Cerner and Epic are the industry’s revenue leaders, though smaller vendors remain popular with physician groups
Sales of electronic health record (EHR) systems and related hardware and services reached $31.5 billion in 2018. And those sales will increase, according to a 2019 market analysis from Kalorama Information. This is important information for clinical laboratories and anatomic pathology groups that must interface with the EHRs of their physician clients to enable electronic transmission of lab orders and test results between doctor and lab.
Kalorama’s ranking includes familiar big EHR manufacturer names—Cerner (NASDAQ:CERN) and Epic—and includes a new name, Change Healthcare, which was born out of Change Healthcare Holding’s merger with McKesson. However, smaller EHR vendors remain popular with many independent physicians.
“We estimate that 40% of the market is not in the top 15 [in total revenue rankings],” said Bruce Carlson, Kalorama’s publisher, in an exclusive interview with Dark Daily. “There’s a lot of room. There are small vendors out there—Amazing Charts, e-MDs, Greenway, NextGen, Athena Health—that show up on a lot of physician surveys.”
“The EHR is really important,” noted Bruce Carlson (above), Publisher at Kalorama. “Since there are a variety of systems—sometimes different from the LIS [laboratory information management system]—you want to make sure you know the vendors and the space.” Carlson says opportunities remain for new entrants in the 700-plus competitor space, which is expected to see continued mergers and acquisitions that will affect clinical laboratories and their client physicians. (Photo copyright: Twitter.)
Interoperability a Key Challenge, as Most Medical
Laboratories Know
Interoperability—or the lack thereof—remains one of the
industry’s biggest challenges. For pathologists, that means seamless electronic
communication between medical laboratories and provider hospitals can be
elusive and can create a backlash against EHR vendors.
Kalorama notes a joint investigation by Fortune and Kaiser Health News (KHN), titled, “Death by a Thousand Clicks: Where Electronic Health Records Went Wrong.” The report details the growing number of medical errors tied to EHRs. One instance involved a California lawyer with herpes encephalitis who allegedly suffered irreversible brain damage due to a treatment delay caused by the failure of a critical lab test order to reach the hospital laboratory. The order was typed into the EHR, but the hospital’s software did not fully interface with the clinical laboratory’s software, so the lab did not receive the order.
“Many software vendors and LIS systems were in use prior to
the real launching of EHRs—the [federal government] stimulus programs,” Carlson
told Dark Daily. “There are a lot of legacy systems that aren’t
compatible and don’t feed right into the EHR. It’s a work in progress.”
Though true interoperability isn’t on the immediate horizon, Carlson expects its arrival within the next five years as the U.S. Department of Health and Human Services ramps up pressure on vendors.
“I think it is going to be a simple matter eventually,” he
said. “There’s going to be much more pressure from the federal government on
this. They want patients to have access to their medical records. They want one
record. That’s not going to happen without interoperability.”
Other common criticisms of EHRs include:
Wasted provider time: a recent study published in JAMA Internal Medicine notes providers now spend more time in indirect patient care than interacting with patients.
Physician burnout: EHRs have been shown to increase physician stress and burnout.
Not worth the trouble: The debate continues over whether EHRs are improving the quality of care.
Negative patient outcomes: Fortune’s investigation outlines patient safety risks tied to software glitches, user errors, or other flaws.
There’s No Going Back
Regardless of the challenges—and potential dangers—it appears EHRs are here to stay. “Any vendor resistance of a spirited nature is gone. Everyone is part of the CommonWell Health Alliance now,” noted Carlson.
Clinical laboratories and pathology groups should expect
hospitals and health networks to continue moving forward with expansion of
their EHRs and LIS integrations.
“Despite the intensity of attacks on EHRs, very few health systems are going back to paper,” Carlson said in a news release. “Hospital EHR systems are largely in place, and upgrades, consulting, and vendor switches will fuel the market.”
Thus, it behooves clinical laboratory managers and
stakeholders to anticipate increased demand for interfaces to hospital-based
healthcare providers, and even off-site medical settings, such as urgent care
centers and retail health clinics.
According to Damo Consulting’s 2019 Healthcare
IT Demand Survey, when it comes to spending money on information
technology (IT), healthcare executives believe AI and digital healthcare
technologies—though promising—need more development.
Damo’s report notes that 71% of healthcare providers
surveyed expect their IT budgets to grow by 20% in 2019. However, much of that
growth will be allocated to improving EHR functionality, Healthcare Purchasing News reported
in its analysis of Damo survey data.
As healthcare executives plan upgrades to their EHRs,
hospital-based medical laboratories will need to take steps to ensure
interoperability, while avoiding disruption to lab workflow during transition.
The survey also noted that some providers that are considering
investing in AI and digital health technology are struggling to understand the
market, the news release states.
“Digital and AI are emerging as critical areas for technology spend among healthcare enterprises in 2019. However, healthcare executives are realistic about their technology needs versus their need to improve care delivery. They find the currently available digital health solutions in the market are not very mature,” explained Paddy Padmanabhan (above), Chief Executive Officer of Damo Consulting, in a news release. (Photo copyright: The Authors Guild.)
Providers More
Positive Than Vendors on IT Spend
Damo Consulting is a Chicago-area based healthcare and
digital advisory firm. In November 2018, Damo surveyed 64 healthcare executives
(40 technology and service leaders, and 24 healthcare enterprise executives). Interestingly, healthcare providers were more
positive than the technology developers on IT spending plans, reported HITInfrastructure.com, which
detailed the following survey findings:
79% of healthcare executives anticipate high
growth in IT spending in 2019, but only 60% of tech company representatives
believe that is so.
75% of healthcare executives and 80% of vendor
representatives say change in healthcare IT makes buying decisions harder.
71% of healthcare executives and 55% of vendors say
federal government policies help IT spending.
50% of healthcare executives associate
immaturity with digital solution offerings.
42% of healthcare providers say they lack
resources to launch digital.
“While information technology vendors are aggressively
marketing ‘digital’ and ‘AI,’ healthcare executives note that the currently
available solutions in these areas are not very mature. These executives are
confused by the buzz around ‘AI’ and ‘digital,’ the changing landscape of who
is playing what role, and the blurred lines of capabilities and competition,” noted
Padmanabhan in the survey report.
The survey also notes that “Health systems are firmly
committed to their EHR vendors. Despite the many shortcomings, EHR systems
appear to be the primary choice for digital initiatives among health systems at
this stage.”
Some Healthcare
Providers Starting to Use AI
Even as EHRs receive the lion’s share of healthcare IT
spends, some providers are devoting significant resources to AI-related
projects and processes.
For example, clinical
pathologists may be intrigued by work being conducted at Cleveland Clinic’s Center for
Clinical Artificial Intelligence (CCAI), launched in March. The CCAI is using
AI and machine learning in pathology, genetics, and cancer research, with the
ultimate goal of improving patient outcomes, reported Becker’s Hospital Review.
“We’re not in it because AI is cool, but because we believe
it can advance medical research and collaboration between medicine and
industry—with a focus on the patient,” Aziz Nazha, MD, Clinical
Hematology and Oncology Specialist and Director of the CCAI, stated in an
article posted by the American Medical Association (AMA).
AI Predictions Lower
Readmissions and Improve Outcomes
Cleveland Clinic’s CCAI reportedly has gathered data from
1.6 million patients, which it uses to predict length-of-stays and reduce
inappropriate readmissions. “But a prediction itself is insufficient,” Nazha told
the AMA. “If we can intervene, we can change the prognosis and make things
better.”
The CCAI’s ultimate goal is to use predictive models to “develop
a new generation of physician-data scientists and medical researchers.” Toward
that end, Nazha notes how his team used AI to develop genomic biomarkers that identify
whether a certain chemotherapy drug—azacitidine (aka,
azacytidine and marketed as Vidaza)—will work for specific patients. This is a
key goal of precision
medicine.
CCAI also created an AI prediction model that outperforms
existing prognosis scoring systems for patients with Myelodysplastic
syndromes (MDS), a form of cancer in bone marrow.
Meanwhile, at Johns
Hopkins Hospital, AI applications track availability of beds and more. The
Judy Reitz Capacity Command Center, built in collaboration with GE Healthcare Partners, is a
5,200 square feet center outfitted with AI apps and staff to transfer patients
and help smooth coordination of services, according to a news release.
Forbes described the Reitz command
center as a “cognitive hospital” and reports that it has essentially enabled
Johns Hopkins to expand its capacity by 16 beds without undergoing bricks-and-mortar-style
construction.
In short, medical laboratory leaders may want to interact
with IT colleagues to ensure uninterrupted workflows as EHR functionality evolves.
Furthermore, AI developments suggest opportunities for clinical laboratories to
leverage patient data and assist in improving the diagnostic accuracy of providers
in ways that improve patient care.
Despite the widespread adoption of electronic health record (EHR) systems and billions in government incentives, lack of interoperability still blocks potential benefits of digital health records, causing frustration among physicians, medical labs, and patients
Clinical laboratories and anatomic pathology groups understand the complexity of today’s electronic health record (EHR) systems. The ability to easily and securely transmit pathology test results and other diagnostic information among multiple providers was the entire point of shifting the nation’s healthcare industry from paper-based to digital health records. However, despite recent advances, true interoperability between disparate health networks remains elusive.
One major reason for the current situation is that multi-hospital health systems and health networks still use EHR systems from different vendors. This fact is well-known to the nation’s medical laboratories because they must spend money and resources to maintain electronic lab test ordering and resulting interfaces with all of these different EHRs.
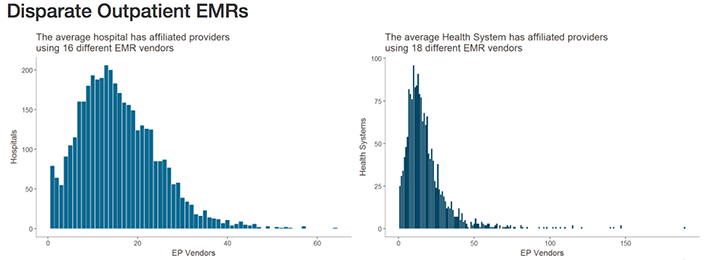
Healthcare IT News highlighted the scale of this problem in recent coverage. Citing data from the Healthcare Information and Management Systems Society (HIMSS) Logic database, they note that—when taking into account affiliated providers—the typical health network engages with as many as 18 different electronic medical record (EMR) vendors. Similarly, hospitals may be engaging with as many as 16 different EMR vendors.
The graphics above illustrates why interoperability is the most important hurdle facing healthcare today. Although the shift to digital is well underway, medical laboratories, physicians, and patients still struggle to communicate data between providers and access it in a universal or centralized manner. (Images copyright: Healthcare IT News.)
The lack of interoperability forces healthcare and diagnostics facilities to develop workarounds for locating, transmitting, receiving, and analyzing data. This simply compounds the problem.
Pressure from Technology Giants Fuels Push for Interoperability
According to HITECH Answers, the Centers for Medicare and Medicaid Services (CMS) has paid out more than $38-billion in EHR Incentive Program payments since April 2018.
Experts, however, point out that government incentives are only one part of the pressure vendors are seeing to improve interoperability.
“There needs to be a regulatory push here to play referee and determine what standards will be necessary,” Blain Newton, Executive Vice President, HIMSS Analytics, told Healthcare IT News. “But the [EHR] vendors are going to have to do it because of consumer demand, as things like Apple Health Records gain traction.”
Another solution, according to TechTarget, involves developing application programming interfaces (APIs) that allow tech companies and EHR vendors to achieve better interoperability by linking information in a structured manner, facilitating secure data transmission, and powering the next generation of apps that will bring interoperability ever closer to a reality.
TechTarget reported on how University of Utah Hospital’s five hospital/12 community clinic health network, and Intermountain Healthcare, also in Utah, successfully used APIs to develop customized interfaces and apps to improve accessibility and interoperability with their Epic and Cerner EHR systems.
Diagnostic Opportunities for Clinical Laboratories
As consumers gain increased access to their data and healthcare providers harness the current generation of third-party tools to streamline EHR use, vendors will continue to feel pressure to make interoperability a native feature of their EHR systems and reduce the need to rely on HIT teams for customization.
For pathology groups, medical laboratories, and other diagnosticians who interact with EHR systems daily, the impact of interoperability is clear. With the help of tech companies, and a shift in focus from government incentives programs, improved interoperability might soon offer innovative new uses for PHI in diagnosing and treating disease, while further improving the efficiency of clinical laboratories that face tightening budgets, reduced reimbursements, and greater competition.
Future EHRs will focus on efficiency, machine learning, and cloud services—improving how physicians and medical laboratories interact with the systems to support precision medicine and streamlined workflows
When the next generation of electronic health record (EHR) systems reaches the market, they will have advanced features that include cloud-based services and the ability to collect data from and communicate with patients using mobile devices. These new developments will provide clinical laboratories and anatomic pathology groups with new opportunities to create value with their lab testing services.
Proposed Improvements and Key Trends
Experts with EHR developers Epic Systems, Allscripts, Accenture, and drchrono spoke recently with Healthcare IT News about future platform initiatives and trends they feel will shape their next generation of EHR offerings.
They include:
Automation analytics and human-centered designs for increased efficiency and to help reduce physician burnout;
Improved feature parity across mobile and computer EHR interfaces to provide patients, physicians, and medical laboratories with access to information across a range of technologies and locations;
A shift toward cloud-hosted EHR solutions with support for application programming interfaces (APIs) designed for specific healthcare facilities that reduce IT overhead and make EHR systems accessible to smaller practices and facilities.
Should these proposals move forward, future generations of EHR platforms could transform from simple data storage/retrieval systems into critical tools physicians and medical laboratories use to facilitate communications and support decision-making in real time.
And, cloud-based EHRs with access to clinical labs’ APIs could enable those laboratories to communicate with and receive data from EHR systems with greater efficiency. This would eliminate yet another bottleneck in the decision-making process, and help laboratories increase volumes and margins through reduced documentation and data management overhead.
Cloud-based EHRs and Potential Pitfalls
Cloud-based EHRs rely on cloud computing, where IT resources are shared among multiple entities over the Internet. Such EHRs are highly scalable and allow end users to save money by hiring third-party IT services, rather than maintaining expensive IT staff.
Kipp Webb, MD, provider practice lead and Chief Clinical Innovation Officer at Accenture told Healthcare IT News that several EHR vendors are only a few years out on releasing cloud-based inpatient/outpatient EHR systems capable of meeting the needs of full-service medical centers.
While such a system would mean existing health networks would not need private infrastructure and dedicate IT teams to manage EHR system operations, a major shift in how next-gen systems are deployed and maintained could lead to potential interoperability and data transmission concerns. At least in the short term.
Yet, the transition also could lead to improved flexibility and connectivity between health networks and data providers—such as clinical laboratories and pathologist groups. This would be achieved through application programming interfaces (APIs) that enable computer systems to talk to each other and exchange data much more efficiently.
“Perhaps one of the biggest ways having a fully cloud-based EHR will change the way we as an industry operate will be enabled API access.” Daniel Kivatinos, COO and founder of drchrono, told Healthcare IT News. “You will be able to add other partners into the mix that just weren’t available before when you have a local EHR install only.”
Paul Black, CEO of Allscripts, believes these changes will likely require more than upgrading existing software or hardware. “The industry needs an entirely new approach to the EHR,” he told Healthcare IT News. “We’re seeing a huge need for the EHR to be mobile, cloud-based, and comprehensive to streamline workflow and get smarter with every use.” (Photo copyright: Allscripts.)
Reducing Physician Burnout through Human-Centered Design
As Dark Daily reported last year, EHRs have been identified as contributing to physician burnout, increased dissatisfaction, and decreased face-to-face interactions with patients.
Combined with the increased automation, Carl Dvorak, President of Epic Systems, notes next-gen EHR changes hold the potential to streamline the communication of orders, laboratory testing data, and information relevant to patient care. They could help physicians reach treatment decisions faster and provide laboratories with more insight, so they can suggest appropriate testing pathways for each episode of care.
“[Automation analytics] holds the key to unlocking some of the secrets to physician well-being,” Dvorak told Healthcare IT News. “For example, we can avoid work being unnecessarily diverted to physicians when it could be better managed by others.”
Black echoes similar benefits, saying, “We believe using human-centered design will transform the way physicians experience and interact with technology, as well as improve provider wellness.”
Some might question the success of the first wave of EHR systems. Though primarily built to address healthcare reform requirements, these systems provided critical feedback and data to EHR developers focused not on simply fulfilling regulatory requirements, but on meeting the needs of patients and care providers as well.
If these next-generations systems can help improve the quality of data recording, storage, and transmission, while also reducing physician burnout, they will have come a long way from the early EHRs. For medical laboratory professionals, these changes will likely impact how orders are received and lab results are reported back to doctors in the future. Thus, it’s worth monitoring these developments.
Both health systems will use their EHRs to track genetic testing data and plan to bring genetic data to primary care physicians
Clinical laboratories and pathology groups face a big challenge in how to get appropriate genetic and molecular data into electronic health record (EHR) systems in ways that are helpful for physicians. Precision medicine faces many barriers and this is one of the biggest. Aside from the sheer enormity of the data, there’s the question of making it useful and accessible for patient care. Thus, when two major healthcare systems resolve to accomplish this with their EHRs, laboratory managers and pathologists should take notice.
NorthShore University HealthSystem in Illinois and Geisinger Health System in Pennsylvania and New Jersey are working to make genetic testing part of primary care. And both reached similar conclusions regarding the best way for primary care physicians to make use of the information.
At NorthShore, two genetic testing programs—MedClueRx and the Genetic and Wellness Assessment—provide doctors with more information about how their patients metabolize certain drugs and whether or not their medical and family histories suggest they need further, more specific genetic testing.
“We’re not trying to make all of our primary care physicians into genomic experts. That is a difficult strategy that really isn’t scalable. But we’re giving them enough tools to help them feel comfortable,” Peter Hulick, MD, Director of the Center for Personalized Medicine at NorthShore, told Healthcare IT News.
Conversely, Geisinger has made genomic testing an automated part of primary care. When patients visit their primary care physicians, they are asked to sign a release and undergo whole genome sequencing. An article in For the Record describes Geisinger’s program:
“The American College of Medical Genetics and Genomics classifies 59 genes as clinically actionable, with an additional 21 others recommended by Geisinger. If a pathogenic or likely pathogenic variant is found in one of those 80 genes, the patient and the primary care provider are notified.”
William Andrew Faucett (left) is Director of Policy and Education, Office of the Chief Scientific Officer at Geisinger Health; and Peter Hulick, MD (right), is Director of the Center for Personalized Medicine at NorthShore University HealthSystem. Both are leading programs at their respective healthcare networks to improve precision medicine and primary care by including genetic testing data and accessibility to it in their patients’ EHRs. (Photo copyrights: Geisinger/NorthShore University HealthSystem.)
The EHR as the Way to Access Genetic Test Results
Both NorthShore and Geisinger selected their EHRs for making important genetic information accessible to primary care physicians, as well as an avenue for tracking that information over time.
Hulick told Healthcare IT News that NorthShore decided to make small changes to their existing Epic EHR that would enable seemingly simple but actually complex actions to take place. For example, tracking the results of a genetic test within the EHR. According to Hulick, making the genetic test results trackable creates a “variant repository,” also known as a Clinical Data Repository.
“Once you have that, you can start to link it to other information that’s known about the patient: family history status, etc.,” he explained. “And you can start to build an infrastructure around it and use some of the tools for clinical decision support that are used in other areas: drug/drug interactions, reminders for flu vaccinations, and you can start to build on those decision support tools but apply them to genomics.”
Like NorthShore, Geisinger is also using its EHR to make genetic testing information available to primary care physician when a problem variant is identified. They use EHR products from both Epic and Cerner and are working with both companies to streamline and simplify the processes related to genetic testing. When a potentially problematic variant is found, it is listed in the EHR’s problem list, similar to other health issues.
Geisinger has developed a reporting system called GenomeCOMPASS, which notifies patients of their results and provides related information. It also enables patients to connect with a geneticist. GenomeCOMPASS has a physician-facing side where primary care doctors receive the results and have access to more information.
Andrew Faucett, Senior Investigator (Professor) and Director of Policy and Education, Office of the Chief Scientific Officer at Geisinger, compares the interpretation of genetic testing to any other kind of medical testing. “If a patient gets an MRI, the primary care physicians doesn’t interpret it—the radiologist does,” adding, “Doctors want to help patients follow the recommendations of the experts,” he told For the Record.
The Unknown Factor
Even though researchers regularly make new discoveries in genomics, physicians practicing today have had little, if any, training on how to incorporate genetics into their patients’ care. Combine that lack of knowledge and training with the current lack of EHR interoperability and the challenges in using genetic testing for precision medicine multiply to a staggering degree.
One thing that is certain: the scientific community will continue to gather knowledge that can be applied to improving the health of patients. Medical pathology laboratories will play a critical role in both testing and helping ensure results are useful and accessible, now and in the future.