Feb 12, 2018 | Digital Pathology, Instruments & Equipment, Laboratory Management and Operations, Laboratory News, Laboratory Operations, Laboratory Pathology, Laboratory Testing
Doctors’ advocacy organization praises potential of ‘My Health Record’ but voices concerns about functionality, interoperability, and added burden placed on providers
Australia’s goal of implementing a nationwide electronic health record (EHR) system received a major boost when the country’s largest pathology laboratories signed agreements with the Australian Digital Health Agency (ADHA) to join the project. But the My Health Record system has yet to fully win over providers as the Australian Medical Association (AMA) raises concerns over functionality, interoperability, and the added burden placed on healthcare providers.
ADHA Chief Executive Tim Kelsey praised the addition of pathology and diagnostic organizations to the My Health Record platform. In Australia, pathology laboratory is the term to describe what are called clinical laboratories in the United States.
“The largest diagnostic organizations in Australia have now agreed to share their test reports with Australian consumers,” Kelsey said in an ADHA news release. “We are working to deliver a My Health Record for all Australians next year, unless they choose not to have one. Health consumers will benefit from this significant commitment by the pathology industry and their software partners.”

Australian Digital Health Agency CEO Tim Kelsey says his agency in 2018 will be creating a universal electronic health record for all the country’s 24.8 million citizens, though patients will have the option to opt out of the My Health Record project. He called the “significant commitment” of pathology labs to the project a major step forward. (Photo copyright: ADHA.)
In May 2017, Sonic Healthcare, Australia’s largest pathology provider, became the first private pathology company to join the My Health Record initiative. That news was followed by agreements between the ADHA and pathology companies Primary Health Care, Australian Clinical Labs, and seven other software vendors and pathology laboratories, including:
The ADHA also finalized service agreements with additional software companies that will enable diagnostic imaging providers to link up to My Health Record by the end of 2018.
AMA Says My Health Record Lacks Functionality and Critical Features
In 2012, Australia announced the roll out of the Personally Controlled Electronic Health Record, the original initiative to create a citizen-controlled secure online summary of health information, which later was renamed My Health Record. According to The Australian, more than 5.3 million Australians are now using My Health Record, a 500% increase in the number of shared health summaries uploaded in 2016-2017 and a 200% rise in interoperability with private hospitals.
Royal College of Pathologists of Australasia President Bruce Latham, MBBS, welcomed the announcement of the increased functionality for My Health Record.
“The Australian pathology sector has been working in support of the national eHealth agenda for a number of years,” Latham stated in the ADHA news release. “Work is now progressing to connect both public and private labs to the My Health Record, and patients nationally will start to see their pathology reports in their My Health Record.”
Developers and program administrators of My Health Record predict it will generate savings of AU$123 million from:
- Reduction in adverse drug events;
- Fewer duplicated diagnostics tests; and,
- Cost savings by 2020-2021.
However, the AMA, Australia’s doctors’ advocacy group, outlined its concerns about My Health Record in a Pre-Budget Submission to the Australian federal government. While praising the project’s potential to “not only save money, but save lives,” the AMA argued the national repository of healthcare information needs improved features and functionality to meet its potential.
“… more work is required,” the AMA wrote. “The return on investment will hinge in the short term on ease of use for medical practitioners who upload the clinical data. Interoperability with the multiple software packages used across the medical profession and broader health sector must be seamless.
“Problems uploading specialists’ letters, poor search functionality, time-consuming adaptations to existing medical practitioner work practices, or inappropriate workarounds will erode clinical utility and deter doctor use—and, more importantly, take time away from focusing on the patient,” the AMA concluded.
Automatic Enrollment Concerns AMA
My Health Record began as a self-register model, but as the program goes nationwide in 2018, it will do so using an “opt-out” model. This means citizens will be enrolled automatically unless they ask to be removed from the program. According to the ADHA, the automatic creation of My Health Record for all Australians will begin in mid-2018. The government’s goal is to provide access to My Health Record to all 24.6 million Australians by June 30, 2018.
The federal government’s switch to an opt-out system for My Health Record drew concerns from the AMA.
“Doctors do not have time to talk their patients through the My Health Record arrangements for opt-out, privacy, [or] setting access controls in standing consent for health providers to upload health information. This is the work of the government. Doctors must be allowed to focus on what they do best—caring for patients,” the AMA stressed.
Clinical Laboratories Have Stake in Outcome
According to Healthcare IT News Australia, the Australian government has spent AU$2 billion ($1.53 billion USD) so far developing what could become a white elephant if general practitioners and hospital groups don’t see a clinical benefit in its use.
If Australia is successful in creating a fully-functioning and widely-used national repository for health information, it will be among the first countries to do so. In 2002, the United Kingdom (UK) kicked off a nearly decade-long effort to create a national EHR system for the UK’s single-payer tax-supported health system. Ultimately, the government pulled the plug on the initiative after spending 12.7 billion pounds ($17 billion USD) trying to complete the project.
That result, and lessons learned from Australia’s experience, should inform American healthcare policy makers. It remains a daunting effort to implement a single electronic patient health records system. Of course, pathologists and clinical laboratory administrators have an interest in this issue, since medical laboratory test data represents the largest proportion of an individual patient’s permanent health record.
—Andrea Downing Peck
Related Information:
Australia’s Largest Pathology Labs Sign Up to My Health Record
Private Pathology Reports to Go Live in My Health Record
E-health Revolution Gather Pace as more Services Pledge their Backing
Australian Medical Association Pre-Budget Submission 2018-19
National Expansion of My Health Record in 2018 Confirmed in Budget Announcement
GPS and Hospitals Claim My Health Record Not Fit for Purpose as Alarming Low Usage Figures Are Released
Jan 17, 2018 | Coding, Billing, and Collections, Instruments & Equipment, Laboratory Instruments & Laboratory Equipment, Laboratory Management and Operations, Laboratory News, Laboratory Pathology, Laboratory Testing, Management & Operations
Moving to market are the newest generation of LIMS products designed to serve clinical laboratories while supporting quality reporting initiatives and new sources of revenue
It was Bob Dylan who made a big hit out of the song, “The Times, They Are A-Changin’.” The same could be said for the next generation of software products designed for use by medical laboratories.
To be fully successful, these next-generation laboratory information management systems (LIMS) must be radically different than the generations that came before. For example, medical laboratories are frustrated with the many limitations of older LIS products that still incorporate software technologies that date back to the 1980s and 1990s, such as MUMPS, which stands for Massachusetts General Hospital Utility Multi-Programming System.
But the newest LIMS products must do more than simply incorporate the latest technologies in software and cloud-based services. They must support all the ways that clinical laboratories and anatomic pathology groups generate increased revenue. More specifically, all medical laboratories will be generating vast quantities of molecular and genetic data. Therefore, an effective LIMS must be capable of capturing that data while also enabling the lab to perform certain healthcare big data analyses in support of the referring physicians and parent hospitals.
There also will be the need for medical laboratories to use their LIMS capabilities to support the data reporting requirements of Medicare and private health insurers. Payers increasingly want providers to report their quality monitoring, patient outcomes, and certain cost-of-care parameters. All these are functions that older LIS (laboratory information systems) products were not developed to provide.
Anatomic pathology group stakeholders and clinical laboratory managers understand the vital importance of their LIMS. Laboratory and healthcare workflows depend on the system’s:
- efficiency;
- scalability that supports the growth of the lab and medical practice; and,
- flexibility to interface with modern, point-of-care telehealth technologies in ways that enable labs and practices to engage in today’s precision medicine healthcare initiatives.
The more immediate need is for a LIMS to be capable of supporting Medicare’s Quality Payment Programs (QPPs), primarily the MACRA Merit-based Incentive Payments System (MIPS). Most physicians, including pathologists, will participate in MIPS. The first Medicare incentives or penalties will be paid next year, based on 2018 metrics and performance.
Given all these changing demands of advanced software technologies and the need for medical laboratories to participate in various value-based revenue programs, how might a LIMS empower labs to ensure success and increased revenue?
Quality Payment Programs and Merit-based Incentives
As part of the shift toward value-based care, the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) works to drive down costs and increase quality within both care and laboratory environments. MACRA establishes a data-driven payment system to reimburse service providers based on the outcome of services and care episodes, instead of the volume of services delivered or billed.
Combined with reduced payments, MACRA’s incentives and penalties, and Medicare’s QPP/MIPS payment programs, pressure has been increased on healthcare providers and medical laboratories alike. Thus, technology that gives labs a competitive edge is essential for thriving in an ever-evolving and increasingly competitive marketplace.
Meeting MACRA Goals with a Laboratory Information Management System
While electronic health record (EHR) systems have helped to consolidate patient protected health information (PHI), they do little to address the real-time creation of laboratory data and the accessibility of the massive volume of lab-related data stored in the average patient’s medical files.
A LIMS, however, helps to consolidate all this data in an easily accessible and powerful system. Some LIMS even combine with telehealth technologies to make data actionable and available at the point-of-care.
In this type of LIMS, laboratories, physicians, and other care providers all access the same dataset to ensure information is relayed quickly and efficiently. Interaction takes place using cloud-based interfaces, such as mobile apps or web portals. This ensures access to patient data and laboratory test results in a variety of locations without dependence on proprietary communications systems or hardware.
From bustling ERs and surgical wards to phlebotomists visiting long-term care facilities and mobile clinics, collecting and retrieving data becomes streamlined and accessible virtually anywhere.
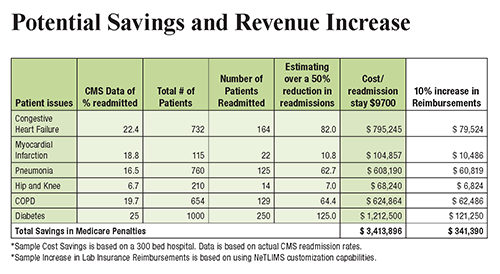
The chart above illustrates how a LIMS offers increased potential to automate processes and scale operations while keeping physicians, patients, and other critical parties up to date. This increase in efficiency and access to data empowers providers to reach improved patient outcomes and reduce hospital readmission rates, increasing revenue for both clinicians and clinical laboratories. (Graphic copyright: NetLIMS.)
When implemented properly, a LIMS also helps laboratories and healthcare facilities meet the terms of MIPS. This reduces Medicare penalties and ensures payment adjustments, which improve revenue streams even further.
Understanding LIMS and Cloud-Based Lab Systems
To help outline and explain the benefits of a LIMS for laboratories and healthcare facilities, The Dark Report, in conjunction with NetLIMS, a global provider of laboratory information management systems to hundreds of hospitals and commercial laboratories worldwide, has produced a free white paper titled, “The Path to More Revenue: Cloud-Based LIMS, Mobile Apps, and Point-of-Care Telehealth.”
- This white paper addresses critical concerns, including:
- Overviews of new technologies;
- The impact of value-based programs on the lab market;
- The importance of MACRA and MIPS adherence;
- How technology, such as a LIMS, can help labs achieve improved efficiency; and,
- Tips on choosing a LIMS vendor to maximize ROI.

To download your free copy of the whitepaper click on this link: Or, copy this URL into your browser: https://www.darkdaily.com/whitepaper/the-path-to-more-revenue-cloud-based-lims-mobile-apps-and-point-of-care-telehealth .
Thanks to advances in LIMS design and development, remote patient digital therapeutics, and cloud-based technology, healthcare providers now have unprecedented opportunities to better manage the health of patients with chronic conditions. In addition, it can help you achieve better efficiency, economics, and compliance with MACRA.
This free white paper is your first step toward significantly reducing hospital readmission rates, bridging the gap between labs, physicians, and other healthcare providers they serve, and positively affecting patient outcomes, improving quality measures, and maximizing reimbursements for all services you provide.
—Jon Stone
Related Information:
The Path to More Revenue: Cloud-Based LIMS, Mobile Apps, and Point-of-Care Telehealth
How Close Is the End of Private Practice Pathology as We’ve Known It?
Attention Anatomic Pathologists: Do You Know Medicare Is Prepared to Change How You Are Paid, Beginning on January 1, 2017?
Innovator Hospitals Bring ICUs into the Info Age, Using New Design Approaches that involve Medical Laboratory Tests

Jan 11, 2018 | Laboratory Hiring & Human Resources, Laboratory Management and Operations, Laboratory News, Laboratory Operations, Laboratory Pathology, Laboratory Testing, Management & Operations
At institutions such as University of Texas Medical Branch, Galveston, and Vanderbilt University Medical Center, pathologists are using diagnostic management teams to improve patient outcomes while lowering the medical costs
Diagnostic Management Teams are a hot concept within the medical laboratory profession. In fact, a new annual DMT conference in Galveston, Texas, is the fastest-growing event in the clinical laboratory industry. This year’s Diagnostic Management Team Conference will take place on February 6-7, 2018, and is produced by the Department of Pathology at the University of Texas Medical Branch (UTMB) in Galveston.
In simplest terms, a diagnostic management team (DMT) is described by pathologist Michael Laposata, MD, PhD, as “involving a group of experts who meet daily and focus on the correct selection of laboratory tests and the interpretation of complex test results in a specific clinical field. Typically, DMTs are led by pathologists focusing on the diagnosis of a specific group of diseases, along with physicians and other lab experts involved in the disease or health condition that is the focus of the DMT.”
How Pathologists Use Diagnostic Management Teams
“What differentiates a DMT are two changes from the classic diagnostic pathway,” continued Laposata. “First, the ordering physician gets assistance in selecting the correct tests. This can be done in several ways, such as creating expert-driven algorithms that are updated regularly to manage utilization of laboratory tests and dramatically minimize overuse and underuse. Use of such algorithms with reflex testing makes it easy for treating healthcare providers to order the right tests and only the right tests.
“The second key difference in this new diagnostic pathway is that, within the DMT’s specific clinical context, an expert-driven, patient-specific interpretation of the test results in a specific clinical context is generated by the members of the DMT,” he said. “This requires the knowledge of a true expert—not someone who may have a general idea about the meaning of a particular laboratory test result—and the participation of someone to help that expert search the medical record for relevant data to be included in the interpretation.
DMTs Typically Organized to Support Specific Diseases or Health Conditions
He pointed out that the DMT has a rather simple organization. There is a front-end and a back-end. The front-end starts when “physicians order tests by requesting evaluation of an abnormal screening test or clinical sign or symptom,” explained Laposata. “Upon receiving that request, the expert physician and colleagues in the DMT then synthesize the clinical and laboratory data and provide a narrative interpretation based upon medical evidence. This happens not only when specifically requested by the referring physician, but also for every case handled by the DMT.”

Diagnostic Management Teams are making significant contributions at the University of Texas Medical Branch (UTMB), Galveston. Pictured above, the members of UTMB’s coagulation DMT are (L-R): Jack Alperin, MD; Michael Laposata, MD; Aristides Koutrouvelis, MD; Camila Simoes, MD; Chad Botz, MD; Aaron Wyble, MD: and Jacob Wooldridge, MD. (Photo copyright: University of Texas Medical Branch, Galveston.)
The back-end of the process involves the DMT conducting an “expert-driven, patient-specific interpretation of the test results in a specific clinical context.” Here is where the participating clinical experts—supplemented by staff who conduct an informed search of the medical record to identify and collect data relevant to the diagnosis—sift through this much richer quantity of information to develop the diagnosis.
Overworked Physicians Value the Expertise, Diagnostic Accuracy of DMTs
Laposata points out that individual physicians who already may be overworked in their daily routines generally welcome the help of DMT experts who are up-to-date on the current literature, and who have decades of experience in these diseases and health conditions. He likes to point out that, in coagulation alone, a physician could have as many as 60 to 90 tests that can be ordered. He also notes that typical primary care physicians, for example, are generally not experts in selecting the best coagulation test to order for every group of symptoms, nor do they know how to order the most appropriate reflexive test to continue the diagnostic pathway.
Knowing how to interpret the results of the 60 to 90 different coagulation tests is equally challenging to most physicians.
Over the course of his career, Laposata has signed out more than 50,000 cases in the field of coagulation. “Every positive case that identified a diagnosis resulted in an earlier and more accurate diagnosis,” stated Laposata. “Every case negative for coagulopathy allowed the treating healthcare provider to focus on a diagnosis other than one related to bleeding and thrombosis.”
Using Clinical Laboratory Data to Improve Patient Outcomes, Reduce Costs
There are other reasons why a growing number of medical lab administrators and clinical pathologists believe that DMTs are the right solution at the right time. One reason is the steady reduction in reimbursement from Medicare and private payers. Another is the trend to measure and publish the quality metrics of hospitals and individual physicians.
There are ever more quality metrics that include diagnostic accuracy and total cost per healthcare encounter. Diagnostic Management Teams are proven to improve diagnostic accuracy and ensure the patient gets the right therapy faster. Both of these benefits contribute to substantial reductions in the cost per healthcare encounter.
Pathologists and clinical laboratory professionals interested in learning more about diagnostic management teams have two opportunities.
At the Galveston Island Convention Center on Feb. 6 -7, 2018, the second annual Diagnostic Management Team Conference will take place. Last year, several hundred-people attended. Information can be found at: http://www.dmtconference.com/.
Special Webinar on Diagnostic Management Teams on January 17
For those interested in learning via webinar, Dark Daily is presenting Laposata and his colleagues in a special session on Wednesday, Jan. 17 at 1:00 PM EASTERN. It is titled, “Using Diagnostic Management Teams to Add Value with Clinical Laboratory Tests and Pathologists’ Expertise.”
During this valuable webinar, you’ll hear from three experts. First to speak will be Michael Laposata, MD, PhD. He will provide you with a detailed overview of DMTs, including:
- How to assemble the right team;
- How to engage with referring physicians; and,
- How to work through individual cases.
Laposata will introduce you to the structure and organization of effective diagnostic management teams, organized around a specific disease or health condition and made up of pathologists, other lab scientists, and physicians who are expert in their particular clinical field. The objective of the DMT is to meet daily with the goal of coming up with faster, more accurate diagnoses in support of a patient’s care team.
Experience from a Diagnostic Management Team Focused on the Liver
Next to speak will be Heather Stevenson-Lerner, MD, PhD, a liver and transplantation pathologist and Assistant Professor, Department of Pathology, UTMB. She will discuss a DMT organized around diseases of the liver. This is a useful, step-by-step description of an effective DMT, illustrated with case studies that demonstrate how diagnostic management teams can make a positive and substantial contribution to improving individual patient outcomes.
The webinar’s third presenter is Christopher Zahner, MD, a resident pathologist at UTMB. He will share how to pull together all the information needed to support DMT interpretations. From the electronic health record (EHR) system to other overlooked sources of useful data, Zahner will explain the most productive ways to assemble any information that will be useful to the diagnostic management team and that will make a positive difference in patient care.
To register for the webinar and see details about the topics to be discussed, use this link (or copy and paste this URL into your browser: https://ddaily.wpengine.com/webinar/using-diagnostic-management-teams-to-add-value-with-clinical-laboratory-tests-and-pathologists-expertise).
This is an essential webinar for any pathologist or lab manager wanting to put the lab front and center in contributing clinical value in ways that directly improve patient outcomes while reducing medical costs. With hospital lab budgets shrinking and fee-for-service payments being slashed, the time is right for your lab team to consider how organizing diagnostic management teams can be the perfect vehicle to demonstrate why clinical lab tests and expertise can be a diagnostic game-changer within your hospital or health system.
And don’t forget, your participation in this webinar can be the foundation for a highly-successful effort to collaborate with physicians and clinical services, to the benefit of both the parent hospital and individual patients. That makes this webinar the smartest investment you can make for crafting your lab’s test utilization and added-value programs in support of clinical care.
—Michael McBride
Related Information:
Webinar: Using Diagnostic Management Teams to Add Value with Clinical Laboratory Tests and Pathologists’ Expertise
Pathologist Michael LaPosata, MD, Delivers the Message about Diagnostic Management Teams and Clinical Laboratory Testing to Attendees at Arizona Meeting
Dec 22, 2017 | Compliance, Legal, and Malpractice, Instruments & Equipment, Laboratory Management and Operations, Laboratory News, Laboratory Pathology, Laboratory Testing
New study published in the Annals of Family Medicine (AFM) indicates that despite efforts to improve EHR usability and efficiency, primary care physicians continue to spend more than 50% of their workdays on computerized physician order entry (CPOE) and other clerical tasks instead of engaging in direct patient care
Do electronic health record (EHR) systems improve or degrade the productivity of physicians? That question has been the subject of robust debate. Now comes a new study in a peer-reviewed journal with a surprising finding: physicians spend up to 50% or more of their workday on EHR-related tasks.
In theory, EHRs offer a wealth of benefits over traditional paper-based systems. In practice, however, between interoperability concerns and implementation costs, they have proven a daunting undertaking for even the largest healthcare systems.
While EHRs might offer easy access to patient data—including medical laboratory records and anatomic pathology reports—this information doesn’t enter itself into databases or make itself instantly accessible. That requires human interaction, which is time consuming and prone to errors.
Thus, research from the American Medical Association (AMA) and the University of Wisconsin revealing that the time it takes to enter data, address communications, and perform other clerical tasks adds up to more than 50% of a physician’s workday is of paramount importance. That’s because physician dissatisfaction and departures from medical practice have increased each year since the EHR revolution began, and reports are the situation is getting worse.
In their retrospective cohort study involving 142 family medicine physicians, published in the Annals of Family Medicine (AFM), Brian G. Arndt, MD, from the School of Medicine and Public Health, Department of Family Medicine and Community Health, University of Wisconsin, et al, reported that clinicians spend 52% of their 11.4-hour workday interacting with an EHR system. On average, nearly 1.5 hours of this EHR interaction occurred outside clinic hours during physicians’ personal time. The researchers assessed interactions using event logs from the Epic EHR system spanning from July 1, 2013, to June 30, 2016.
Researchers validated their data through direct observation of 14 nonresident family medicine physicians from May through June of 2016. This observation showed similar findings. During clinical hours, 60% of physician time related to non-EHR tasks, with 40% of time devoted to EHR tasks.
Documentation Burden Leads to Physician Burnout, Dissatisfaction
“Our family medicine physicians spent 44% of their workday (157 minutes) in the EHR doing clerical and other administrative tasks,” study authors reported. “Computerized physician order entry accounted for 12.1% of their clinic hours (43 minutes) in the EHR. The burden related to order entry has been associated with clinician burnout, dissatisfaction, and intent to leave practice.”
Researchers tracked various tasks and assigned them to categories. Of the tasks tracked, only 32.1% fell under the heading of “medical care.” Reviewing chart notes, chart medications, and problem lists topped medical care tasks.
Review of clinical laboratory results in charts ranked near the bottom, with only 2.5% of the total time spent performing medical care tasks. These tasks, however, could offer opportunities for medical laboratories to help physicians identify opportunities to optimize reporting and test-ordering processes and improve productivity for clinicians who are responsible for most of the data entry burden associated with EHRs.

One potential solution to EHR burnout involves the use of medical scribes who work with physicians during and after a patient’s visit inputting encounter data. Alan Bank, MD, cardiologist at Allina Health, and medical scribe Jaeda Roth, are shown above during a patient visit. Bank told the StarTribune that he’s convinced scribes help doctors get more done and reduce billing errors. (Photo and caption copyright: Elizabeth Flores/StarTribune.)
Researchers also questioned the EHR’s role as a communication or telemedicine hub. “There is insufficient evidence that such asynchronous care improves health outcomes, cost, and overall healthcare use,” they noted.
However, even for intra-practice communications between healthcare professionals, EHRs may not be the most efficient approach. “Face-to-face communication is associated with increased efficiency,” the researchers noted. “Whereas more electronic communication among team members leads to greater clinician and staff dissatisfaction, as well as poorer clinical outcomes and increased healthcare use among patients with coronary artery disease.”
EHR Cost/Benefits Generate Debate
This latest study is not the first to suggest that EHRs are creating problems for clinicians. While there appear to be no trends between studies, multiple researchers have highlighted the workload created by EHR systems in recent years.
In a study published in the Annals of Internal Medicine (AIM), Christine A. Sinsky, MD, of the American Medical Association, et al, analyzed data from the observation of 57 US-based physicians in family medicine, internal medicine, cardiology, and orthopedics.
Comparing data across 430 hours of observation, researchers concluded, “For every hour physicians provide direct clinical face time to patients, nearly two additional hours are spent on EHR and desk work within the clinic day. Outside office hours, physicians spend another one to two hours of personal time each night doing additional computer and other clerical work.”
However, in a 2015 study published in the Annals of Family Medicine (AFM), Valerie Gilchrist, MD, Chair of the Department of Family Medicine and Family Health at the School of Medicine and Public Health, University of Wisconsin, et al, found lower numbers. Observing 27 community-based family physicians across a single practice day, the researchers found that 39% of the practice day on average was devoted to office-based time. Of that time, 61% was spent on medical care related tasks.
Building a Better EHR
While medical laboratories and diagnostic specialists—such as anatomic pathologists—can work with physicians to streamline ordering and reporting processes relating to EHRs, much of the burden comes from how EHR systems are designed and used.
In a 2016 New England Journal of Medicine Catalyst Panel on EHRs, Tait Shanafelt, MD, Director of the Mayo Clinic Department Program on Physician Wellness, noted that one of the most contested features of EHR systems in the US, according to the AMA and Mayo Clinic, is computerized physician order entry (CPOE).
Later in the discussion, Sinsky discussed a recent trip to the UK, where she observed general practitioners (GPs) at the National Health Service (NHS). She noted that most GPs loved their EHRs. However, those EHRs were designed with GP input to best work with an NHS GP’s typical workflows and procedures. She also noted that overall usage is different in the UK, as EHRs there are not tied into billing systems.
As Dark Daily has reported, up to 70% of data stored in a patient’s electronic health record is clinical pathology laboratory related. As newer EHRs replace outdated models, it will remain critical for healthcare professionals—including clinical laboratory professionals who generate most of the data stored in EHRs—to assess, track, and report on what is working with various platforms and what is not.
Communicating this end-user data to EHR developers is essential to designing EHRs that reduce unneeded burden and clerical load on physicians, rather than increasing it.
Clinical laboratories tat wish to take proactive steps might contact physicians and other professionals in their workgroups to tailor data generation, reporting, and ordering processes to the EHRs in use at those practices.
—Jon Stone
Related Information:
Primary Care Doctors Spend More Than 50% of Workday on EHR Tasks, American Medical Association Study Finds
Tethered to the EHR: Primary Care Physician Workload Assessment Using EHR Event Log Data and Time-motion Observations
Study: EHRs Bloat Clerical Workload for Docs
Harried Doctors Hail the Rise of the Medical Scribe
Type and Click Tasks Drain Half the Primary Care Workday
Allocation of Physician Time in Ambulatory Practice: A Time and Motion Study in 4 Specialties
Doctors Wasting Over Two-Thirds of Their Time Doing Paperwork
Physician Activities During Time Out of the Examination Room
Heavy Burden of EHRs Could Contribute to Physician Burnout
Nov 22, 2017 | Instruments & Equipment, Laboratory Instruments & Laboratory Equipment, Laboratory Management and Operations, Laboratory News, Laboratory Pathology, Laboratory Testing, Management & Operations
Industry analysts speculate that Apple might be planning to enter the EHR and healthcare related markets by transforming mobile technologies into gateway devices connected to providers’ EHR systems and patient data
Imagine a mobile device that monitors vitals while connected in real-time to healthcare providers, electronic health records (EHR), and clinical laboratories. One that measures the physical condition and emotional state of the user by casting light onto skin, and then records and transmits it with a swipe of the touch screen. Would such an innovation change how patients expect to interact with their providers? And how physicians, anatomic pathologists, and medical laboratories receive data from their patients? Certainly.
This is why US patents recently granted to Apple have caught the attention of industry analysts. Some speculate that the tech giant is planning to enter the mobile healthcare monitoring device, EHR, and healthcare data storage markets, as reported at Becker’s Health IT and CIO Review and Patently Apple.
How this would affect medical laboratories and anatomic pathology groups remains to be seen. But where Apple goes, industries follow. Thus, it’s worth following the company’s activities in the healthcare market.
Bringing Clinical Data, Medical Laboratory Test Results, to iPhone
Mobile devices launched the era of consumer-grade fitness wearables. It’s not uncommon for a smart phone or watch to capture and store a range of health data generated by users. This can include everything from heart rate and sleeping patterns to dietary logs and fertility tracking. But, to date, much of that healthcare data is user generated and does not integrate in any meaningful way with the majority of EHR systems. Nor does it enable communications with primary care providers or diagnostic services—such as medical laboratories or pathology groups.
This may soon change.
According to a CNBC report, a unit at Apple is “in talks with developers, hospitals, and other industry groups about bringing clinical data—such as detailed lab results and allergy lists—to the iPhone, according to a half-dozen people familiar with the team.”
The report states that Apple:
· “Wants the iPhone to become the central bank for health information;
· “Is looking to host clinical information, such as labs and allergy lists, and not just wellness data; and,
· “Is talking with hospitals, researching potential acquisitions, and attending health IT industry meetings.”
Christina Farr, the report’s author, predicts that Apple could be preparing to apply its music industry model to the healthcare industry by, “Replacing CDs and scattered MP3s with a centralized management system in iTunes and the iPod—in the similarly fragmented and complicated landscape for health data.”
Former National Coordinator of Health IT for the Department of Health and Human Services, Farzad Mostashari, MD, ScM, rather enthusiastically noted the significance of the move, stating, “If Apple is serious about this, it would be a big f—ing deal.”

At a special event in September, Apple COO Jeff Williams (above) announced Stanford Medicine’s Apple Heart Study, which uses “data from Apple Watch to identify irregular heart rhythms, including those from potentially serious heart conditions like atrial fibrillation,” and, according to Williams, “notify users.” This is just one of several healthcare-related study collaborations Apple is exploring. It is not known if Apple is looking to collaborate with medical laboratories. (Photo copyright: Apple.)
Apple’s History with Healthcare Related Technology
Taken as a single event, these speculations might not convince industry leaders. However, Apple’s long-term investments and acquisitions show a clear trend toward integrating healthcare data into the Apple ecosystem.
Healthcare IT News noted that from 2014 to 2017 Apple:
· Unveiled three different APIs—HealthKit, ResearchKit, and CareKit—designed to help capture, analyze, communicate, and integrate healthcare data with the Apple iOS and watchOS ecosystems;
· Hired several MDs, including: Stephen Friend, MD; Rajiv Kumar, MD; Mike Evans, MD; Ricky Bloomfield, MD; and Sumbul Ahmad Desai, MD; and,
· Engaged with the Argonaut Project and Health Gorilla (a centralized hub of healthcare data and information) suggesting a shift from wearables and basic device-based biometrics toward in-depth reporting, interoperability, and access to third-party healthcare data repositories—such as those in a person’s EHR or medical laboratory portal.
The Future of EHRs or Another Failed Attempt at Innovation?
Apple isn’t the only company to attempt such a system. Other efforts include Microsoft’s Health Vault and Google’s now shuttered Google Health. Another CNBC article notes that Amazon is also researching healthcare related options. “The new team is currently looking at opportunities that involve pushing and pulling data from legacy electronic medical record systems,” stated Farr. “The group is also exploring health applications for existing Amazon hardware, including Echo and Dash Wand.”
However, where most services fail to gain traction is user engagement. After all, if a system isn’t widely used or fails to offer benefits over existing systems, patients and service providers are not likely to go through the process of switching systems. Speaking with CNBC, Micky Tripathi, President and CEO of the Massachusetts eHealth Collaborative notes, “At any given time, only about 10% to 15% of patients care about this stuff. If any company can figure out engagement, it’s Apple.”
According to comScore, 85.8-million people over the age of 13 already own an iPhone in the US. The upcoming facial recognition features on Apple’s iPhone X might also provide the added security needed for those questioning the safety of their data. Should Apple succeed, communicating data between clinical laboratories, physicians, and patients might be both convenient and fast. More importantly, it might be the universal platform that finally provides health data access across the entire care continuum, while simultaneously improving access to providers and empowering healthcare consumers.
Of course, this is a few years from reality. But, we can speculate … would innovative medical laboratories have their patients’ lab test data hosted in the Cloud in such a way that patients and providers could access it securely, along with other protected clinical records?
Imagine how this would enable patients to have their complete medical record traveling with them at all times.
—Jon Stone
Related Information:
Could Apple Be Taking a Bite Out of EHRs?
Could Amazon or Apple Actually Make a Dent In the EHR Market?
Apple Extends Its Reach into Healthcare
Electronic device that computes health data
Apple Is Quietly Working on Turning Your iPhone Into the One-Stop Shop for All Your Medical Info
Wait! What? Amazon and Apple Eye Building EHRs
Apple Is Working with This Small Start-Up to Change How We Track Our Health
Timeline: How Apple Is Piecing Together Its Secret Healthcare Plan
Amazon Has a Secret Health Tech Team Called 1492 Working on Medical Records, Virtual Doc Visits
With Apple Consulting Argonaut Project on Health Records, Interoperability Could Get the Push It Needs
Apple Enlists Help of Startup Health Gorilla to Add Diagnostic Data to iPhones



