Encouraging patients—even children—to be more directly involved in their own medical care may reduce the burden on healthcare workers and might even help those clinical laboratories struggling to hire enough phlebotomists to collect specimens
Researchers at Emory University School of Medicine have concluded a study which found that school-aged children can successfully use a nasal swab to obtain their own SARS-CoV-2 test specimens. This may come as a surprise to hospital and clinical laboratory personnel who have performed nasal swabbing for COVID-19 tests. Some people, adults included, find the procedure so uncomfortable it brings tears.
And yet, after being shown a 90-second how-to video and given a handout with written instructions and pictures, 197 Atlanta children who had COVID-19 symptoms between July and August of 2021 performed their own self-swabbing. A healthcare worker then collected a second swabbed sample. All samples were submitted to a clinical laboratory for PCR analysis.
The Emory study provides another example of how the healthcare system is engaging patients to be directly involved in their own medical care. Results of the study could positively impact clinical laboratories facing a shortage of personnel, as well as schools where children have to take repeated COVID-19 tests with the assistance of trained professionals.
In a study with 197 school-age children, researchers at Emory University School of Medicine found that children could self-swab themselves for COVID-19 testing after watching a 90-second instructional video. Clinical laboratory leaders who are short on personnel may find these results intriguing. (Photo copyright: Emory University.)
How Did the Children Do?
The self-collected swabs and those collected by a healthcare worker agreed 97.8% of the time for a positive result and 98.1% of the time for a negative result. The analysis showed that both collection methods identified the 44% of symptomatic kids who were positive for COVID-19.
“Seeing how closely the results line up between the children and trained healthcare workers is a strong indicator that these age groups are fully capable of swabbing themselves if given proper instruction,” said Jesse Waggoner, MD, an Assistant Professor of Infectious Diseases with the Emory University School of Medicine and one of the lead authors on the study, in an Emory University press release.
A higher percentage of children age eight and under needed assistance, such as more instruction before correctly completing self-collection—21.8% compared to 6.1% for children older—but SARS-CoV-2 detection among the two age groups did not differ.
Does FDA Approve of Self-Swabbing?
The US Food and Drug Administration (FDA) has not authorized COVID-19 tests that include self-swabbing by children under age 14. However, data from the Emory study, published in JAMA, is now available to test manufacturers seeking authorization for pediatric self-collection.
“Pediatric self-swabbing will support expanded testing access and should make it even easier to test school age populations with fewer resources,” said Tim Stenzel, MD, PhD, Director of the Office of In Vitro Diagnostics at the FDA, in the Emory statement. “This study furthers our knowledge of test accuracy with these types of samples and provides test manufacturers with data to support their EUA (Emergency Use Authorization) requests to the FDA.”
Self-swabbing versus Clinical Laboratory Worker
While it has been longstanding medical practice to have healthcare workers collect samples for respiratory tract infection testing, the Emory researchers suggest that allowing children to collect their own COVID-19 samples could be one way to reduce the burden of a shortage of healthcare workers.
The researchers also believe pediatric self-swabbing would expand access to diagnostic tests and make it easier to test school-age populations.
“Every minute of a healthcare worker’s time is at a premium,” said senior study author Wilbur Lam, MD, Professor of Pediatrics and Biomedical Engineering, Emory University and Georgia Tech, in a National Institutes of Health (NIH) press release. “Why not allow a kid to self-swab? It’s a win-win! They would rather do it themselves and it frees up the healthcare worker to do other things,” he added.
In 2020, a Stanford University School of Medicine study published in JAMA showed test samples collected by adults who swabbed their own nasal passages were as accurate as those collected by healthcare workers. This study involved 30 participants who had previously tested positive for COVID-19.
Though the Emory University and Stamford University studies were small, they agreed in their findings which is significant. Clinical laboratory executives and pathologists should expect this trend toward direct-to-consumer and other forms of self-testing to continue, even among young patients.
These findings may be useful to clinical laboratory professionals when physicians want guidance in effective treatments for COVID-19 patients, particularly when there are concerns about a rebound of the infection
Drug interactions are a major concern for physicians and clinical laboratories. That is especially true given the push for nearly universal COVID-19 vaccinations and boosters. Now, a study conducted in Denmark may show that the use of Paxlovid as an antiviral drug to treat early SARS-CoV-2 infection could trigger drug-drug interactions (DDI) in some patients.
For clinical laboratory managers, insights into the issues associated with Paxlovid may be useful in helping client physicians diagnose their patients and anticipate possible negative drug reactions where other anti-viral drugs are involved.
Also of interest to medical laboratory leaders is the fact that the federal Centers for Disease Control and Prevention (CDC) in May released a Health Alert Network (HAN) Health Advisory about the potential for COVID-19 rebound after Paxlovid treatment.
COVID-19 Rebound, according to the CDC, “has been reported to occur between two and eight days after initial recovery and is characterized by a recurrence of COVID-19 symptoms or a new positive viral test after having tested negative.”
In an article she penned for STAT, Joan Susan Bregstein, MD (above), a pediatric emergency medicine physician and professor of pediatrics at Columbia University Irving Medical Center in New York, wrote, “Is Paxlovid worth it? The CDC advisory states in black, bold, and no uncertain terms that, despite the risk of rebound COVID, ‘Paxlovid continues to be recommended for early-stage treatment of mild to moderate COVID-19 among persons at high risk for progression to severe disease.’ But the definition of ‘high risk’ in this situation has been a moving target since the first days of COVID-19.” Clinical laboratory leaders can attest to the accuracy of that statement. (Photo copyright: Columbia University.)
Do Anti-Viral Drugs Interact with Other Medications?
Paxlovid is the retail name for a combination of two anti-viral drugs: nirmatrelvir and ritonavir. The medication for COVID-19 was developed by American pharmaceutical company Pfizer (NYSE:PFE) and received Emergency Use Authorization from the US Food and Drug Administration in August of this year.
The drug is taken orally for five days by people who test positive for the SARS-CoV-2 coronavirus to head off disease progression as well as serious illness, according to the CDC advisory.
But a “sizeable proportion” of elderly people are on medications that could interact with Paxlovid, Reuters reported.
“Two oral antiviral drugs—nirmatrelvir/ritonavir (NMV/r) and molnupiravir—have been approved for early outpatient treatment of COVID-19 to prevent severe disease. Ritonavir, contained in NMV/r is known to have significant DDI with several drugs frequently used by the elderly. This communication puts the problem with DDI with oral antiviral COVID-19 treatment into perspective,” the study authors wrote.
Their analysis of prescription data from Denmark residents found “extensive use of drugs likely to interact with NMV/r” as follows:
Anticoagulants (blood thinners): used by 20% of people over age 65 and by 30% of people over 80.
Statins (cholesterol-lowering medications): taken by 15% to 18% of people over 65.
Analgesics (for pain), calcium channel blockers (used to decrease blood pressure in patients with hypertension), or digoxin (used to treat heart conditions): taken by 20% of those studied.
In their paper, the researchers offered guidance to physicians. “Before prescribing NMV/r, the patient’s full medical history, including herbals and over-the-counter and recreational drugs, must be known and co-treatment carefully managed by the treating physician or by a specialist to avoid detrimental effects.”
However, one infectious disease specialist told Scientific American it may just take the elderly who were taking Paxlovid more time to completely get over COVID-19.
“Being of an elderly age and then having other risk factors—like diabetes, heart disease, kidney disease, or some sort of cancer—does put you at higher risk of rebound,” Aditya Shah, MBBS, Mayo Clinic Infectious Disease Physician and Researcher, told Scientific American.
That study’s researchers retrospectively reviewed 92 million electronic health records (EHR) from US patients. They found most people (11,270) had been treated with Paxlovid. However, 2,374 patients took molnupiravir, which also was granted EUA status by the FDA and is marketed as Lagevrio.
That COVID-19-rebound study found:
After nirmatrelvir/ritonavir (Paxlovid) treatment: 3.53% had rebound infections, 2.3% with rebound symptoms, and .44% were hospitalized.
After molnupiravir (Lagevrio) treatment: 5.86% had rebound infections, 3.75% with rebound symptoms, and .84% were hospitalized.
“Patients who took molnupiravir were significantly older and had more comorbidities than those who took Paxlovid,” the researchers wrote. “Results further suggest that rebound was not unique to Paxlovid and may be associated with persistent viral infection in some patients treated with either of these two antivirals. There has been more attention to COVID-19 rebound following Paxlovid treatment than molnupiravir, which may be attributable to more people being treated with Paxlovid,” they concluded.
Clinical Laboratories Can Guide Doctors
In an article she penned for STAT, titled, “Paxlovid Rebound Happens, Though Why and to Whom Are Still a Mystery,” Joan Susan Bregstein, MD, a pediatric emergency medicine physician and professor of pediatrics at Columbia University Irving Medical Center in New York, wrote of COVID-19 rebound, “My emergency medicine physician colleagues are seeing tons of it. Although people tend to think of medical care as something that is certain, it is actually a real-time experiment. Paxlovid, like a lot of COVID-19 care, is a reminder of this.”
Similarly, Mayo Clinic’s Shah acknowledged difficulty in identifying a COVID-19 rebound case. “You need real documentation of three tests—a positive, a negative, a positive—and clear documentation of symptoms—all symptoms gone, symptoms come back,” Shah told Scientific American.
Thus, clinical laboratories play a vital role in diagnosing and treating COVID-19 rebound patients, because that is what clinical labs do: test, document, and report. And as the study of the Danish population pointed out, doctors need guidance as they prescribe oral antivirals to COVID-19 patients who are on other drugs and at possible risk of drug-drug interactions.
Issues arose after a pathologist who once was the clinical laboratory director at Theranos suggested his testimony during the trial was misconstrued by federal prosecutors
Just when clinical laboratory directors and pathology group managers thought they could look forward to a world without an ongoing Theranos fraud trial, company founder and ex-CEO Elizabeth Holmes requested a new trial. Her request was based on comments by pathologist and former Theranos lab director Adam Rosendorff, MD, that he was remorseful about his testimony in Holmes’ fraud trial.
Now, it appears the court will hear Holmes’ argument. On October 4, a federal judge agreed to delay Holmes’ sentencing to consider new evidence that was submitted to the court in a September filing and further evaluate her request for a new trial.
In that filing, Holmes claimed that Rosendorff visited her home on August 8 to express regret over his testimony. According to Holmes, Rosendorff alleged that his statements had been misconstrued by prosecutors at her trial. He stated that “he tried to answer the questions honestly, but that the prosecutors tried to make everyone look bad” and he now feels like “he had done something wrong,” The Guardian reported.
Theranos founder and ex-CEO Elizabeth Holmes (left) as she was seen entering the federal courthouse in San Jose, Calif., on Sept. 1 to argue that her trail verdict should be overturned due to new comments from pathologist and former lab director Adam Rosendorff, PhD, who expressed remorse over his original testimony. Clinical laboratory managers may want to track these new developments in the unfolding saga of Theranos and Elizabeth Holmes. (Photo copyright: AP/Daily Mail.)
Pathologist Rosendorff’s Testimony about Holmes
Rosendorff, the pathologist who served as the CLIA laboratory director at Theranos for several years, was a major witness for the prosecution in the Holmes trial which lasted nearly four months. During his four-day testimony, he contended that Holmes was cognizant of accuracy issues with Theranos’ blood-testing device and that she intentionally misled both investors and patients.
In January, a jury found Holmes guilty of three counts of wire fraud and one count of conspiracy to commit wire fraud for lying to investors about Theranos products. The jury of eight men and four women deliberated for more than 50 hours over seven days to arrive at the verdict. She faces up to 20 years in prison and a fine of $250,000 plus restitution for each count.
In September, US District Judge Edward Davila, who presided over Holmes’ original fraud trial, declined to overturn the guilty verdict.
The new hearing regarding the issues with Rosendorff’s testimony will occur on October 17, the original date of Holmes’ sentencing. Davila stated that he has scheduled an entire day for hearing, but that he expects it to take less than the full allotted day.
Judge Wants to Know If Former Theranos Lab Director Told the Truth
If her request for a new trial is denied, Holmes will be sentenced sometime between November and January. She is currently free on bail while awaiting her sentencing.
Regarding the latest development, Davila stated that it was unusual for a witness to appear at a convicted defendant’s home. “I will say I haven’t seen a case where this happened before,” Davila told CNN.
“What the court wants to know is, Dr. Rosendorff, do you feel the government manipulated you in the preparation or in any way in regards to your testimony?” Davila said about what will be covered in the October 17 hearing. “What I want to know is, did you tell the truth?”
After Holmes used Rosendorff’s appearance at her home to request a new trial, the former Theranos lab director filed a sworn declaration with the court on September 21 that he stands by his testimony “in every respect.”
“Nevertheless, I feel compassion for Ms. Holmes and Mr. Balwani, and even more so for the members of their families who were not responsible for their conduct but will be affected by the punishment they may receive,” he wrote.
And so, the saga of Elizabeth Holmes continues. Clinical laboratories will once again get a view into how a lab director’s responsibilities can alter testing outcomes—and fraud trials.
Study also may have found relationship between atherosclerosis and cholesterol
Chinese scientists have developed a cutting-edge method for non-invasively monitoring blood cholesterol levels in humans. The innovative technology utilizes images of skin on hands and may eliminate the need for both invasive venipunctures and fasting for testing cholesterol. Given the large volumes of blood cholesterol tests currently performed by clinical laboratories, this new technology could have significant impact on cholesterol testing if further studies confirm its capabilities.
Notably, the Chinese researchers have apparently already developed a lab analyzer to perform the procedure and it is being used in clinical care. However, in the United States and other countries, this technology will require additional clinical studies and regulatory review before clinical laboratories would be able to use it in daily patient care.
The cholesterol sensing system consists of a detection reagent associated with a fluorescent group that binds to skin cholesterol, and a detection device. Cholesterol levels are easily obtained from the skin, according to the researchers, by analyzing the manner in which the skin absorbs and scatters light via a scanner.
Should this technology be validated for clinical care, it could replace other invasive clinical laboratory tests for cholesterol measurement.
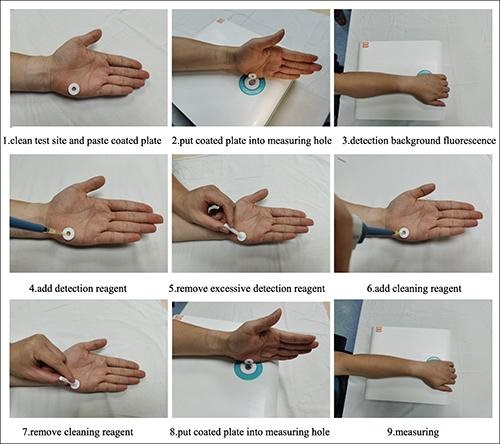
The series of images above, taken from the researchers’ Lipids in Health and Disease published study, demonstrates how their non-invasive clinical laboratory test for total blood cholesterol is performed. Non-invasive clinical laboratory tests for monitoring biomarkers in the blood are always preferred by patients over veinous punctures and fasting. (Photo copyright: Hefei Institutes of Physical Science, Chinese Academy of Sciences.)
First Evidence of Relationship between Cholesterol and Atherosclerosis
“Just put your hands on, and the system will tell you the cholesterol data,” Yikun Wang, PhD, Professor, Department of Physical Sciences, Hefei Institutes of Physical Science, Chinese Academy of Sciences, and leader of the research team, told Diagnostics World. “Cholesterol is one of several types of fats (lipids) that play an important role in human body, we can track your fats in this simple way.”
To perform the testing, clinicians first clean the test site located on the fleshy edge of the palm of the hand with an alcohol swab. A patient’s non-dominant hand is used for the test as the skin on that hand is typically less abrasive and contains fewer melanocytes, which allows for more stable results. A plastic-coated annulus is then applied to the test site and the examined portion is positioned on the measuring hole of the detection system to measure the background light spectrum of the skin.
Once the background signal is ascertained, the detection reagent is added to the annulus until it is full. After 60 seconds, any excess detection reagent is removed from the annulus. A cleaning reagent is then added to the annulus for 30 seconds and removed with a sterile cotton swab. The treated portion of the skin is then placed over the measuring hole of the detection system and two spectrums of light are compared to measure the skin cholesterol, which accurately correlates to the cholesterol in the bloodstream.
“Compared to in-situ detection used in the previous clinical research, our device may offer more accurate results for we can avoid the influence of pressure and skin background differences [person to person],” Wang said. “Study results offer the first evidence of a relationship between skin cholesterol and atherosclerotic disease in a Chinese population, which may be of great significance to researchers around the world.”
Initially, 154 patients diagnosed with acute coronary syndrome (ACS) between January 2020 and April 2021 were involved in the study. However, only 121 of those patients were included in the final study with the remaining being excluded due to at least one of the following criteria:
Severe hepatic (liver) or renal (kidney) insufficiency, and
Obesity.
Clinician Use Can Affect Accuracy of Test
Developed by researchers from the Hefei Institutes of Physical Science Chinese Academy of Sciences, and the University of Science and Technology of China, the researchers noted that how clinicians operate the device can have an impact on the accuracy of the test results.
“A critical step in the [testing] process that is subject to operator variability is blotting, which requires the operator to remove an unbound detector from the palm before adding the indicator,” Wang told Diagnostics World. “Excess residual indicator solution can result in falsely increased skin cholesterol levels. Considering this, we are planning to develop a simplified and standardized blotting procedure.”
Millions of people in the US live with illness that requires regular monitoring of blood cholesterol. Normal total cholesterol should be less than 200 milligrams per deciliter (mg/dL). According to the federal Centers for Disease Control and Prevention (CDC), nearly 94 million US adults over the age of 20 have total cholesterol levels higher than 200 mg/dL and 28 million adults have total cholesterol levels higher than 240 mg/dL. In addition, 7% of children and adolescents between the ages of six and 19 have high cholesterol. For these reasons, cholesterol testing represents a substantial portion of the clinical laboratory tests performed daily in this country.
This new non-invasive technology for monitoring total blood cholesterol in humans could greatly benefit patients, especially if it eliminates the need for venipunctures and fasting prior to testing. Clinical laboratory managers and pathologists may want to follow the progress of this new cholesterol testing technology as it demonstrates its value in China and is submitted for regulatory review in this country.
Clinical laboratories and pathology groups can benefit from knowing how genetic testing is being used for other than medical testing purposes
It is useful for pathologists and clinical laboratory managers to be aware of the different ways genetic testing and DNA sequencing is being conducted. That’s because a genetic test for one purpose—such as identifying an individual’s relatives and connection to a region or a cultural group—might generate data that could become part of that person’s medical care.
Thus, an ongoing genetic study in South Africa highlighting the issue of so-called “helicopter research” will be informative for Dark Daily’s readers.
Also known as “neo-colonial science,” helicopter research describes when scientists from wealthy countries perform research in lower-income countries in ways that may be deemed exploitative or disrespectful to local populations.
“Scientists conduct helicopter research when they collect data from developing countries and marginalized communities with little to no involvement from local researchers and community members,” wrote researchers Dana Al-Hindi, and Brenna Henn PhD, in an article for The Conversation. “Helicopter research also occurs when researchers take data out of the country they collected it from without either providing benefit to or sharing the results with the community.”
In an article for The Conversation, UC Davis researchers Brenna Henn, PhD (left), and Dana Al-Hindi (right), wrote, “While we have learned a great deal from these communities, we have been unable to fulfill a common request: providing them their individual genetic ancestry result. In our attempts to overcome the logistical challenges of providing this information, we’ve grappled with the common question of how to ensure an equitable balance of benefits between researchers and the community they study. What we’ve found is that there is no easy answer.” Clinical laboratories will want to remember the term “Helicopter Research” in relation to these types of studies. (Photos copyright: UC Davis/The Conversation.)
The South Africa study, conducted over the past 12 years, aims to use genetic data “to help unravel the history and prehistory of southern Africans and their relationship to populations around the world,” the authors wrote in The Conversation.
The researchers have been using the genetic data to trace the ancestry of indigenous Khoekhoe and San peoples in South Africa as well as other populations that self-identify as “Colored.”
“Early European colonizers initially used this term to refer to indigenous Khoekhoe and San groups long before it was codified by the apartheid government in 1948,” the researchers wrote. “It persists today as an ethnic category, broadly encompassing Khoe-San groups, various East African, Indian, and Southeast Asian populations brought by the slave trade, and people of mixed ancestry.”
Challenges Sharing Genetic Data with Study Participants
Participants in the study have asked to see their personal genetic ancestry results, but the researchers noted several challenges, including local restrictions and the difficulty of presenting complex data in “an accessible and digestible form.” So, the researchers partnered with consumer-focused genetic testing company 23andMe (NASDAQ:ME).
23andMe provided additional funding for the research, assisted the researchers in community outreach, and “expanded our ability to ‘capacity-build’—that is, to make sure that the knowledge and skills we gain are shared with local institutions,” Henn and Al-Hindi wrote in The Conversation. They added that they are still dealing with questions about whether their efforts to provide equitable benefits are sufficient.
“Our research team, local collaborators, and 23andMe are all concerned about how to best address the risk of helicopter research, coercion, and any unknown risks that may arise from disclosing personal ancestry results,” they wrote.
Cape Town Statement on Fostering Research Integrity
The issue of helicopter research was a major focus at the 7th World Conference on Research Integrity (WCRI), held May 29-June 1 in Cape Town, South Africa. It was the first WCRI to be held in Africa and adopted the theme “Fostering Research Integrity in an Unequal World.”
One outcome of the conference will be an effort to produce what is known as the Cape Town Statement on Fostering Research Integrity. The statement will “highlight the importance of fairness in international research partnerships,” noted Research Professional News.
The statement “compels institutions and researchers alike to act on their responsibilities to promote equity, diversity, and fairness in research partnerships,” conference speaker Retha Visagie, DCur, told the publication. She leads the Research Integrity Office at the University of South Africa.
Conference co-chair Lyn Horn, PhD, director the Office of Research Integrity at the University of Cape Town, told the publication that it could take up to a year before a draft of the statement is ready for comment.
One overarching goal will be to “demonstrate why inequity and unfair practices in research collaborations and contexts is a research integrity (RI) matter,” the authors wrote. “Second it must identify some key values or principles and action guides that will address the issue of equity and fairness in research within the context of the complete research life cycle from research agenda setting and call to proposal development, through grant application, allocation and management of funding, data production, analysis, management and sharing, to outputs, translation, and evaluation.”
Another conference speaker, Francis Kombe PhD, told attendees the statement will offer guidance specifically to institutions such as universities, journals, and funding organizations, the journal Science reported. That stands in contrast to earlier statements on helicopter research, which were geared more toward individuals and small groups.
How any of this will impact clinical laboratories and pathology groups remains unclear. Nevertheless, it is worthwhile knowing how gene sequencing is being used by researchers for purposes other than to guide diagnoses and treatment of patients.