Settlement is a reminder to all clinical laboratories that state and federal DOJs and AGs are willing to file actions against genetic testing companies that intentionally mislead the public
California’s Attorney General, in cooperation with the Federal Trade Commission (FTC), announced a recent settlement with CRI Genetics regarding deceptive trade practices. The at-home genetics testing company will have to pay $700,000 in civil penalties and according to the Santa Monica Daily Press, “will be barred from a wide range of deceptive practices to settle charges from the Federal Trade Commission and the California Attorney General that the company deceived users about the accuracy of its DNA reports.”
Santa Monica, Calif.-based CRI Genetics (CRI), which also does business as OmniPGx, offers DNA saliva-swab test kits that are analyzed by a third party laboratory to return customers ancestry data, health information, optimal nutritional guidelines, and potential allergies. The company’s website states a guaranteed 8-week turn around for the kits.
The original complaint against CRI alleged the company used misleading marketing practices by claiming its DNA tests are more accurate and detailed than their competitors, such as Ancestry DNA and 23andMe. CRI also claimed their ancestry data was more than 90% accurate and could determine ancestry dating back 50 generations.
In addition, the company stated its algorithm for matching DNA was patented, which it was not, according to the complaint.
The complaint also alleged the CRI website contained deceitful information and was formatted to appear independent but included inflated reviews and false testimonials.
“CRI Genetics could have found legitimatewaysto market its services. Unfortunately, in its pursuit of growth and profits, the company repeatedly misled consumers. The FTC and my office took notice, we investigated, and we are delivering results today,” said California Attorney General Rob Bonta (above) in a press release. (Photo copyright: State of California Department of Justice.)
Alleged Deceptive Business Practices
According to court documents, CRI manipulated customers into purchasing add-on services and forced consumers to click through a myriad of pop-up pages to lure them into purchasing more products. Customers were informed they would have a chance to review their orders before being charged but were immediately billed. Consumers then had to go through a lengthy and often confusing process to obtain refunds for returned items.
“Based on the facts and violations of law alleged in this Complaint, the FTC has reason to believe that Defendant has violated or is about to violate laws enforced by the Commission because, among other things, Defendant engaged in the unlawful conduct over a period of four years, willfully and knowingly, despite having knowledge of hundreds of consumer complaints and refund requests, as well as inquiries by the Better Business Bureau regarding their deceptive practices and only ceased its unlawful activities after the FTC notified Defendant of its pending investigation,” the court filings state.
“Our settlement not only holds CRI Genetics accountable for its past misconduct, it also aims to ensure that CRI Genetics doesn’t engage in similar misconduct going forward,” said California Attorney General Rob Bonta in the press release. “I want to thank our federal counterparts at the FTC for their continued partnership and commitment to ensuring that all businesses play by the same rules.”
In addition to the $700,000 fine, CRI is obligated to change its practices by:
Ceasing to make misrepresentations about its testing and analysis services.
Not using deceptive tactics to sell its products, represent endorsements, or in billing practices.
Accurately disclosing its website billing practices.
Disclosing any sharing or usage of genetic data for purposes besides the services the consumer purchases.
Refraining from offering the sale of any DNA information testing product or service.
“Today’s action continues the FTC’s crackdown on deceptive reviews, dark patterns, and baseless claims around algorithmic solutions,” said Samuel Levine, Director, Bureau of Consumer Protection at the FTC, in the press release. “We are proud to partner with California on this important matter and will continue to carefully scrutinize claims around biometric information technologies.”
This settlement serves as a reminder to all genetic testing firms and clinical laboratories that state and federal Departments of Justice and state Attorney Generals are willing to file actions against genetic testing organizations that intentionally mislead the public. It is also useful for lab managers to stay aware of the lengths some genetic testing companies will go to deceive consumers and that regulatory agencies are noticing egregious practices.
Patients concerns about the quality of care provided since Amazon acquired One Medical in 2022 can affect clinical laboratory testing for those providers
Recently, The Washington Post reported on leaked documents that appear to indicate Amazon’s One Medical primary care call center was not using trained, certified medical professionals to field patient phone calls and provide telehealth guidance. Instead, The Post reported, “[One Medical’s] call center is staffed by contractors who receive about two weeks of medical training before responding to patient concerns,” and that, “They have missed urgent issues like blood pressure spikes and sudden stomach pain with blood in one patient’s stool,” MSN’s Business Insider reported.
The Washington Post, which is owned by Amazon founder Jeff Bezos, went on to report, “Amazon’s primary care clinic One Medical circulated talking points telling workers to claim that in cases when its call center failed to escalate potentially urgent calls to medical staff, patients ‘received the care they needed,’ according to screenshots of internal messages seen by The Washington Post.”
The Post’s report highlights the challenges some telemedicine providers using “non-physician” personnel are having in delivering quality primary care.
During the COVID-19 pandemic, social distancing and hospital lockdowns kept many people indoors and unable to access their doctors and clinical laboratories when they needed. As the pandemic progressed, enterprising mega corporations like Amazon saw an opportunity and invested heavily in bringing healthcare to patients where they live and shop.
Amazon, for example, announced in 2022 that it would be purchasing One Medical and all of its primary care clinics nationwide for $3.9 Billion.
“There is an immense opportunity to make the healthcare experience more accessible, affordable, and even enjoyable for patients, providers, and payers,” said Amir Dan Rubin, One Medical’s CEO, in an Amazon press release announcing the acquisition at that time. “We look forward to innovating and expanding access to quality healthcare services, together,” he added.
But it turns out, developing alternative pathways to primary care is not such an easy thing. According to Business Insider, some patients with One Medical are struggling to get adequate care, major patient concerns have been missed, and there are concerns over the efficacy of the services.
“The opportunity to transform healthcare and improve outcomes by combining One Medical’s human-centered and technology-powered model and exceptional team with Amazon’s customer obsession, history of invention, and willingness to invest in the long-term is so exciting,” said Amir Dan Rubin (above), One Medical’s CEO, in an Amazon press release. Clinical laboratories that service One Medical’s providers may want to follow this developing story. (Photo copyright: LinkedIn.)
Call Center Contractors Spark Concerns
One Medical was started by Harvard-trained internist Thomas Lee, MD, in an effort to streamline medical services to the benefit of stakeholders and patients, according to Forbes. This subscription based service offered patients 24/7 virtual care with access to in-person appointments.
“One Medical was founded in 2007 as a concierge medical network before going public in 2020 and purchasing Iora Health, a value-based provider for seniors, in 2021. By the end of 2022, a majority of One Medical’s revenue came from capitated contracts. The company currently operates more than 200 clinics and a telehealth service in a membership model,” Healthcare Dive reported.
But according to reports reviewed by journalists at The Washington Post, on more than one occasion elderly patients have been failed by the One Medical call center in Tempe, Arizona. Patients began to be rerouted to this call center about a year after the Amazon acquisition.
The Post reported that several patients reported symptoms such as pain and swelling, blood in stool, a spike in blood pressure and sudden rib pain, and that the call center failed to escalate these calls to clinical staff—instead simply scheduling an appointment sometimes for days later.
The workers at the Tempe call center included newly hired contractors with what The Post described as “limited training and little to no medical experience.” Internal sources at One Medical are raising the alarm bell about the dangers of Amazon’s frugal approach. “There were a lot of things slipping through the cracks,” one anonymous source told The Post.
Quantity over Quality
In an interview with PBS, Caroline O’Donovan, the reporter at The Washington Post who broke this story said, “In the documents that were leaked to us, there’s a doctor who wrote a note saying, ‘I don’t think these call center people even realize that they’re triaging patients, which is not something that they’re qualified to do.’”
Amazon contends that no one was harmed in the cases where protocol was not followed.
In an email statement concerning the Washington Post report, Amazon spokesperson Dawn Brun wrote, “While the patients ended up receiving the care they needed (during in-person visits with their providers), the initial call could have been managed more effectively,” The Post reported.
“We take patients’ feedback seriously and the [Washington Post] story mischaracterizes the dedication we have to our patients and care teams,” she added.
However, O’Donovan says that the patients—and some employees—she spoke with challenged that idea. “The patients I spoke to again and again—and some of the One Medical employees I spoke to—said there’s a difference between getting your phone call answered faster, literally someone picking up the phone, and actually getting your problem solved,” she told PBS.
When data-driven companies like Amazon get involved in healthcare certain care standards may be sacrificed in the name of optimization.
This story shows that there is not an easy solution/answer to developing alternative primary care pathways. Clinical laboratories have a stake in the evolution and developments in the field of primary care and telemedicine because often these patients need lab tests.
Researchers used CRISPR-based assays to develop new clinical laboratory point-of-care blood test which boasts accuracy, affordability, and accessibility
According to UPI, the test can “distinguish between influenza A and influenza B—the two main types of seasonal flu—as well as identifying more virulent strains like H1N1 and H3N2.”
Many research teams are working to develop paper-based diagnostic screening tests because of their lower cost to produce and usefulness in remote locations. Should this near-patient point-of-care test become clinically viable, it could mean shorter times to answer, enabling speedier diagnoses and earlier start of treatment.
It also means patient specimens do not have to be transported to a clinical laboratory for testing. And reduced cost per test makes it possible to test more people. This serves the public health aspect of monitoring outbreaks of influenza and other diseases and gives hope for improved treatment outcomes.
“Being able to tease apart what strain or subtype of influenza is infecting a patient has repercussions both for treating them and public health interventions, said Jon Arizti Sanz, PhD, co-lead study author and postdoctoral researcher at the Broad Institute of Harvard and MIT, in a Broad Institute news release.
“Ultimately, we hope these tests will be as simple as rapid antigen tests, and they’ll still have the specificity and performance of a nucleic acid test that would normally be done in a laboratory setting,” Cameron A. Myhrvold, PhD (above), Assistant Professor of Molecular Biology at Princeton University in New Jersey, told CIDRAP. Influenza tests that can be performed at the point of care and in remote locations may reduce the number of screening tests performed by clinical laboratories. (Photo copyright: Michael James Butts/Hertz Foundation.)
Her team developed their tests using Streamlined Highlighting of Infections to Navigate Epidemics (SHINE), “a clustered regularly interspaced short palindromic repeats (CRISPR)-based RNA detection platform,” the researchers wrote in their Journal of Molecular Diagnostics paper.
“SHINE has a runtime of 90 minutes, can be used at room temperature and only requires an inexpensive heat block to heat the reaction. The SHINE technology has previously been used to identify SARS-CoV-2 and later to distinguish between the Delta and Omicron variants,” Bioanalysis Zone reported.
“The test uses genetically engineered enzymes to identify specific sequences of viral RNA in samples,” the researchers told UPI. Originally designed to detect COVID-19, the team adapted the technology to detect influenza in 2022 “with the aim of creating a screening tool that could be used in the field or in clinics rather than hospitals or high-tech diagnostic labs,” they said.
Influenza A and B as well as H1N1 and H3N2 subtypes were the targets of the four SHINE assays. “When tested on clinical samples, these optimized assays achieved 100% concordance with quantitative RT-PCR. Duplex Cas12a/Cas13a SHINE assays were also developed to detect two targets simultaneously,” the researchers wrote in their paper.
The team used “20 nasal swabs from people with flu-like symptoms during the 2020-2021 flu season, nasal fluid from healthy people as the control, and 2016-2021 influenza sequences downloaded from the National Center for Biotechnology Information Influenza (NICB) database. They compared the results with those from quantitative reverse transcription-polymerase chain reaction (RT-PCR) tests,” CIDRAP reported.
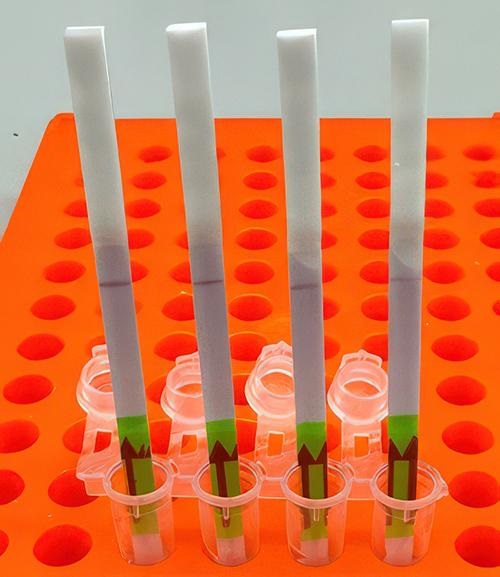
The original 2020 test (shown above) takes 90 minutes to develop at room temperature. The test developers aim to drop this down to 15 minutes. In comparison, typical polymerase chain reaction (PCR) testing requires medical laboratories to have specialized equipment, trained staff, and prolonged processing times, the Broad Institute news release notes. (Photo copyright: Broad Institute.)
Implications of the New Tests
The ease of the new tests is an important development since approximately only 1% of individuals who come down with the flu see doctors for testing, according to the news release. And researchers had this in mind, looking at speed, accuracy, and affordability as a means to “improve outbreak response and infection care around the world,” UPI reported.
There are great benefits to strain differentiation that be achieved with the new test. Doctors are hopeful the test will help dial in the best treatment plans for patients since some strains are resistant to the antiviral medication oseltamivir (Tamiflu), UPI noted. This is significant since Tamiflu “is a common antiviral,” said Sanz in the Broad Institute news release.
“These assays have the potential to expand influenza detection outside of clinical laboratories for enhanced influenza diagnosis and surveillance,” the Journal of Molecular Diagnostics paper noted. This allows for more strategic treatment planning.
“Using a paper strip readout instead of expensive fluorescence machinery is a big advancement, not only in terms of clinical care but also for epidemiological surveillance purposes,” said Ben Zhang, an MD candidate in the Health Sciences and Technology at Harvard and co-first author of the study, in the Broad Institute news release.
Future Plans for Tests
“With further development, the test strip could be reprogrammed to distinguish between SARS-CoV-2 and flu and recognize swine flu and avian flu, including the H5N1 subtype currently causing an outbreak in US dairy cattle,” the study authors told CIDRAP.
The team is also looking at ways to help prevent H5N1 from crossing into human contamination, Sanz told UPI.
The new Princeton/MIT/Harvard tests echo the trend to bring in affordability and ease-of-use with accurate results as an end goal. Faster results mean the best treatments for each person can start sooner and may render the transport of specimens to a clinical laboratory as a second step unnecessary.
As research teams work to develop paper-based viral tests for their plethora of benefits, clinical laboratories will want to pay close attention to this development as it can have a big implication on assisting with future outbreaks.
Additional research is needed before these tests are going to be commonplace in homes worldwide, but this first step brings inspiration and hope of what’s to come.
Use of artificial intelligence in clinical laboratory testing could improve the diagnosis of cancer worldwide
In a proof of concept study, scientists at Shanghai Jiao Tong University in China have developed a clinical laboratory test that utilizes artificial intelligence (AI) to diagnose three types of cancer from a single drop of dried blood. The paper-based test was able to identify patients with colorectal, gastric, and pancreatic cancers and distinguish between patients with and without cancer.
The team’s goal was to develop a way to diagnose cancer while the disease is still in the earlier stages, especially in rural areas.
“Over a billion people across the world experience a high rate of missed disease diagnosis, an issue that highlights the need for diagnostic tools showing increased accuracy and affordability. In addition, such tools could be used in ecologically fragile and energy-limited regions, pointing to the need for developing solutions that can maximize health gains under limited resources for enhanced sustainability,” the researchers wrote in an article published in the journal Nature Sustainability titled, “A Sustainable Approach to Universal Metabolic Cancer Diagnosis.”
The researchers determined that by using less than 0.05 millimeters of dried blood, their test could accurately and quickly identify if a patient had cancer between 82% to 100% of the time.
According to Chaoyuan Kuang, MD, PhD (above), an oncologist at Montefiore Health System and assistant professor at the Albert Einstein College of Medicine, unlike liquid blood, dried serum can be “collected, stored, and transported at much lower cost and with much simpler equipment,” Live Science reported. “This could help democratize the availability of cancer early detection testing across the world,” he added. A paper-based clinical laboratory test that can detect and distinguish one cancer type from another would be a boon to cancer diagnosis worldwide. (Photo copyright: Albert Einstein College of Medicine.)
Improving Cancer Screening in Rural Areas
An earlier study conducted in China in 2022 examined results from 1,570 cancer survivors from both urban and rural areas of China. That study showed that 84.1% of the patients were diagnosed with cancer only after developing symptoms and that urban patients were more likely to be diagnosed in the early stages of cancer. In addition, rural patients also had less screening and treatment options available to them.
The researchers in this latest Chinese study tested their AI model on blood donors with and without cancer and compared the results to traditional liquid-blood biopsy tests.
“Based on modeling they performed, they reported the new tool could reduce the estimated proportion of undiagnosed cases of pancreatic, gastric, and colorectal cancers by about 20% to 50% if it was used for population-level cancer screening in rural China,” Live Science reported.
The scientists used dried serum spots (DSS) and machine learning to perform the research. According to their Nature Sustainability paper, DSS can be challenging in cancer research because sensitive biomarkers in the samples are often degraded or have inadequate amount of blood for proper analysis. To circumvent these issues, the researchers used nanoparticle-enhanced laser desorption/ionization mass spectrometry (NPELDI MS) to increase reliability and sensitivity. Inorganic nanoparticles were applied to the samples to strengthen selectivity and refine metabolic compounds from the samples.
However, the study authors noted that “the adaptation of NPELDI MS to dried spot analysis has not been validated,” Interesting Engineering reported.
A ‘Great Start’
The machine learning algorithm the Chinese scientists created demonstrates that DSS samples can be used to preserve important biological markers and could be beneficial in the diagnosis of cancer.
Their research indicated an overall reduction rate of undiagnosed cancers in the range of 20.35% to 55.10%. The researchers estimated the implementation of their AI tool could reduce the proportion of specific undiagnosed cancer cases in rural China by:
84.30% to 29.20% for colorectal cancer,
77.57% to 57.22% for gastric cancer, and
34.56% to 9.30% for pancreatic cancer.
It’s a “great start,” Chaoyuan Kuang, MD, PhD, an oncologist at Montefiore Health System and assistant professor at the Albert Einstein College of Medicine told Live Science. “This cancer test won’t enter use for a long time,” he said. Nevertheless, the potential of the tool is “immense,” he added, but that “we are still years away from being able to offer this test to patients.
“With further development, it could theoretically be used for the early detection of other types of cancer or for other diseases, or to monitor the progression of disease in patients who have already been diagnosed,” he noted.
Further research and clinical trials are needed before this AI tool can be used in a clinical diagnostic setting. This study is another example of researchers looking for cancer biomarkers in specimen types that are not tissue and further supports the hope that machine learning may one day detect cancer in earlier stages, increase survival rates, and save healthcare costs.
One factor motivating this type of research in China is the fact that the nation has more than 36,000 hospitals and approximately 20,000 anatomic pathologists. Of this total, only a minority of these pathologists have been trained to the standards of North America and Northern Europe.
Like other nations, China’s demand for subspecialist pathology services outstrips its supply of such pathologists. This is the reason why researchers in that country want to develop diagnostic assays for cancer and other diseases that are faster, cheaper, and comparable to a human pathologist in accuracy.
Results of an earlier study in which locks of Beethoven’s hair underwent genetic analysis showed the composer ‘had a predisposition for liver disease and became infected with hepatitis B’
Here is an example of modern technologies being used with “historical biospecimens” to solve long-standing mysteries or questions about the illnesses of famous historical figures. Clinical laboratory scientists at the Mayo Clinic have used modern-day chemical analysis techniques to answer a 200-year-old question: What caused Ludwig van Beethoven’s deafness and other health problems?
“Such lead levels are commonly associated with gastrointestinal and renal ailments and decreased hearing but are not considered high enough to be the sole cause of death,” the authors wrote.
Beethoven’s death at age 56 has been attributed to kidney and liver disease, CNN reported. Even if the lead concentrations were not the sole cause, they would nevertheless be regarded as lead poisoning, lead study author Nader Rifai, PhD, told CNN.
“If you walk into any emergency room in the United States with these levels, you will be admitted immediately and you will undergo chelation therapy,” he said.
“It is believed that Beethoven died from liver and kidney disease at age 56. But the process of understanding what caused his many health problems has been a much more complicated puzzle, one that even Beethoven himself hoped doctors could eventually solve,” CNN reported, adding, “The composer expressed his wish that his ailments be studied and shared so ‘as far as possible at least the world will be reconciled to me after my death.’” Mayo clinical laboratory scientists are using chemical analysis on authenticated locks of Beethoven’s hair to do just that. (Photo copyright: Joseph Karl Stieler/Public Domain.)
Mass Spectrometry Analysis
Mayo Clinic’s metals laboratory, led by chemist Paul Jannetto, PhD, an associate professor in the Department of Laboratory Medicine and Pathology and Laboratory Director at the Mayo Clinic, performed the analysis on two authenticated locks of Beethoven’s hair, using inductively coupled plasma mass spectrometers.
The researchers found that one lock had 258 micrograms of lead/gram and the other had 380 micrograms. Normally they would expect to find less than four micrograms.
“These are the highest values in hair I’ve ever seen,” Jannetto told The New York Times. “We get samples from around the world and these values are an order of magnitude higher.”
The researchers also found that the composer’s hair had four times the normal level of mercury and 13 times the normal amount of arsenic.
Rifai and other researchers noted that Beethoven drank large amounts of plumbed wine, and at the time it was common to sweeten wine with lead acetate, CNN reported.
The composer also could have been exposed to lead in glassware. He likely absorbed high levels of arsenic and mercury by eating fish caught from the Danube River in Vienna.
David Eaton, PhD, a toxicologist, pharmacologist, and Professor Emeritus, Department of Environmental and Occupational Health Sciences at the University of Washington, told The New York Times that high levels of lead could have impaired Beethoven’s hearing through their effect on the nervous system. Additionally, he said the composer’s gastrointestinal ailments “are completely consistent with lead poisoning.”
Rifai told CNN that he’d like to study locks of hair from other 19th century Vienna residents to see how their lead levels compared with Beethoven’s.
Beethoven’s Genome and Genetic Predisposition for Liver Disease
Additional research published in May built on an earlier genomic analysis of Beethoven’s hair, which appeared in March 2023 in the journal Current Biology.
The international team included geneticists, archeologists, and immunologists who analyzed eight locks of hair attributed to the composer. They determined that five were authentic. One, known as the Stumpff Lock, appeared to be the best preserved. They used this lock to sequence Beethoven’s DNA.
“Although we could not identify a genetic explanation for Beethoven’s hearing disorder or gastrointestinal problems, we found that Beethoven had a genetic predisposition for liver disease,” the authors wrote. “Metagenomic analyses revealed furthermore that Beethoven had a hepatitis B infection during at least the months prior to his death. Together with the genetic predisposition and his broadly accepted alcohol consumption, these present plausible explanations for Beethoven’s severe liver disease, which culminated in his death.”
One surprising discovery was the likelihood of an extramarital affair on the composer’s father’s side, CNN reported. The researchers learned this in part by comparing his genetic profile with those of living relatives.
“Through the combination of DNA data and archival documents, we were able to observe a discrepancy between Ludwig van Beethoven’s legal and biological genealogy,” study coauthor Maarten Larmuseau, PhD, told CNN. Larmuseau is assistant professor, Faculty of Medicine, and head of the Laboratory of Human Genetic Genealogy at KU Leuven in Belgium.
The Mayo Clinic team used two locks authenticated in the 2023 study—the Bermann Lock and Halm-Thayer Lock—to perform their chemical analysis, CNN reported.
Beethoven’s Wishes
The earlier study noted that Beethoven wanted his health problems to be made public. In 1802, he wrote a document known as the Heiligenstadt Testament in which he asked that his physician, surgeon/ophthalmologist Johann Adam Schmidt, MD, discuss his disease after he died.
“For almost two years I have ceased to attend any social functions, just because I find it impossible to say to people: I am deaf,” Beethoven wrote at age 30, The New York Times reported. “If I had any other profession, I might be able to cope with my infirmity, but in my profession, it is a terrible handicap. And if my enemies, of whom I have a fair number, were to hear about it, what would they say?”
The authors of the Current Biology paper wrote, “Genomic sequence data from authenticated locks of Beethoven’s hair provide Beethoven studies with a novel primary source, already revealing several significant findings relating to Beethoven’s health and genealogy, including substantial heritable risk for liver disease, infection with HBV [Hepatitis B], and EPP [extra pair paternity]. This dataset additionally permits numerous future lines of scientific inquiry.
“The further development of bioinformatics methods for risk stratification and continued progress in medical genetic research will allow more precise assessments both for Beethoven’s disease risk and for the genetic inference of additional phenotypes of interest.
“This study illustrates the contribution and further potential of genomic data as a novel primary source in historical biography,” the scientists concluded.
The work of the clinical laboratory professionals at Mayo Clinic also demonstrates how advances in various diagnostic technologies can enable pathologists and lab scientists to participate in solving long-standing health questions about historical figures, especially if their hair or other types of specimens survived and can be used in the analysis.