team adapted the technology to detect influenza in 2022 “with the aim of creating a screening tool that could be used in the field or in clinics rather than hospitals or high-tech diagnostic labs,” they said.
Influenza A and B as well as H1N1 and H3N2 subtypes were the targets of the four SHINE assays. “When tested on clinical samples, these optimized assays achieved 100% concordance with quantitative RT-PCR. Duplex Cas12a/Cas13a SHINE assays were also developed to detect two targets simultaneously,” the researchers wrote in their paper.
The team used “20 nasal swabs from people with flu-like symptoms during the 2020-2021 flu season, nasal fluid from healthy people as the control, and 2016-2021 influenza sequences downloaded from the National Center for Biotechnology Information Influenza (NICB) database. They compared the results with those from quantitative reverse transcription-polymerase chain reaction (RT-PCR) tests,” CIDRAP reported.
The original 2020 test (shown above) takes 90 minutes to develop at room temperature. The test developers aim to drop this down to 15 minutes. In comparison, typical polymerase chain reaction (PCR) testing requires medical laboratories to have specialized equipment, trained staff, and prolonged processing times, the Broad Institute news release notes. (Photo copyright: Broad Institute.)
Implications of the New Tests
The ease of the new tests is an important development since approximately only 1% of individuals who come down with the flu see doctors for testing, according to the news release. And researchers had this in mind, looking at speed, accuracy, and affordability as a means to “improve outbreak response and infection care around the world,” UPI reported.
There are great benefits to strain differentiation that be achieved with the new test. Doctors are hopeful the test will help dial in the best treatment plans for patients since some strains are resistant to the antiviral medication oseltamivir (Tamiflu), UPI noted. This is significant since Tamiflu “is a common antiviral,” said Sanz in the Broad Institute news release.
“These assays have the potential to expand influenza detection outside of clinical laboratories for enhanced influenza diagnosis and surveillance,” the Journal of Molecular Diagnostics paper noted. This allows for more strategic treatment planning.
“Using a paper strip readout instead of expensive fluorescence machinery is a big advancement, not only in terms of clinical care but also for epidemiological surveillance purposes,” said Ben Zhang, an MD candidate in the Health Sciences and Technology at Harvard and co-first author of the study, in the Broad Institute news release.
Future Plans for Tests
“With further development, the test strip could be reprogrammed to distinguish between SARS-CoV-2 and flu and recognize swine flu and avian flu, including the H5N1 subtype currently causing an outbreak in US dairy cattle,” the study authors told CIDRAP.
The team is also looking at ways to help prevent H5N1 from crossing into human contamination, Sanz told UPI.
The new Princeton/MIT/Harvard tests echo the trend to bring in affordability and ease-of-use with accurate results as an end goal. Faster results mean the best treatments for each person can start sooner and may render the transport of specimens to a clinical laboratory as a second step unnecessary.
As research teams work to develop paper-based viral tests for their plethora of benefits, clinical laboratories will want to pay close attention to this development as it can have a big implication on assisting with future outbreaks.
Additional research is needed before these tests are going to be commonplace in homes worldwide, but this first step brings inspiration and hope of what’s to come.
Study of the 50 Omicron variants could lead to new approaches to clinical laboratory testing and medical treatments for long COVID
Patients infected with SARS-CoV-2 can usually expect the COVID-19 illness to subside within a couple of weeks. However, one Dutch patient remained infected with the coronavirus for 612 days and fought more than 50 mutations (aka, variants) before dying late last year of complications due to pre-existing conditions. This extreme case has given doctors, virologists, microbiologists, and clinical laboratories new insights into how the SARS-CoV-2 virus mutates and may lead to new treatments for long COVID.
The medication the patient was taking for his pre-existing conditions may have contributed to his body being unable to produce antibodies in response to three shots of the Moderna mRNA COVID vaccine he received.
Magda Vergouwe, MD, PhD candidate at the Center for Experimental and Molecular Medicine (CEMM), Amsterdam UMC, who lead a study into the patient, theorized that some of the medications the patient was on for his pre-existing conditions could have destroyed healthy cells alongside the abnormal cancer-causing B cells the drugs were meant to target.
“This case underscores the risk of persistent SARS-CoV-2 infections in immunocompromised individuals,” the researchers said prior to presenting their report about the case at a meeting of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in Barcelona, Spain, Time reported. “We emphasize the importance of continuing genomic surveillance of SARS-CoV-2 evolution in immunocompromised individuals with persistent infections.”
“Chronic infections and viral evolution [are] commonly described in [the] literature, and there are other cases of immunocompromised patients who have had [COVID] infections for hundreds of days,” Magda Vergouwe, MD, PhD candidate (above), Center for Experimental and Molecular Medicine at Amsterdam UMC, told Scientific American. “But this is unique due to the extreme length of the infection … and with the virus staying in his body for so long, it was possible for mutations to just develop and develop and develop.” Microbiologists, virologists, and clinical laboratories involved in testing patients with long COVID may want to follow this story. (Photo copyright: LinkedIn.)
Risks to Immunocompromised Patients
Pre-existing conditions increase the risk factor for COVID-19 infections. A 2021 study published in the Journal of the American Board of Family Medicine (JABFM) titled, “Prevalence of Pre-existing Conditions among Community Health Center Patients with COVID-19,” found that about 61% of that study’s test group had a pre-existing condition prior to the outbreak of the COVID-19 pandemic.
When the Dutch man was admitted to Amsterdam UMC with common and serious COVID-19 symptoms, such as shortness of breath, a cough, and low blood oxygen levels, he was prescribed sotrovimab (a monoclonal antibody) along with other COVID treatments.
About a month after being admitted his COVID-19 symptoms decreased, so he was first discharged to a rehab facility and then finally to his home. However, he continued to test positive for the coronavirus and developed other infections that may have been complicated by the persistent case of COVID-19.
The Amsterdam UMC doctors emphasized that the man ultimately succumbed to his pre-existing conditions and not necessarily COVID-19.
“It’s important to note that in the end he did not die from his COVID-19,” Vergouwe told Scientific American. “But he did keep it with him for a very long period of time until then, and this is why we made sure to sample [the virus in his body] as much as we could.”
One in Five Adults Develop Long COVID
Long COVID does not necessarily indicate an active infection. However, in as many as one in five US adults COVID symptoms persist after the acute phase of the infection is over, according to a study published recently in JAMA Network Open titled, “Epidemiologic Features of Recovery from SARS-CoV-2 Infection.”
“In this cohort study, more than one in five adults did not recover within three months of SARS-CoV-2 infection. Recovery within three months was less likely in women and those with pre-existing cardiovascular disease and more likely in those with COVID-19 vaccination or infection during the Omicron variant wave,” the JAMA authors wrote.
The origins of long COVID are not entirely clear, but according to the National Institutes of Health (NIH) it can develop when a patient is unable to sufficiently rest while battling off the initial virus. According to Vergouwe, the SARS-CoV-2 genome will always grow quicker when found in a patient with a compromised immune system.
Unique COVID-19 Mutations
More than 50 new mutations of the original Omicron variant were identified in the Dutch patient. According to Vergouwe, “while that number can sound shocking, mutations to the SARS-CoV-2 genome are expected to evolve more quickly in those who are immunocompromised (the average mutation rate of the virus is estimated to be two mutations per person per month),” Scientific American reported. “What does make these mutations unusual, she noted, is how their features differed vastly from mutations observed in other people with COVID. [Vergouwe] hypothesizes that the exceptional length of the individual’s infection, and his pre-existing conditions, allowed the virus to evolve extensively and uniquely.”
COVID-19 appears to be here to stay, and most clinical laboratory managers and pathologists understand why. As physicians continue to learn about the SARS-CoV-2 coronavirus, this is another example of how the knowledge about SARS-CoV-2 is growing as different individuals are infected with different variants of the virus.